Young Femoral Fracture: Essential Management & Surgical Decisions
Introduction & Epidemiology
Femoral shaft fractures in young adults represent a significant orthopaedic challenge, predominantly resulting from high-energy trauma such as motor vehicle collisions, motorcycle accidents, or falls from height. These injuries are often isolated but frequently associated with polytrauma, necessitating a comprehensive Advanced Trauma Life Support (ATLS) assessment to identify and manage concomitant injuries to the head, chest, abdomen, pelvis, or other extremities.
The incidence of femoral shaft fractures peaks in young males due to their higher involvement in high-velocity activities. The robust bone quality in this demographic means that substantial force is required to induce fracture, often leading to significant soft tissue injury, substantial blood loss (potentially 1-1.5 liters internally), and a higher risk of complications. The primary goals of management are anatomical reduction, stable fixation, restoration of limb length and alignment, early mobilization, and minimizing long-term disability, including non-union, malunion, and chronic pain. The choice of surgical technique is paramount for achieving these objectives and is largely dictated by fracture morphology, location, associated injuries, and the patient's physiological status.
Surgical Anatomy & Biomechanics
A thorough understanding of femoral anatomy and biomechanics is critical for effective surgical planning and execution. The femur is the longest and strongest bone in the human body, designed to withstand significant compressive, tensile, and torsional forces.
Surgical Anatomy
- Femoral Diaphysis: Characterized by its anterior convexity (bowing) and the presence of the linea aspera, a prominent posterior ridge that serves as an attachment for adductor, hamstring, and vastus muscles. The medullary canal is narrowest in the mid-diaphysis and widens proximally and distally.
- Proximal Femur: The greater trochanter serves as a critical entry point for antegrade intramedullary nailing. The lesser trochanter is the insertion site for the iliopsoas. The femoral neck-shaft angle typically averages 125-130 degrees, and the femoral neck anteversion averages 10-20 degrees; these parameters must be respected during reduction to prevent malrotation.
- Distal Femur: Characterized by the broad supracondylar flare, epicondyles, and the intricate articular surfaces of the femoral condyles, which articulate with the tibia to form the knee joint. The adductor tubercle and adductor hiatus are important landmarks for vascular bundles.
- Musculature: The femur is enveloped by powerful muscle groups. The quadriceps femoris (rectus femoris, vastus lateralis, medialis, intermedius) inserts into the patella. The hamstrings (biceps femoris, semitendinosus, semimembranosus) originate from the ischial tuberosity and insert distally around the knee. The adductor muscles originate from the pelvis. These muscles contribute significantly to fracture displacement patterns (e.g., flexion/abduction of the proximal fragment due to gluteus medius/minimus and iliopsoas with subtrochanteric fractures, or shortening due to quadriceps and hamstrings in midshaft fractures).
- Neurovascular Structures: The femoral artery and vein, along with the femoral nerve, are anterior in the groin. The deep femoral artery and its perforating branches supply the femoral diaphysis; these are at risk during extensive subperiosteal dissection. The sciatic nerve courses posteriorly in the thigh, vulnerable during posterior approaches or with severe posterior fracture displacement.
Biomechanics
The femur experiences complex loading during ambulation, with peak forces reaching 3-5 times body weight. Torsional stability is primarily provided by intramedullary fixation or bicortical screw purchase. The intrinsic anterior bow of the femur must be considered during intramedullary nail selection and insertion to prevent iatrogenic fracture or anterior cortical impingement. The goal of fixation is to neutralize these deforming forces, allowing for biological healing and early functional recovery. IMN acts as a load-sharing device, whereas plate osteosynthesis is typically load-bearing, influencing weight-bearing protocols.
Indications & Contraindications
Operative Indications (Nearly Universal in Young Adults)
The vast majority of femoral shaft fractures in young, physiologically stable adults are managed operatively.
- Displaced, unstable femoral shaft fractures: This includes most mid-diaphyseal, subtrochanteric, and distal metaphyseal fractures.
- Open fractures: Require urgent debridement and stabilization.
- Polytrauma patients: Early surgical stabilization of the femur (within 24 hours in hemodynamically stable patients) is critical for resuscitation, reducing pain, decreasing pulmonary complications (e.g., fat embolism syndrome), and facilitating nursing care. This is often termed "early appropriate care."
- Vascular injury: Requiring repair; stabilization of the femur facilitates vascular reconstruction.
- Floating knee injury: Concomitant ipsilateral femoral and tibial fractures. Early stabilization of both bones is crucial.
- Pathological fractures: Secondary to tumors (primary or metastatic); require specific oncological considerations for fixation and adjuvant therapy.
- Ipsilateral acetabular, pelvic, or spinal fractures: To facilitate patient positioning and rehabilitation for associated injuries.
- Obesity: Extremely challenging to manage non-operatively.
- Fractures with significant soft tissue compromise: May benefit from initial external fixation, followed by definitive fixation once soft tissues improve.
Non-Operative Indications (Rare in Young Adults)
Non-operative management of femoral shaft fractures in young adults is exceedingly rare and generally reserved for specific, unusual circumstances.
- Physiological instability: Severe comorbidities or polytrauma where the patient cannot tolerate surgery; temporary external fixation may be applied as a damage control measure.
- Severe local soft tissue compromise: Such as extensive degloving injuries or severe contamination where immediate definitive internal fixation would be ill-advised; external fixation or traction may be used as a temporary measure.
- Minimal displacement/stress fractures: A rare subset, not typically considered traumatic femoral shaft fractures in the acute sense.
Contraindications (Relative & Temporary)
- Uncontrolled hemorrhage or profound shock: Requires resuscitation and stabilization prior to definitive surgery (Damage Control Orthopaedics principles apply).
- Active systemic infection (sepsis): Needs to be controlled.
- Severe burns: Over the operative site, requiring staged management.
- Unmanageable anesthetic risk: Requires medical optimization.
Summary Table: Operative vs. Non-Operative Indications
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Fracture Pattern | Displaced, unstable diaphyseal, metaphyseal fractures | Minimally displaced stress fractures (rarely traumatic acute fractures) |
| Associated Injuries | Polytrauma, open fractures, vascular injury, floating knee | N/A |
| Patient Physiology | Physiologically stable, suitable for surgery | Physiologically unstable (temporary external fixation may be used) |
| Soft Tissue Status | Adequate soft tissue envelope | Severe soft tissue compromise (temporary external fixation) |
| Specific Conditions | Pathological fractures, ipsilateral pelvic/spinal trauma | N/A |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is crucial to optimize outcomes and minimize complications.
Pre-Operative Planning
- Patient Assessment & Resuscitation: Adherence to ATLS protocols. Full secondary survey to identify all injuries. Haemodynamic stability is paramount.
-
Imaging:
- Plain Radiographs: AP and lateral views of the entire femur, including the hip and knee joints, are essential to fully characterize the fracture, identify associated injuries, and assess alignment.
- CT Scan: Useful for complex fracture patterns (e.g., comminution, articular involvement), especially in the proximal and distal femur, and for evaluation of concomitant pelvic, acetabular, or spinal injuries.
- Angiography: If vascular injury is suspected.
-
Timing of Surgery:
- Early Appropriate Care (EAC): In polytrauma patients, definitive fixation within 24-48 hours, once the patient is physiologically optimized, is associated with better outcomes.
- Damage Control Orthopaedics (DCO): For hemodynamically unstable patients or those with severe associated injuries, initial external fixation (spanning the knee, hip, or both) may be performed as a life-saving measure, with definitive internal fixation delayed until the patient is stable ("fix and flap" or "fix and defer").
- Antibiotics & Tetanus: Prophylactic intravenous antibiotics are administered pre-operatively for closed fractures. Open fractures require broad-spectrum antibiotics and tetanus prophylaxis according to Gustilo-Anderson classification.
- Anesthesia: General anesthesia is typically employed. Regional nerve blocks (e.g., femoral nerve block) can aid in post-operative pain control.
-
Implant Selection:
Based on fracture pattern, location, and surgeon preference.
- Intramedullary Nailing (IMN): Gold standard for most diaphyseal fractures. Nailing diameter and length are critical. Pre-operative templating from contralateral femur radiographs can assist.
- Plate Osteosynthesis: Primarily for articular or highly metaphyseal fractures, or fractures with significant canal distortion where IMN is not feasible.
- External Fixation: For temporary stabilization or definitive fixation in specific open fractures.
Patient Positioning
Patient positioning depends on the chosen surgical approach (antegrade vs. retrograde IMN, or plating) and the available equipment (fracture table vs. radiolucent table).
-
Supine on Fracture Table:
- Advantages: Allows for closed reduction via traction, provides excellent stability, and frees the surgical team for other tasks.
- Disadvantages: Fixed hip abduction/flexion can make entry point access challenging for antegrade nailing. Malrotation can be difficult to assess.
- Preparation: The injured leg is placed in boot traction. The contralateral leg is typically flexed and abducted to allow access for the C-arm for AP imaging of the injured hip and knee. The torso may be slightly tilted. Ensure adequate padding to prevent pressure injuries.
-
Supine on Radiolucent Table with Leg Holder/Beach Chair:
- Advantages: Allows for free manipulation of the limb, easier assessment of rotation, and versatility for both antegrade and retrograde nailing (with appropriate drapes).
- Disadvantages: Requires manual traction/reduction, potentially increasing operative time and radiation exposure.
- Preparation: The patient is positioned supine. The injured limb is typically free-draped, often with a sterile thigh support or a well-padded bolster under the knee to facilitate knee flexion for retrograde nailing.
- Lateral Decubitus: Less common but can be used for specific plating approaches, especially for the proximal femur.
- C-arm Access: Ensure unrestricted C-arm access for AP and lateral views of the entire femur, including hip and knee joints. This is crucial for confirming reduction, guide wire placement, reaming, and locking screw insertion.
Detailed Surgical Approach / Technique
Intramedullary nailing (IMN) is the gold standard for diaphyseal femoral fractures in young adults. Plate osteosynthesis is typically reserved for specific indications.
Intramedullary Nailing (IMN)
1. Antegrade Nailing (Standard Approach for Diaphyseal Fractures)
-
Entry Point Options:
- Piriformis Fossa: Historically common, but associated with increased risk of iatrogenic avascular necrosis of the femoral head due to disruption of the superior gluteal artery branches. Requires a more medial entry point, through the piriformis fossa.
- Tip of Greater Trochanter: Current preferred entry point. Directly in line with the femoral canal, minimizing angular mismatch and stress risers. Accessed through the vastus lateralis, splitting the gluteus medius fibers.
- Greater Trochanteric Apex: A more lateral entry, through the vastus lateralis, suitable for fractures extending proximally.
- Patient Positioning: Supine on fracture table or radiolucent table. Traction is applied to achieve length.
-
Surgical Steps:
- Incision: Longitudinal incision (typically 3-5 cm) extending proximally from the tip of the greater trochanter, through skin and subcutaneous tissue.
- Muscle Split: Incise the fascia lata, then split the gluteus medius and vastus lateralis muscles longitudinally to expose the tip of the greater trochanter.
- Entry Reaming: Use an awl or drill to create an entry portal at the chosen trochanteric entry point. The entry should be in line with the medullary canal on both AP and lateral fluoroscopic views.
- Guide Wire Insertion: A ball-tipped guide wire is inserted through the entry portal, across the fracture site, and into the distal fragment. Ensure it is centrally placed in both fragments.
- Reaming (if indicated): Sequential reaming with flexible reamers is performed to the desired nail diameter. Reaming clears the canal, provides bone graft, and ensures intimate contact between the nail and endosteum for stability. Unreamed nailing may be considered in specific circumstances (e.g., patients at high risk for fat embolism, severe head injury) but provides less stable fixation.
- Nail Insertion: The appropriate length and diameter nail is selected. The nail is inserted over the guide wire, typically with a power driver, until the proximal end is flush with the trochanter. Fluoroscopy confirms proper depth.
- Distal Locking: Performed through an aiming device or freehand, using fluoroscopy to guide drill bits and locking screws through the nail's distal holes and into the distal fragment. Typically two screws for stability.
- Proximal Locking: Performed through the aiming jig for the proximal screws. Two screws are usually placed through the nail and into the proximal fragment. Dynamic vs. static locking depends on fracture stability and comminution.
- Guide Wire Removal & Closure: Remove the guide wire. Irrigate and close the wound in layers.
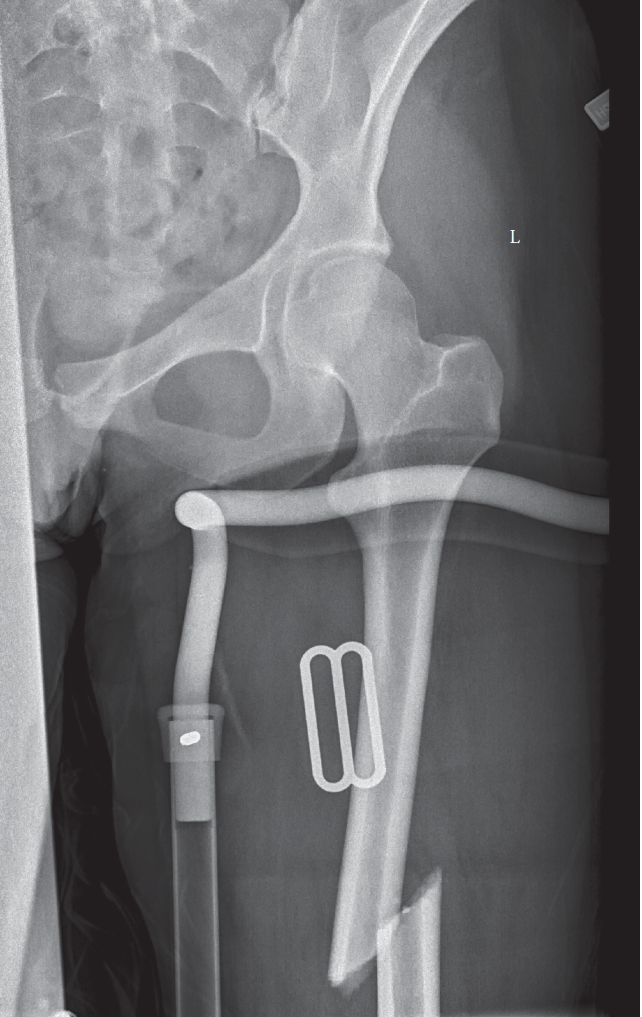
Figure 1: Intraoperative fluoroscopic image demonstrating antegrade intramedullary nailing. Note the guide wire across the fracture, reaming reamer inside the canal, and planned nail path. Proper alignment and central guide wire placement are critical for successful reduction and fixation.
2. Retrograde Nailing
- Indications: Distal femoral fractures, ipsilateral acetabular/pelvic/spinal fractures, floating knee injuries, morbid obesity, bilateral femur fractures, or when antegrade nailing is difficult (e.g., ipsilateral hip fracture).
- Patient Positioning: Supine on a radiolucent table with knee flexed (often with a knee bolster) to 90 degrees.
-
Surgical Steps:
- Incision: Longitudinal incision (typically 3-5 cm) just proximal to the patella, either paramedian or through the quadriceps tendon.
- Arthrotomy (if using transpatellar approach): An incision is made through the quadriceps tendon and patellar fat pad to expose the intercondylar notch. Care must be taken to avoid articular damage. Suprapatellar approaches are gaining favor to minimize patellofemoral pain.
- Entry Point: The entry point is located in the intercondylar notch, typically just anterior to Blumensaat's line, slightly medial or lateral to the midline depending on the nail's curvature.
- Guide Wire Insertion: A guide wire is inserted through the entry portal, across the fracture, and into the proximal fragment.
- Reaming & Nail Insertion: Similar to antegrade nailing, sequential reaming (if desired) is performed, followed by nail insertion.
- Locking: Proximal and distal locking screws are inserted through the nail.
- Closure: Close the quadriceps tendon, deep fascia, and skin layers.
Pearls & Pitfalls for IMN:
- Reduction: Achieving and maintaining reduction is paramount. Manual traction, external manipulators, and reduction clamps can assist.
- Rotation: Critical to restore normal femoral anteversion. Clinical assessment of foot rotation relative to the patella (with the knee flexed to 90 degrees) or comparison with the contralateral side is essential. Fluoroscopic "offset" views can help.
- Entry Point: Incorrect entry point can lead to malalignment, hardware impingement, or iatrogenic fracture.
- Nail Length/Diameter: Accurate measurement prevents prominent hardware, non-union, or iatrogenic fracture.
- Locking Screws: Ensure bicortical purchase for optimal stability.
Plate Osteosynthesis (ORIF)
- Indications: Distal or proximal articular fractures, highly comminuted metaphyseal fractures not amenable to IMN, fractures with significant canal deformity, pediatric fractures requiring physeal sparing, non-unions, or specific open fractures where IMN is contraindicated due to contamination.
-
Approaches:
- Lateral Approach (Distal Femur): Incision along the lateral aspect of the thigh, splitting the vastus lateralis to expose the lateral femoral shaft and condyle.
- Anterior Approach: Less common for shaft fractures, sometimes used for subtrochanteric fractures.
- Minimally Invasive Plate Osteosynthesis (MIPO): Small incisions proximally and distally, with the plate slid submuscularly. Preserves soft tissue and blood supply but makes direct reduction more challenging.
-
Surgical Steps (General for Lateral Plating):
- Incision & Exposure: A longitudinal incision along the lateral aspect of the distal femur. The fascia lata is incised, and the vastus lateralis is either retracted anteriorly or split longitudinally from its origin to expose the lateral femoral cortex.
- Reduction: Indirect reduction techniques are preferred to minimize soft tissue stripping. Traction, external manipulators, and percutaneous clamps can be used to restore length, alignment, and rotation. For articular fractures, direct visualization and reduction of the joint surface is critical.
- Plate Application: A pre-contoured locking compression plate (LCP) is typically used. The plate is applied to the lateral aspect of the femur. For diaphyseal fractures, bridge plating principles are often employed, with sufficient working length to span the comminuted zone. For articular fractures, anatomical reduction and lag screws followed by a buttress plate are common.
- Screw Insertion: Locking screws are inserted bicortically. Ensure adequate bone purchase and avoid articular penetration.
- Closure: Irrigate the wound and close in layers.

Figure 2: Lateral view of a distal femoral locking plate applied. This GIF would typically show the progressive application of the plate and screws, highlighting the importance of anatomical contouring and bicortical purchase for stable fixation, especially in metaphyseal fractures extending into the articular segment.
External Fixation
- Indications: Damage control in polytrauma, severe open fractures (Gustilo IIIB/IIIC), vascular repair, severe soft tissue compromise, burns, or impending compartment syndrome. Often a temporary measure prior to definitive IMN or ORIF.
- Technique: Pins are inserted into the safe corridors of the proximal and distal femur, respecting neurovascular structures. A rigid frame is constructed to stabilize the fracture.
Complications & Management
Femoral shaft fractures can be associated with a range of complications, both early and late. Proactive recognition and management are crucial for optimal outcomes.
Early Complications
- Hemorrhage/Vascular Injury: Significant blood loss can occur with the initial injury. Iatrogenic vascular injury (e.g., during reaming or screw placement) is rare but devastating. Management involves immediate control of bleeding and vascular repair.
- Nerve Injury: Sciatic nerve (posteriorly) or femoral nerve (anteriorly) damage can occur due to fracture displacement or iatrogenic causes. Careful clinical assessment pre- and post-operatively is essential.
- Fat Embolism Syndrome (FES): A potentially life-threatening complication, more common with reamed IMN, especially in polytrauma patients. Characterized by respiratory distress, cerebral dysfunction, and petechial rash. Management is supportive (oxygen, ventilation).
- Infection: Higher incidence with open fractures. Prophylactic antibiotics and meticulous surgical technique reduce risk in closed fractures. Management involves debridement, antibiotics, and possible hardware removal/exchange.
- Compartment Syndrome: Rare in the thigh, but vigilance is required, especially with high-energy trauma or extensive soft tissue injury. Diagnosis is clinical, confirmed by compartment pressure measurements. Management is urgent fasciotomy.
Late Complications
-
Non-Union:
Failure of the fracture to heal after an appropriate period (typically 6-9 months).
- Causes: Inadequate reduction, unstable fixation, infection, biological factors (e.g., extensive comminution, periosteal stripping, patient comorbidities).
- Incidence: Varies from 1-10% with IMN. Higher with plating.
- Salvage: Exchange nailing (for IMN non-unions), plate osteosynthesis with bone grafting, external fixation, or revision to a different IMN. Biological adjuncts (e.g., autologous bone graft, demineralized bone matrix, bone morphogenetic proteins) may be considered.
-
Malunion:
Healing of the fracture in an unacceptable position (e.g., rotational, angular, or shortening deformities).
- Causes: Inadequate reduction at the time of surgery, loss of reduction post-operatively. Rotational malunion is particularly problematic and often poorly tolerated by patients.
- Incidence: Up to 10-20% for rotational malunion, often underdiagnosed.
- Salvage: Corrective osteotomy and stable internal fixation (e.g., with plate or nail) once the fracture has united.
-
Hardware Failure:
Breakage or loosening of the nail/plate/screws, usually indicating a non-union or excessive stress on the implant.
- Salvage: Addressing the underlying non-union, often with revision surgery and new hardware.
-
Persistent Pain:
- Knee pain: Common after retrograde nailing (up to 50%), due to quadriceps irritation or entry point issues.
- Hip pain: Can occur after antegrade nailing due to prominent hardware or trochanteric bursitis.
- Salvage: Hardware removal (if symptomatic), physical therapy, corticosteroid injections.
-
Heterotopic Ossification (HO):
Ectopic bone formation in soft tissues, especially after extensive soft tissue trauma or in patients with head injuries.
- Incidence: Up to 10-20% in high-risk patients.
- Salvage: Prophylaxis (NSAIDs, radiation therapy in high-risk patients), surgical excision if functionally limiting after maturation.
-
Refracture:
After hardware removal, particularly if the bone has not fully remodeled or if hardware is removed too early.
- Prevention: Ensure radiographic signs of complete union and cortical remodeling before removal.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approx.) | Salvage Strategies |
|---|---|---|
| Early | ||
| Hemorrhage/Vascular Injury | <1% (iatrogenic) | Direct repair, ligation, graft interposition, embolization, fracture stabilization. |
| Nerve Injury | <1% | Observation, neurolysis, reconstruction (rarely needed if iatrogenic) |
| Fat Embolism Syndrome (FES) | 1-5% (clinical) | Supportive care, ventilatory support. |
| Infection (deep) | 1-2% (closed); 5-30% (open) | Debridement, irrigation, antibiotics, implant retention vs. removal, possible revision/exchange nailing. |
| Compartment Syndrome | <1% | Emergency fasciotomy. |
| Late | ||
| Non-union | 1-10% | Exchange nailing, revision plating with bone grafting, dynamization, external fixation, biological augmentation. |
| Malunion (rotational, angular, shortening) | 5-20% | Corrective osteotomy with internal fixation (plate or nail). |
| Hardware Failure | 2-5% | Address underlying non-union, revise hardware (exchange nail, new plate). |
| Persistent Pain (knee/hip) | Up to 50% (retrograde); 10-20% (antegrade) | Hardware removal, physical therapy, bursal injections. |
| Heterotopic Ossification (HO) | 10-20% (high risk) | Prophylaxis (NSAIDs/radiation), surgical excision after maturation if functionally limiting. |
| Refracture | <5% | Revision surgery with new fixation, potentially stronger implant; bone grafting if non-union component. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for restoring function, preventing stiffness, and ensuring successful recovery following a young femoral fracture. Protocols are tailored based on the stability of fixation, fracture pattern, and patient comorbidities.
Phase 1: Immediate Post-Operative (Days 0-7)
- Pain Management: Multimodal analgesia including opioids, NSAIDs, acetaminophen, and regional nerve blocks.
- Wound Care: Daily dressing changes, monitor for signs of infection.
- DVT Prophylaxis: Pharmacological (low molecular weight heparin) and mechanical (TED stockings, pneumatic compression devices) is crucial.
-
Weight-Bearing (WB):
- Intramedullary Nailing: Typically immediate weight-bearing as tolerated (WBAT) with crutches or a walker, provided stable fixation is achieved. This is a key advantage of IMN.
- Plate Osteosynthesis: Often touch-down weight-bearing (TDWB) or non-weight-bearing (NWB) initially, progressing to partial weight-bearing (PWB) based on construct stability and fracture comminution.
-
Physical Therapy (PT):
- Ankle Pumps & Quadriceps Sets: To prevent DVT and maintain muscle tone.
- Gentle Passive & Active-Assisted Range of Motion (ROM): Of the hip and knee, within pain limits, to prevent stiffness. Knee flexion is particularly important.
- Upper Body Strengthening: To facilitate ambulation with assistive devices.
Phase 2: Early Mobilization & Strengthening (Weeks 1-6)
- Weight-Bearing Progression: Gradually increase WB as tolerated, guided by pain and radiographic signs of early callus formation. Patients with IMN typically progress to full weight-bearing (FWB) over 2-4 weeks. Plate fixation may require slower progression over 6-12 weeks.
-
Physical Therapy (PT):
- Active ROM: Progress to full active ROM of hip and knee. Focus on achieving at least 90-100 degrees of knee flexion.
- Strengthening: Initiate isometric and isotonic exercises for quadriceps, hamstrings, gluteals, and core musculature. Examples include straight leg raises, gluteal sets, gentle hamstring curls, and knee extensions.
- Gait Training: Progression from walker to crutches, then to a single crutch or cane, and eventually independent ambulation. Emphasis on proper gait mechanics.
Phase 3: Intermediate Healing & Advanced Strengthening (Months 2-4)
- Radiographic Assessment: X-rays at 6-8 weeks and 12-16 weeks to confirm callus formation and progression of healing.
- Weight-Bearing: Full weight-bearing should be achieved by this stage in most IMN patients. Plating patients should be progressing towards FWB.
-
Physical Therapy (PT):
- Advanced Strengthening: Incorporate progressive resistive exercises, closed-chain activities (e.g., squats, lunges), balance training, and proprioceptive drills.
- Functional Training: Begin incorporating sport-specific drills or work-related tasks if applicable.
- Scar Mobilization: To prevent adhesions and improve soft tissue gliding.
Phase 4: Full Recovery & Return to Activity (Months 4-12+)
- Radiographic Assessment: Continue monitoring healing until cortical bridging and remodeling are evident.
- Activity Progression: Gradual return to recreational activities and sports, guided by pain, strength, and confidence. High-impact activities should be delayed until full healing is confirmed.
-
Hardware Removal:
- Indications: Symptomatic hardware (e.g., bursitis over the nail, knee pain from distal locking screws, prominent plates), or patient preference.
- Timing: Typically 12-18 months post-op, once the fracture is fully healed and cortical remodeling has occurred.
- Risks: Refracture (especially in weight-bearing bones), infection, nerve injury. These risks must be weighed against the benefits.
Summary of Key Literature / Guidelines
Management of young femoral shaft fractures is guided by strong evidence favouring early, stable internal fixation.
- Intramedullary Nailing as Gold Standard: Numerous studies and systematic reviews consistently identify reamed intramedullary nailing as the preferred method for diaphyseal femoral fractures in adults. It offers advantages of load-sharing, biological fixation, high union rates (95-99%), and early weight-bearing. Unreamed nailing may be considered in specific polytrauma settings (e.g., severe pulmonary compromise) but often provides less stable fixation and has slightly higher non-union rates.
- Timing of Fixation (Damage Control Orthopaedics vs. Early Total Care): The concept of Damage Control Orthopaedics (DCO) versus Early Total Care (ETC) is critical in polytrauma. ETC (definitive fixation within 24-48 hours) is generally preferred for physiologically stable polytrauma patients, reducing complications like ARDS, fat embolism, and prolonged ICU stay. DCO (temporary external fixation followed by delayed definitive fixation) is reserved for physiologically unstable patients (the "borderline" or "unstable" patient), allowing resuscitation and organ stabilization before definitive surgery. The decision-making process requires careful assessment of the patient's "physiologic reserve."
- Rotation Control: Preventing rotational malunion is a major challenge. Studies indicate a significant incidence (up to 20-30%) of clinically relevant rotational malunion if not adequately assessed. Various intraoperative techniques, including comparing lesser trochanter profiles on fluoroscopy, clinical assessment of foot rotation, and computer-assisted navigation, have been described to minimize this complication.
- Entry Point for Antegrade Nailing: The piriformis fossa entry point has been associated with a higher risk of iatrogenic avascular necrosis of the femoral head. The greater trochanteric tip entry point is now widely preferred, balancing optimal nail alignment with minimizing injury to the surrounding blood supply.
- Role of Plate Osteosynthesis: While IMN is dominant for diaphyseal fractures, plate osteosynthesis, particularly with locking plates, remains crucial for metaphyseal and articular fractures (e.g., distal femoral fractures, subtrochanteric fractures with significant comminution that preclude IMN). Minimally Invasive Plate Osteosynthesis (MIPO) techniques are gaining traction for these indications to preserve periosteal blood supply.
- Prevention of Complications: Prophylactic antibiotics, DVT prophylaxis, meticulous surgical technique, and early mobilization are evidence-based practices to minimize infection, thromboembolic events, and stiffness. For Heterotopic Ossification (HO) prevention in high-risk patients (e.g., concomitant head injury), NSAIDs or low-dose radiation therapy can be considered.
- Rehabilitation Guidelines: Early weight-bearing and aggressive physical therapy are emphasized to prevent stiffness and facilitate functional recovery. While specific protocols vary, the general principle of progressive loading and functional return is universally accepted, tailored to the individual patient and fixation stability.
- Hardware Removal: The decision to remove hardware is nuanced. While often requested by patients, it carries surgical risks. Current evidence suggests that hardware removal is not always necessary unless symptomatic and should be considered only after complete fracture healing and remodeling.
