Applied Surgical Anatomy of the Leg— Approaches for Decompression of a Compartment Syndrome
Overview
The tibia and fibula are very different bones. The tibia has a large subcutaneous surface that allows access to the bone along its entire length; the fibula is enclosed almost completely in muscle. Only at its proximal end and in the lower third of the bone does the fibula develop a subcutaneous surface, which terminates in the lateral malleolus. For this reason, operations on most of the fibula almost always involve extensive stripping of muscle off bone. In addition, the tibia has no major
neurovascular structures running directly on it other than its nutrient artery; the fibula has close ties to the common peroneal nerve and its branches.
The deep fascia of the leg is a tough, fibrous, unyielding structure that encloses the calf muscles. Where the bones become subcutaneous, the fascia usually is attached to the border of the bone.
Two intermuscular septa, one anterior and one posterior, pass from the deep surface of the encircling fascia to the fibula and enclose the peroneal or lateral compartment of the leg.
Four separate muscular compartments exist in the lower leg (Fig. 11-48).
Anterior (Extensor) Compartment
The anterior compartment contains the extensor muscles of the foot and ankle. Its medial boundary is the lateral (extensor) surface of the tibia, and its lateral boundary is the extensor surface of the fibula and anterior intermuscular septum. The anterior compartment is enclosed by the deep fascia of the leg and all its muscles are supplied by the deep peroneal nerve. The compartment’s artery is the anterior tibial artery (Fig. 11-49).
 |
 |
 |
 |
Figure 11-48 The fibro-osseous compartments of the leg.
Lateral (Peroneal) Compartment
The peroneal compartment is bounded by the anterior intermuscular septum in front, by the posterior intermuscular septum behind, and by the fibula medially. It contains the peroneal muscles which evert the foot. The superficial peroneal nerve supplies all the muscles in the compartment. No artery runs in it; its muscles receive their supply from several branches of the peroneal artery (Fig. 11-50).
Superficial Posterior (Flexor) Compartment
The superficial flexor compartment contains three muscles: the
gastrocnemius, soleus, and plantaris. The compartment is separated from the lateral (peroneal compartment) by the posterior intermuscular septum. It is separated from the deep posterior flexor compartment by a fascial layer.
Deep Posterior Flexor Compartment
The deep posterior flexor compartment contains three muscles: the tibialis posterior, flexor hallucis longus, and flexor digitorum longus. It also contains the tibial nerve and posterior tibial artery. It is separated from the superficial flexor compartment by the posterior intermuscular septum and from the anterior compartment by the interosseous membrane.
Surgical Approaches for Decompression of Lower Leg Compartment Syndrome
The details of pathophysiology and diagnosis of an acute compartment syndrome are beyond the scope of this book but the authors believe that diagnosis is still mainly clinical and that routine decompression of all four compartments is the current gold standard in treatment in the absence of strong evidence that a compartment is not involved. Two approaches are described which will allow adequate decompression of all four compartments.
 |
 |
 |
 |
 |
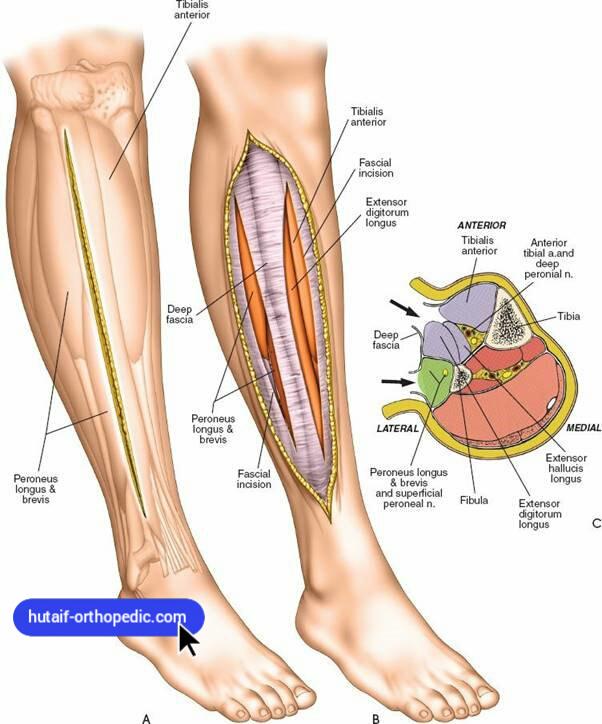
Figure 11-49 To decompress the anterior and lateral compartments, make a longitudinal incision overlying the anterolateral aspect of the lower leg. A: Begin at the level of the tibial tubercle and extend the incision to end 6 cm above the level of the ankle. B: Incise the fascia overlying the anterior and lateral compartments in the line of the skin incision. C: Transverse section showing the fascial compartments. Incising the fascia overlying the anterior, lateral, and superficial flexor compartments is easy. Decompressing the deep flexor compartment may involve lifting the soleus muscle of the intermuscular septum and dividing that septum under direct vision, taking care to avoid the posterior
neurovascular bundle.
 |
 |
 |
 |
Figure 11-50 To decompress the superficial and deep flexor compartments, make a longitudinal incision overlying the posteromedial aspect of the lower leg. Begin at the level of the tibial tubercle and extend the incision distally, ending 6 cm above the ankle. At right, transverse section showing the fascial compartments. Incising the fascia overlying the anterior, lateral, and superficial flexor compartments is easy. Decompressing the deep flexor compartment may involve lifting the soleus muscle of the intermuscular septum and dividing that septum under direct vision, taking care to avoid the posterior neurovascular bundle.
Position of the Patient
Place the patient supine on the operating table. The use of a tourniquet is clearly contraindicated (see Fig. 11-28).
Landmarks and Incisions
Palpate the tibial tubercle on the anterior aspect of the proximal tibia and the lateral and medial malleoli at the level of the ankle.
Anterolateral Incision
Make a longitudinal incision overlying the anterolateral aspect of the lower leg (see Fig. 11-49A). Begin at the level of the tibial tubercle and extend the incision to end 6 cm above the level of the ankle.
Posteromedial Incision
Make a longitudinal incision overlying the posteromedial aspect of the lower leg (see Fig. 11-50). Begin at the level of the tibial tubercle and extend the incision distally ending 6 cm above the ankle.
Superficial Surgical Dissection
To decompress the anterior and lateral compartments incise the fascia overlying the anterior and lateral compartments in the line of the skin incision (Fig. 11-49B). Two separate incisions are required. Ensure that the fascial incision extends the full length of the skin incision.
To decompress the superficial and deep flexor compartments incise the deep fascia in line with the skin incision to expose the soleus muscle. To decompress the deep flexor compartment lift the soleus muscle off the intermuscular septum and divide the septum under direct vision, taking care to avoid the posterior neurovascular bundle which lies just beneath it (Fig. 11-50). Figure 11-48 shows a transverse section of the leg illustrating the fascial compartments.
Dang
The posterior neurovascular bundle is at risk if the fascia covering the deep flexor compartment is not divided carefully. The main danger of the approach is however inadequate decompression. A compartment syndrome in not an indication for minimally invasive surgery.
