Introduction to Upper Extremity Magnetic Resonance Imaging
Magnetic Resonance Imaging (MRI) has a highly specialized and continuously expanding role in the evaluation of pathological conditions of the upper extremity, particularly the wrist, elbow, and shoulder articulations. The successful diagnostic study of these complex joints requires high-resolution images, which are best obtained utilizing advanced surface coil techniques and high-field systems (1.5 Tesla or 3.0 Tesla).
Often, these joints are examined using an extremity coil, which traditionally requires the extension of the arm overhead within the isocenter of the magnetic field—a posture colloquially known as the "Superman position." This position is notoriously difficult to maintain for all but the most agile individuals, often leading to motion artifacts that degrade image quality. While open MRI scanners alleviate this claustrophobic and ergonomic problem, there is usually a clinical tradeoff: a reduced signal-to-noise ratio (SNR) or a significantly increased examination time. Dedicated wrist and elbow coils, when available, or coupled surface coils allow imaging of these articulations at the patient’s side, drastically improving patient compliance and image fidelity. Ultimately, every MRI examination must be meticulously directed at solving a specific clinical problem or surgical question.
Clinical Pearl: When ordering an MRI for upper extremity pathology, always specify the suspected diagnosis. This allows the musculoskeletal radiologist to tailor the pulse sequences (e.g., adding FABS—Flexed Abducted Supinated—views for distal biceps evaluation) and optimize the field of view (FOV).
The Shoulder: Labral Pathology and Paralabral Cysts
Although the primary focus of extremity coils often centers on the distal segments, the shoulder joint frequently presents with complex capsulolabral pathologies that require high-resolution MRI arthrography for definitive surgical planning.
Anterior Labral Tears and MRI Arthrography
The glenoid labrum is a critical static stabilizer of the glenohumeral joint, deepening the glenoid concavity by approximately 50% and serving as the attachment site for the glenohumeral ligaments.
Indications for Surgery:
Surgical intervention is indicated for recurrent anterior shoulder instability, persistent pain following a traumatic dislocation, or failure of a comprehensive 3- to 6-month conservative rehabilitation program. MRI arthrography is the gold standard for identifying Bankart lesions, anterior labroligamentous periosteal sleeve avulsions (ALPSA), and Perthes lesions.
Surgical Approach: Arthroscopic Anterior Stabilization (Bankart Repair)
1. Positioning: The patient is placed in either the lateral decubitus position (with 10-15 lbs of balanced suspension traction) or the beach-chair position, depending on surgeon preference.
2. Portal Placement: A standard posterior viewing portal is established, followed by the creation of anteroinferior (5 o'clock) and anterosuperior (3 o'clock) working portals using an outside-in spinal needle localization technique.
3. Preparation: The anterior labrum and capsule are mobilized from the glenoid neck using an arthroscopic elevator. It is imperative to release the tissue inferiorly to the 6 o'clock position to allow adequate superior shift during repair.
4. Bone Preparation: The anterior glenoid neck is decorticated using a motorized burr to create a bleeding bone bed, promoting biological healing of the capsulolabral complex.
5. Anchor Placement: Suture anchors (typically all-suture or biocomposite) are placed on the articular margin. The first anchor is placed at the 5:30 position.
6. Capsular Plication: Sutures are passed through the capsulolabral tissue using a suture-shuttling device, ensuring a healthy bite of the inferior glenohumeral ligament (IGHL) to achieve an inferior-to-superior capsular shift.
Postoperative Protocol:
Patients are immobilized in a sling for 4 to 6 weeks. Passive range of motion (ROM) begins at week 2, avoiding external rotation beyond neutral. Active ROM commences at week 6, with strengthening initiated at week 10. Return to contact sports is typically permitted at 6 months postoperatively.
Spinoglenoid Notch Ganglions and Suprascapular Nerve Entrapment
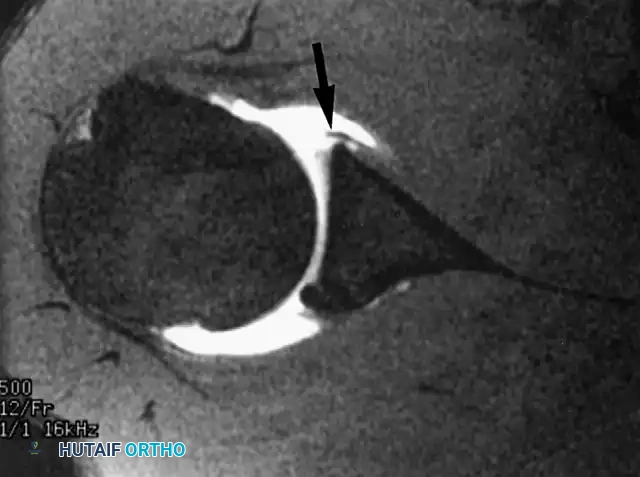
Paralabral cysts, often presenting as soft-tissue ganglions, are frequently associated with superior labral anterior-posterior (SLAP) tears or posterior labral tears. When these cysts extend into the spinoglenoid notch, they can compress the suprascapular nerve.

Biomechanics and Pathophysiology:
The suprascapular nerve provides motor innervation to the supraspinatus and infraspinatus muscles. Entrapment at the spinoglenoid notch selectively denervates the infraspinatus, leading to isolated external rotation weakness and visible muscle atrophy. The one-way valve mechanism of a labral tear allows synovial fluid to pump into the cyst, exacerbating the compression.
Surgical Approach: Arthroscopic Cyst Decompression and Labral Repair
1. Diagnostic Arthroscopy: Identify the associated labral tear (usually a posterior or SLAP lesion).
2. Cyst Decompression: The cyst can often be decompressed intra-articularly by elevating the torn labrum. If the cyst does not decompress, a capsulotomy is performed posterior to the biceps anchor, carefully dissecting toward the spinoglenoid notch to evacuate the gelatinous ganglion fluid.
3. Labral Repair: The underlying labral pathology must be repaired using suture anchors to close the one-way valve and prevent cyst recurrence.
Surgical Warning: When dissecting near the spinoglenoid notch, meticulous care must be taken to avoid iatrogenic injury to the suprascapular nerve and artery, which lie in close proximity to the base of the coracoid and the posterior glenoid neck.
The Wrist: Carpal Ligaments and the TFCC
In the wrist, the most common indication for MRI is the evaluation of the intrinsic carpal ligaments and the triangular fibrocartilage complex (TFCC).
Triangular Fibrocartilage Complex (TFCC) Injuries
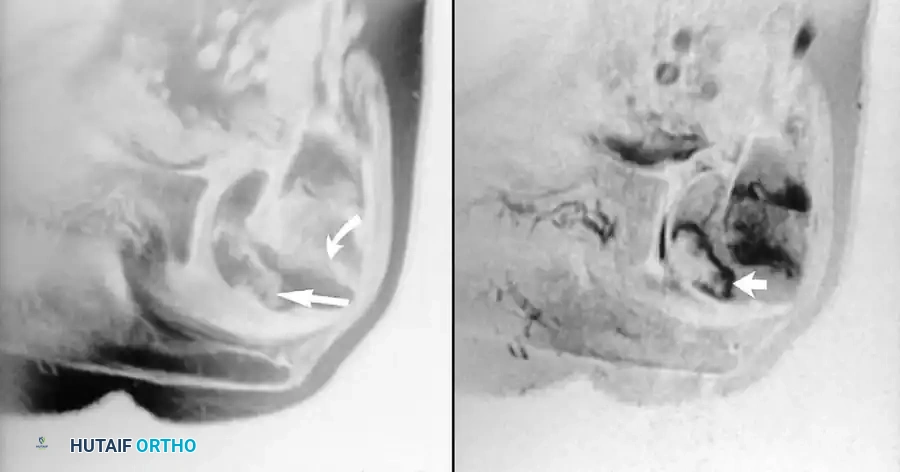
The TFCC is the primary stabilizer of the distal radioulnar joint (DRUJ) and acts as a shock absorber, transmitting approximately 20% of the axial load from the carpus to the ulna. It is composed of signal-poor fibrocartilage. Perforations or tears in the TFCC appear as linear defects or gaps filled with hyperintense fluid on coronal gradient-echo or T2-weighted pulse sequences.

Indications for Surgery:
Surgical intervention is indicated for Palmer Class 1B (ulnar avulsion) or 1D (radial avulsion) tears that fail conservative management, particularly when associated with DRUJ instability. Central perforations (Class 1A) are typically debrided rather than repaired due to the avascular nature of the central articular disc.
Surgical Approach: Arthroscopic TFCC Repair (Outside-In Technique)
1. Positioning: The patient is placed supine with the arm on a hand table. The wrist is suspended in a traction tower utilizing 10-12 lbs of longitudinal traction via finger traps on the index and middle fingers.
2. Portal Placement: Standard radiocarpal portals (3-4 and 4-5) are established. The 6R portal is utilized for viewing the ulnar periphery of the TFCC.
3. Debridement: The tear is identified, and the synovitis is cleared using a 2.0 mm or 2.9 mm full-radius shaver. The ulnar capsule is abraded to stimulate a healing response.
4. Suture Passing: A spinal needle is introduced from the ulnar aspect of the wrist, just volar to the extensor carpi ulnaris (ECU) tendon, passing through the capsule and the peripheral edge of the TFCC. A PDS suture is shuttled through.
5. Knot Tying: A second needle is passed dorsal to the ECU. The sutures are retrieved and tied over the capsule, securely reducing the TFCC to its ulnar footprint.
Postoperative Protocol:
The wrist and elbow are immobilized in a Muenster cast or sugar-tong splint for 4 weeks to prevent forearm rotation. This is followed by a removable wrist splint and the initiation of active ROM. Strengthening begins at 8 weeks.
Intrinsic Carpal Ligament Disruptions
Although the evaluation of the scapholunate (SL) and lunatotriquetral (LT) ligaments is highly challenging, with optimal technique and 3.0T equipment, the integrity of these structures can be consistently assessed. Before the advent of high-resolution MRI, these ligaments were studied almost exclusively by arthrography, a method still preferred by some authors for its dynamic capabilities.
The extrinsic carpal ligaments can be identified with three-dimensional volumetric scanning and subsequent reconstruction; however, the MRI assessment of these specific extrinsic ligaments currently has little impact on operative treatment algorithms compared to the intrinsic ligaments.
The Elbow and Additional Wrist Pathologies
MRI evaluation of the elbow is critical for assessing collateral ligament integrity (e.g., Ulnar Collateral Ligament in throwing athletes), osteochondral lesions of the capitellum, and distal biceps tendon ruptures.
Advanced Imaging of the Elbow
The elbow presents unique challenges for MRI due to its position relative to the magnetic isocenter. When evaluating the ulnar collateral ligament (UCL), coronal and axial T1 and T2 fat-suppressed images are paramount. A "T-sign" on MR arthrography—where contrast extends medial to the sublime tubercle—is pathognomonic for a distal UCL tear.
Surgical Approach: UCL Reconstruction (Tommy John Surgery)
1. Incision: A medial longitudinal incision is made centered over the medial epicondyle.
2. Nerve Management: The ulnar nerve is identified and protected. Depending on preoperative symptoms, an ulnar nerve transposition may be performed.
3. Muscle Splitting: The flexor-pronator mass is split longitudinally to expose the native UCL.
4. Tunnel Creation: Convergent tunnels are drilled in the sublime tubercle of the ulna, and a single or double tunnel is created in the medial epicondyle.
5. Graft Passage: A palmaris longus or gracilis autograft is passed through the tunnels in a figure-of-eight fashion and tensioned with the elbow in 30 degrees of flexion and varus stress applied.
Carpal Tunnel Syndrome and Osteonecrosis
MRI has a limited, albeit specific, role in the evaluation of carpal tunnel syndrome. Although this remains a strictly clinical and electrodiagnostic (EMG/NCS) diagnosis, axial imaging with T2 weighting can clearly display space-occupying masses (e.g., lipomas, ganglions, anomalous muscle bellies) within the confines of the carpal tunnel, as well as edema and swelling of the median nerve.
Furthermore, MRI is highly sensitive and useful in detecting marrow abnormalities in osteonecrosis. This is classically seen in the lunate in Kienböck disease or in the scaphoid following a proximal pole fracture.
Surgical Management of Kienböck Disease:
Treatment is dictated by the Lichtman classification.
* Stage I-II: If ulnar minus variance is present, a joint-leveling procedure, such as a radial shortening osteotomy, is indicated to unload the lunate.
* Stage III: Characterized by lunate collapse. Options include vascularized bone grafting (e.g., 4+5 Extensor Compartmental Artery graft) or proximal row carpectomy (PRC) if carpal collapse is severe.
* Stage IV: Pancarpal arthritis necessitates a total wrist fusion or total wrist arthroplasty.
Clinical Pearl: In cases of scaphoid nonunion with suspected avascular necrosis of the proximal pole, MRI without contrast is often sufficient to detect marrow edema; however, gadolinium-enhanced MRI provides the most accurate assessment of proximal pole perfusion, directly dictating whether a vascularized bone graft (e.g., 1,2-Intercompartmental Supraretinacular Artery graft) is required over a standard non-vascularized structural graft.
Conclusion
The integration of high-resolution MRI into the diagnostic algorithm of upper extremity orthopaedics has revolutionized the precision with which surgeons can plan interventions. From the intricate capsulolabral anatomy of the shoulder to the delicate fibrocartilaginous structures of the wrist, advanced imaging allows for targeted, minimally invasive, and highly successful surgical outcomes. Mastery of these imaging modalities, coupled with a profound understanding of the underlying biomechanics and surgical anatomy, is essential for the modern orthopaedic surgeon.
