Introduction to the Wafer Distal Ulnar Resection
The partial, or “wafer,” excision of the distal ulna is a highly specialized, joint-preserving orthopedic procedure originally described and popularized by Feldon, Terrono, and Belsky. It is primarily indicated for patients suffering from symptomatic tears of the triangular fibrocartilage complex (TFCC), ulnar impaction syndrome (ulnocarpal abutment), or a combination of both.
The fundamental philosophy of the wafer procedure is to decompress the ulnocarpal joint by removing the distal 2 to 4 millimeters of the ulnar dome (the "wafer" of bone and cartilage) while meticulously preserving the ulnar styloid process and the critical foveal attachments of the radioulnar ligaments. Extensive clinical outcome studies have demonstrated that the wafer resection provides pain relief and restoration of grip strength and wrist function that are equal, and in some specific cohorts superior, to those obtained with a formal ulnar shortening osteotomy (USO).
By avoiding a diaphyseal osteotomy, the wafer procedure eliminates the risks of delayed union, nonunion, and hardware-related complications that frequently necessitate a second surgery for plate removal in USO patients. Today, the procedure can be performed via a traditional open approach or an all-arthroscopic approach, depending on the surgeon's expertise and the specific pathoanatomy of the TFCC tear.
Pathoanatomy and Biomechanics of Ulnocarpal Impaction
To fully appreciate the utility of the wafer distal ulnar resection, the operating surgeon must understand the biomechanics of load transmission across the human wrist.
In a wrist with neutral ulnar variance, approximately 80% of the axial load is transmitted through the radiocarpal joint, while 20% is transmitted through the ulnocarpal joint via the TFCC. However, ulnar variance is not static; it is dynamic and changes with forearm rotation and grip. Pronation and forceful gripping increase relative ulnar positive variance.
An increase in ulnar variance of just 2.5 mm shifts the load distribution dramatically, increasing the load transmitted across the ulnocarpal joint to approximately 42%. Over time, this excessive load leads to ulnar impaction syndrome, characterized by:
* Degenerative tearing or central perforation of the articular disc of the TFCC.
* Chondromalacia and eburnation of the ulnar head.
* Chondral wear on the proximal ulnar aspect of the lunate and the proximal radial aspect of the triquetrum.
* Tearing of the lunotriquetral (LT) interosseous ligament.
The wafer resection directly addresses this biomechanical overload. By removing 2 to 4 mm of the distal ulna, the surgeon effectively converts a positive ulnar variance to a neutral or slightly negative variance, thereby normalizing load transmission and alleviating the impaction on the carpus.
Indications and Patient Selection
Proper patient selection is the most critical determinant of success for the wafer distal ulnar resection. The procedure is highly effective when applied to the correct pathology but will fail predictably if used outside its specific indications.
Primary Indications
- Ulnar Impaction Syndrome: Symptomatic ulnocarpal abutment that has failed a minimum of 3 to 6 months of conservative management (splinting, NSAIDs, activity modification, and intra-articular corticosteroid injections).
- Symptomatic TFCC Tears: Specifically, Palmer Class 2 (degenerative) tears with associated ulnar-positive variance.
- Mild to Moderate Ulnar Positive Variance: Patients with an ulnar positive variance of +1 mm to +4 mm.
Clinical Pearl: The wafer procedure is ideal for patients with +1 to +3 mm of ulnar positive variance. If the patient has severe ulnar positive variance (greater than 4 to 5 mm), an ulnar shortening osteotomy is preferred. Attempting a wafer resection of >4 mm risks violating the foveal attachment of the TFCC, leading to iatrogenic distal radioulnar joint (DRUJ) instability.
Contraindications
The wafer procedure is strictly contraindicated in the presence of:
* Distal Radioulnar Instability: The procedure does not stabilize the DRUJ; if the joint is unstable, a reconstructive procedure is required.
* DRUJ Degenerative Arthritis: The wafer procedure preserves the articulation between the ulnar head and the sigmoid notch of the radius. If this articulation is arthritic, a Darrach procedure, Sauvé-Kapandji procedure, or DRUJ arthroplasty is indicated.
* Carpal Instability: Uncorrected carpal instability (e.g., severe VISI or DISI deformities) will not be addressed by ulnar decompression.
* Severe Ulnar Positive Variance: Variance exceeding 4-5 mm.
Preoperative Clinical and Radiographic Evaluation
Clinical Examination
Patients typically present with ulnar-sided wrist pain that is exacerbated by pronation, gripping, and ulnar deviation.
* Ulnocarpal Stress Test: The examiner places the patient's wrist in maximum ulnar deviation and applies an axial load while rotating the forearm from pronation to supination. A positive test elicits sharp pain or a mechanical catching sensation.
* DRUJ Ballottement Test: Essential to rule out gross DRUJ instability, which would contraindicate the wafer procedure.
Imaging Protocol
- Zero-Rotation PA Radiograph: True ulnar variance must be measured on a standardized posteroanterior (PA) radiograph with the shoulder abducted 90 degrees, the elbow flexed 90 degrees, and the forearm in neutral rotation.
- Magnetic Resonance Imaging (MRI): Highly recommended to evaluate the integrity of the TFCC, assess for subchondral cystic changes in the lunate or ulnar head, and evaluate the lunotriquetral ligament.
Surgical Anatomy
A profound understanding of the ulnar-sided wrist anatomy is required to perform this procedure safely:
* Dorsal Sensory Branch of the Ulnar Nerve (DSBUN): Emerges from beneath the flexor carpi ulnaris (FCU) approximately 5 to 8 cm proximal to the ulnar styloid and travels dorsally. It is highly susceptible to iatrogenic injury during the surgical approach.
* Extensor Carpi Ulnaris (ECU) Subsheath: The ECU tendon runs in the 6th extensor compartment. The subsheath is a distinct structure from the extensor retinaculum and is critical for ECU stability. It must be preserved or meticulously repaired.
* The TFCC Foveal Attachment: The deep fibers of the radioulnar ligaments attach to the fovea at the base of the ulnar styloid. This is the primary stabilizer of the DRUJ. The wafer resection must remain distal to this insertion.
Open Surgical Technique: Step-by-Step
The open approach remains a highly reliable method for performing the wafer resection, particularly when arthroscopic equipment is unavailable or when concurrent open procedures are required.
1. Patient Positioning and Preparation
- Place the patient supine on the operating table.
- Apply a well-padded pneumatic tourniquet to the proximal arm.
- Prepare and drape the affected upper extremity in a standard sterile fashion.
- Place the arm on a radiolucent hand table. Pronate the forearm to bring the distal ulna into a prominent dorsal position.
2. Surgical Approach and Dissection
- Make a longitudinal dorsal skin incision extending 5 to 7 cm proximal to the distal ulnocarpal joint, centered over the distal ulna.
- Carefully dissect through the subcutaneous tissues.
- CRITICAL STEP: Identify, mobilize, and protect the dorsal sensory branch of the ulnar nerve (DSBUN). Retract it gently with a vessel loop.
- Identify the extensor retinaculum. Incise the retinaculum over the 5th extensor compartment (extensor digiti minimi) or between the 5th and 6th compartments.
- Retract the ECU tendon ulnarward. Leave the ECU subsheath intact to prevent postoperative ECU subluxation.
3. Capsulotomy and Joint Exposure
- Identify the dorsal capsule of the DRUJ.
- Make a U-shaped incision in the DRUJ capsule. The base of the "U" should be ulnar, leaving the capsular flap attached to the dorsal rim of the sigmoid notch of the radius.
- Reflect the capsular flap radially to expose the DRUJ, the proximal surface of the TFCC, and the ulnar head.
- Inspect the exposed structures. Evaluate the articular cartilage of the ulnar head, the integrity of the TFCC, and the proximal articular surfaces of the lunate and triquetrum.
4. The Wafer Resection
- Using a narrow, sharp osteotome, a small rongeur, or a high-speed motorized burr, begin the resection of the distal ulnar dome.
- Remove the distal 2 to 4 mm of the ulnar head. This resection must include the articular cartilage and the underlying subchondral bone.
- Preservation of Anatomy: You must meticulously preserve the ulnar styloid process, the foveal attachments of the triangular fibrocartilage, and the articular cartilage of the ulnar seat (the portion of the ulna that articulates with the sigmoid notch of the radius).
- Debride any unstable flap tears or degenerative abrasions on the proximal surface of the TFCC using a scalpel or arthroscopic shaver.
Surgical Warning: The resection must be perfectly contoured. Avoid leaving sharp cortical edges on the volar or dorsal margins of the resected ulnar head, as these can cause secondary impingement or attritional wear on the overlying soft tissues.
5. Closure
- Deflate the pneumatic tourniquet and achieve meticulous hemostasis using bipolar electrocautery. Hematoma formation in this space can lead to severe postoperative stiffness.
- Close the DRUJ capsule carefully. Suspend the dorsal edge of the TFCC to the capsule with a row of interrupted non-absorbable or slowly absorbing sutures (e.g., 3-0 PDS or Vicryl). Tightly close the DRUJ capsule to restore dorsal stability.
- Repair the extensor retinaculum, ensuring the ECU tendon glides smoothly without subluxation.
- Close the skin with interrupted nylon or subcuticular sutures.
Arthroscopic Wafer Resection Technique
With advancements in wrist arthroscopy, the arthroscopic wafer resection has become the gold standard for many specialized hand surgeons. It allows for simultaneous evaluation and treatment of intra-articular carpal pathology, minimal soft tissue disruption, and faster early rehabilitation.
Arthroscopic Setup and Portal Placement
- Suspend the wrist in a traction tower with 10 to 15 lbs of longitudinal traction applied via finger traps on the index and middle fingers.
- Establish standard radiocarpal portals (3-4 and 6R) to evaluate the radiocarpal joint, the distal surface of the TFCC, and the interosseous ligaments.
- If a central TFCC tear is present, the arthroscope can be passed directly through the tear to visualize the ulnar head. If the TFCC is intact but ulnar impaction is present, the DRUJ portals (proximal and distal DRUJ portals) must be utilized.
Step 1: TFCC Debridement and Ulnar Head Exposure
- Introduce the arthroscope through the 3-4 portal and a motorized shaver through the 6R portal.
- Identify the degenerative central perforation of the TFCC.
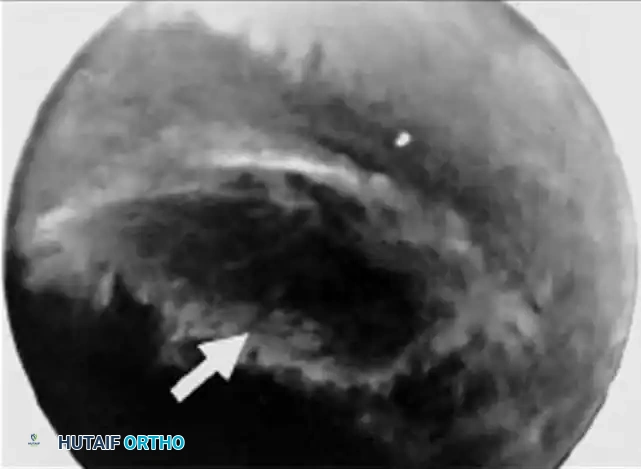
- Debride the unstable margins of the TFCC tear until a stable, smooth rim is achieved. This debridement exposes the chondromalacic ulnar head beneath.

Arthroscopic view demonstrating a central perforation of the triangular fibrocartilage complex (TFCC) (arrow), a hallmark of ulnar impaction syndrome.
Step 2: Arthroscopic Bone Resection
- Introduce a 2.9 mm or 2.0 mm high-speed arthroscopic burr through the 6R portal (or directly through the TFCC defect).
- Begin the wafer resection of the distal ulna. The burr is used to decorticate the articular cartilage and resect 2 to 3 mm of the subchondral bone.
- The resection should extend from the radial border of the ulnar head to the base of the ulnar styloid, ensuring the foveal attachments are not violated.
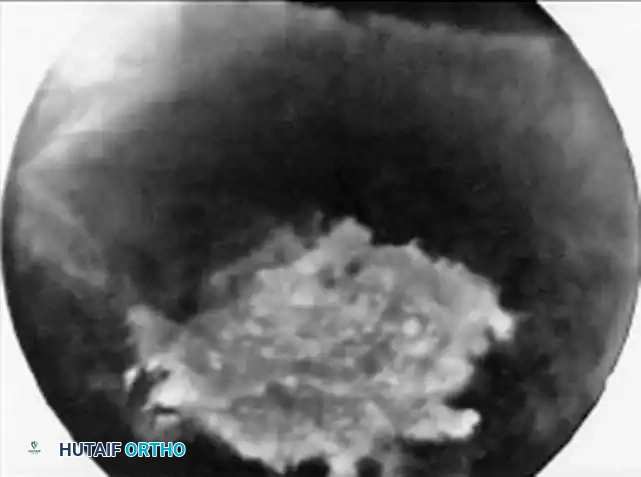
Arthroscopic view after excision of the central disc. The high-speed burr is utilized to perform a wafer resection of 2 mm of the ulnar head (arrow), decompressing the ulnocarpal joint.
Step 3: Final Assessment and Washout
- Release the longitudinal traction and take the wrist through a range of pronation and supination while viewing arthroscopically.
- Confirm that there is no residual impingement between the resected ulnar head and the lunate/triquetrum during dynamic rotation.
- Thoroughly irrigate the joint to remove all bone debris, which could otherwise cause severe postoperative synovitis.
Final arthroscopic view after completion of the TFCC debridement and the wafer resection. The ulnocarpal space is now adequately decompressed.
Postoperative Care and Rehabilitation Protocol
The postoperative protocol is designed to protect the capsular repair (in open procedures) while preventing stiffness in the radiocarpal and distal radioulnar joints.
- Immediate Postoperative Phase (Days 0-14):
- Apply a bulky compression dressing supported by a well-molded sugar-tong splint.
- The splint should extend above the elbow, holding the forearm in mid-supination. This position relaxes the dorsal capsule and the DRUJ ligaments.
- Strict elevation and active digital range of motion (ROM) are encouraged immediately to prevent tendon adhesions and reduce edema.
- First Clinic Visit (10 to 14 Days):
- Remove the postoperative dressing and skin sutures.
- Transition the patient to a custom-molded Munster splint or a short-arm supination splint. This splint is worn continuously for an additional 2 to 3 weeks.
- Rehabilitation Phase (3 to 6 Weeks):
- At 3 weeks postoperatively, the splint is discontinued, and gentle, active-assisted range of motion exercises for the wrist and forearm are initiated under the guidance of a certified hand therapist.
- Avoid forceful gripping or heavy lifting.
- Strengthening Phase (6+ Weeks):
- Progression to normal use and activities is encouraged after 6 weeks.
- Progressive grip strengthening and proprioceptive training are initiated.
- Expected Recovery:
- Patients must be counseled preoperatively that maximal recovery, complete resolution of deep ulnar
