Unusual Causes of Kyphosis: Comprehensive Surgical Management
Key Takeaway
Unusual causes of kyphosis, including postlaminectomy deformity, achondroplasia, and mucopolysaccharidoses, present complex biomechanical challenges. Management requires a deep understanding of spinal instability, altered growth mechanics, and neurological risks. Surgical intervention typically necessitates combined anterior and posterior arthrodesis, meticulous decompression, and rigid instrumentation to restore sagittal balance and prevent progressive neurological deterioration in the growing spine.
UNUSUAL CAUSES OF KYPHOSIS
While Scheuermann’s disease and postural roundback represent the vast majority of kyphotic deformities encountered in orthopedic practice, unusual causes of kyphosis demand a heightened level of biomechanical understanding and surgical precision. These deformities—most notably postlaminectomy spinal deformity, skeletal dysplasias, and mucopolysaccharidoses—are frequently associated with intrinsic osseous deficiencies, ligamentous instability, and significant neurological risk. The management of these conditions requires a multidisciplinary approach, meticulous preoperative planning, and often, complex reconstructive spinal surgery.
Postlaminectomy Spinal Deformity
Laminectomies are most frequently performed in the pediatric population for the diagnosis and resection of spinal cord tumors (e.g., astrocytomas, ependymomas), though they are also indicated in the management of neurofibromatosis, syringomyelia, and severe trauma. The iatrogenic disruption of the posterior tension band in a growing spine predictably leads to progressive deformity.
Incidence and Risk Factors
The frequency of spinal deformities following laminectomy in children is alarmingly high. Historical series by Haft et al., Tachdjian and Matson, and Lonstein et al. report an incidence ranging from 33% to a staggering 100%.
Yasuoka et al. established that chronological age is the most critical determinant of postlaminectomy deformity, with children younger than 15 years being at the highest risk. Furthermore, the anatomical level of the laminectomy directly correlates with the likelihood of instability. Cervical and cervicothoracic laminectomies are almost universally followed by deformity due to the high mobility and natural lordotic reliance on posterior elements in these regions.
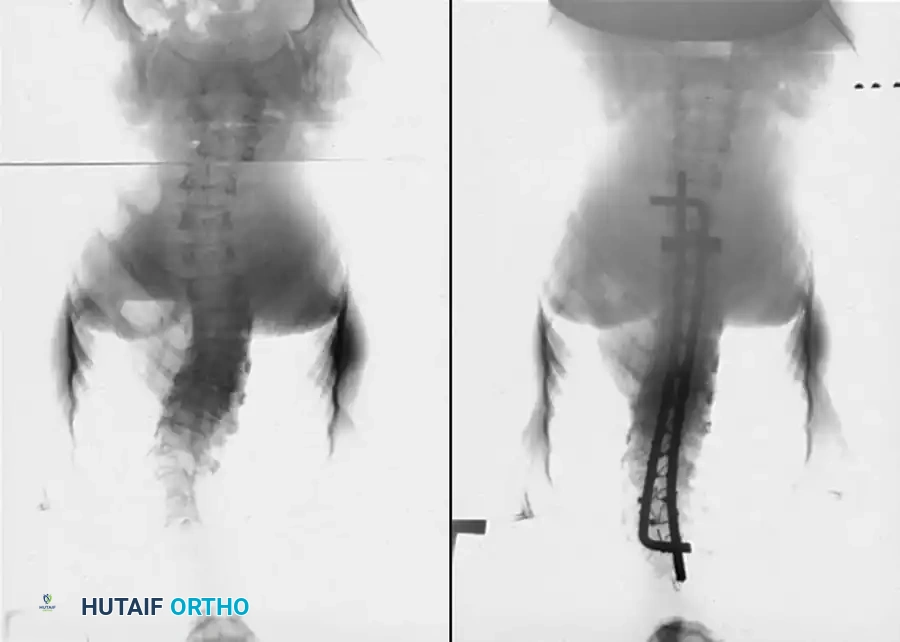
Fig. 38-216 A, Preoperative posteroanterior radiographs of a patient with osteogenesis imperfecta with progressing curvature. B, Postoperative radiographs after instrumentation with sublaminar cables and Luque rods.
Biomechanics and Pathophysiology
The primary deformity following multiple-level laminectomies is kyphosis, though scoliosis may occur concurrently. Panjabi et al. elegantly demonstrated that the excision of the interspinous ligaments, spinous processes, and laminae obliterates the posterior stabilizing structures. This allows normal physiological flexion forces to overpower the deficient posterior column, driving the spine into kyphosis.
In the pediatric spine, this mechanical imbalance initiates a vicious cycle governed by the Hueter-Volkmann principle. As the spine falls into kyphosis, compressive forces increase exponentially on the anterior cartilaginous endplates of the vertebral bodies. Over time, this pathological compression suppresses anterior physeal growth, resulting in progressive anterior vertebral wedging.
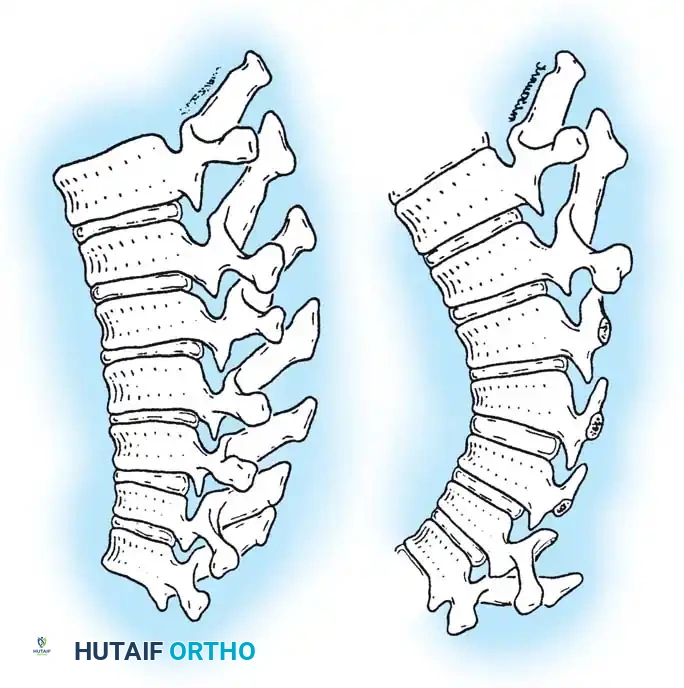
Fig. 38-217 Drawings of the thoracic spine before and after repeated laminectomy illustrating the effects on vertebral body growth. A, Normal rectangular configuration. B, Increased anterior compression due to loss of posterior supporting structures results in decreased anterior growth and subsequent wedging.
Lonstein et al. emphasized the critical role of the facet joints in dictating the morphology of the resulting deformity:
* Complete Bilateral Facetectomy: Results in gross instability at that specific level, producing a sharp, angular kyphos, enlargement of the intervertebral foramen, and posterior opening of the disc space.
* Unilateral Facetectomy: Produces an angular kyphosis accompanied by a sharp, apex-matched scoliosis.
* Preserved Facets: Results in a long, gradual, rounding kyphosis spanning the laminectomy defect.
Clinical Pearl: The etiology of postlaminectomy deformity is multifactorial. In addition to the surgical destabilization, factors such as neuromuscular imbalance (paralysis from the tumor), progressive osseous deformity, and radiation therapy (which injures the vertebral physis) compound the risk of severe progression.
Prevention Strategies
The optimal treatment for postlaminectomy kyphosis is prevention. When posterior access to the spinal canal is required, facet joints must be meticulously preserved.
The advent of laminoplasty (e.g., open-door or French-door techniques) has significantly reduced the incidence of post-surgical deformity. By hinging the laminae and suturing them back into place, the surgeon preserves a fibrous tether and maintains the posterior osseous boundary, which Mimatsu has shown to decrease the incidence of subsequent kyphosis.
Surgical Management
If a deformity is detected early, conservative management with a Milwaukee brace or custom Thoracolumbosacral Orthosis (TLSO) may be attempted to delay progression while the child grows. However, if the patient has a reasonable long-term oncologic prognosis, progressive deformity mandates surgical arthrodesis.
Because of the extensive loss of posterior bone mass, posterior fusion alone is associated with an unacceptably high pseudarthrosis rate (up to 33%). Biomechanically, a posterior fusion mass in a kyphotic spine is subjected to relentless tensile forces. Therefore, combined anterior and posterior spinal fusion is the gold standard, reducing the pseudarthrosis rate to approximately 9.5%.
Stage 1: Anterior Release and Arthrodesis
- Approach: A standard thoracotomy or thoracoabdominal approach is utilized depending on the apex of the curve.
- Discectomy: Radical removal of all disc material is performed. It is imperative to resect the disc entirely back to the posterior longitudinal ligament (PLL). Failure to remove the posterior aspect of the cartilaginous endplate will allow continued posterior growth, exacerbating the kyphosis.
- Grafting: Structural strut grafting (using autologous rib harvested during the approach, or fibular allograft) is placed anteriorly to provide immediate mechanical support and correction. Cancellous bone is packed tightly into the remaining disc spaces.

Fig. 38-218 A, Progressive cervical kyphosis in a 13-year-old girl treated for a low-grade astrocytoma with laminectomy and radiotherapy. Note the severe anterior vertebral wedging.

Fig. 38-218 B, Radiograph demonstrating partial reduction of the kyphotic deformity utilizing preoperative halo traction.
Stage 2: Posterior Instrumentation and Fusion
Performed either under the same anesthetic or staged 1 to 2 weeks later.
1. Instrumentation: Despite the absence of posterior elements, pedicle screw fixation has revolutionized the management of these deformities, allowing rigid three-column fixation.
2. Material Selection: Torpey et al. strongly recommend the use of titanium instrumentation. Titanium provides excellent biomechanical stability while minimizing artifact on postoperative MRI, which is essential for longitudinal tumor surveillance.
3. Salvage Fixation: In cases where the deformity is too severe or the pedicles are too dysplastic to accept screws, postoperative immobilization in a halo-vest or custom cast is mandatory until the anterior fusion mass consolidates.

Fig. 38-218 C, Postoperative radiograph demonstrating restoration of sagittal alignment following combined anterior and posterior fusion.
Skeletal Dysplasias: Achondroplasia
Achondroplasia, an autosomal dominant mutation in the FGFR3 gene, is the most common rhizomelic skeletal dysplasia. The spinal manifestations of achondroplasia are profound, characterized by a congenitally narrowed spinal canal, short pedicles, and a decreased interpedicular distance in the lumbar spine.
Pathoanatomy of Achondroplastic Kyphosis
A thoracolumbar kyphosis is almost universally present at birth in achondroplastic infants. This is primarily a flexible, postural deformity secondary to hypotonia and the relatively large head size. As the child develops truncal muscle tone and begins to ambulate, the kyphosis typically resolves, transitioning into a hyperlordosis.
However, Bailey noted that in approximately 30% of patients, the thoracolumbar kyphosis persists, and in 35% of these cases, it progresses to a severe, rigid structural deformity. This kyphosis is exceptionally poorly tolerated. The apex of the kyphosis acts as a fulcrum over which the spinal cord is draped, severely exacerbating the pre-existing congenital spinal stenosis and leading to early-onset myelopathy or claudication.
Conservative Management
Early intervention is paramount. Pauli et al. demonstrated that aggressive conservative management can prevent the development of structural kyphosis.
* Sitting Protocols: Parents must be strictly instructed to prohibit unsupported sitting in infants. Children should not be allowed to sit up more than 60 degrees, even with support, until adequate truncal tone is achieved.
* Bracing: If a kyphosis develops and exceeds 30 degrees, rigid TLSO bracing is initiated. Bracing is maintained until the child is walking independently and serial radiographs confirm the reversal of vertebral body wedging.
Surgical Management
Operative stabilization is indicated for:
1. Documented progression despite bracing.
2. Kyphosis exceeding 40 degrees in a child older than 5 years.
3. Any neurological deficit attributable to the deformity.
Surgical Warning: Neurological deficits in an achondroplastic infant may not stem from the thoracolumbar kyphosis, but rather from severe narrowing of the foramen magnum causing basilar impression. A comprehensive MRI of the craniocervical junction is mandatory prior to any surgical intervention.
Surgical Technique
Most progressive deformities require a combined anterior and posterior approach. Historically, posterior instrumentation was avoided due to the diminutive size of the spinal canal and the risk of iatrogenic neurological injury. However, modern techniques have proven pedicle screw fixation to be safe and effective.
Ain and Browne outlined a highly successful protocol for pediatric achondroplasia:
1. Anterior Corpectomy: Indicated if the pedicles are too small for instrumentation, if there is severe anterior cord impingement, or if hyperextension radiographs over a bolster fail to correct the kyphosis to less than 50 degrees.
2. Posterior Instrumentation: Pedicle screws are placed under strict fluoroscopic or navigation guidance.
3. Construct Design: All kyphotic segments must be included in the fusion construct. Crucially, if a concomitant laminectomy is performed for decompression, the fusion must be extended at least one level cephalad to the highest laminectomy to prevent the development of a catastrophic junctional kyphosis.
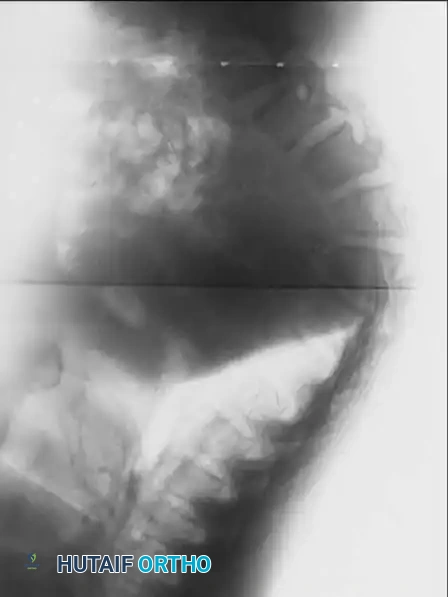
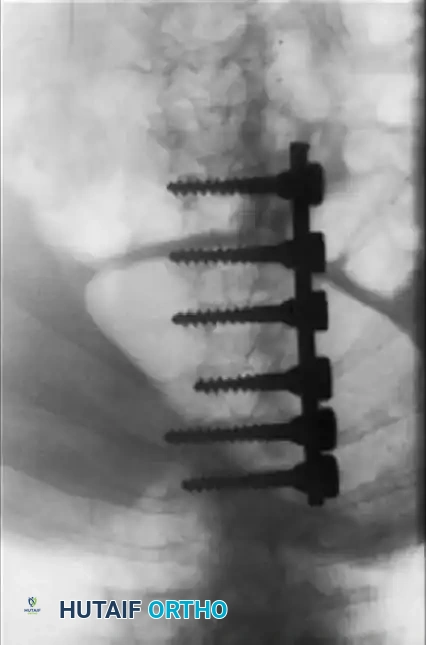
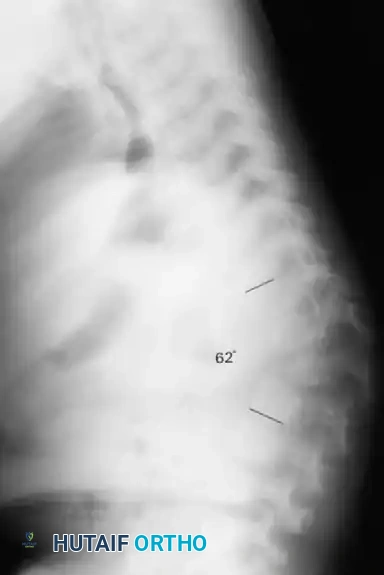
Fig. 38-219 A, Preoperative lateral radiograph of a pediatric patient with achondroplasia demonstrating severe, rigid thoracolumbar kyphosis.

Fig. 38-219 B & C, Postoperative anteroposterior and lateral radiographs demonstrating successful spinal arthrodesis with pedicle screw instrumentation, restoring sagittal balance without neurological compromise.
Additional imaging demonstrating the complex osseous anatomy and pedicle morphology that must be navigated during instrumentation in skeletal dysplasias.
Mucopolysaccharidoses (MPS)
The mucopolysaccharidoses are a group of rare, inherited lysosomal storage disorders characterized by the absence or malfunction of specific enzymes required to break down glycosaminoglycans (GAGs). The intracellular accumulation of GAGs leads to progressive, multisystemic cellular damage.
From an orthopedic standpoint, Morquio syndrome (Type IV), Hurler syndrome (Type I), and Maroteaux-Lamy syndrome (Type VI) are most frequently associated with severe structural spinal deformities.
Pathoanatomy of MPS Kyphosis
The hallmark spinal deformity in MPS is a progressive thoracolumbar kyphosis. The pathophysiology is driven by dysplastic endochondral ossification.
* Vertebral Morphology: The vertebral bodies are characteristically deficient anteriorly, appearing flattened (platyspondyly), notched, or prominently "beaked" on lateral radiographs.
* Disc Pathology: The intervertebral discs are abnormally thick, bulging, and often larger in vertical height than the dysplastic vertebral bodies themselves.
Radiographic representation of the classic thoracolumbar kyphosis seen in mucopolysaccharidoses, highlighting the anterior beaking and platyspondyly.
In early childhood, this kyphosis is highly flexible. However, as the child ages and the dysplastic bone undergoes remodeling under abnormal biomechanical stress, the curve collapses and becomes rigidly fixed.

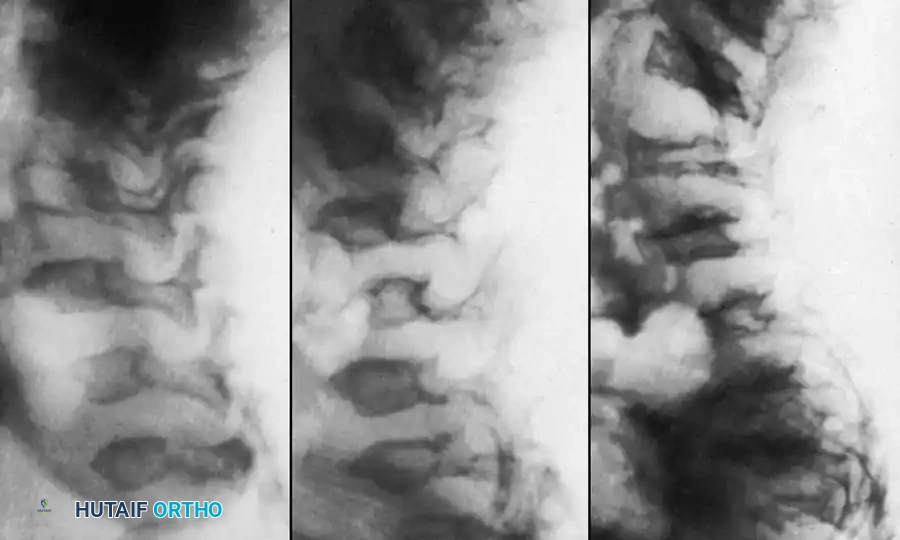
Detailed view of the dysplastic vertebral segments in MPS, demonstrating the thick, bulging intervertebral discs that contribute to the structural collapse.
Cervical Spine Instability: A Critical Consideration
While thoracolumbar kyphosis is the most visible deformity, the most life-threatening orthopedic manifestation of MPS—particularly in Morquio syndrome—is atlantoaxial instability.
Patients with Morquio syndrome universally exhibit odontoid hypoplasia or complete aplasia, combined with ligamentous laxity due to GAG deposition. This results in severe C1-C2 instability.
* Clinical Presentation: The most common early presenting symptom of cervical myelopathy in these children is simply a reduced exercise tolerance. Surgeons must maintain a high index of suspicion, as overt neurological signs (hyperreflexia, clonus) may present late.
* Management: Prophylactic posterior C1-C2 arthrodesis is frequently indicated in Morquio syndrome to prevent sudden catastrophic spinal cord injury or progressive quadriparesis.
Advanced imaging of the cervical and upper thoracic spine in a patient with mucopolysaccharidosis, utilized to evaluate for odontoid hypoplasia and spinal canal stenosis prior to surgical intervention.
Surgical Strategy for MPS Kyphosis
The treatment algorithm for thoracolumbar kyphosis in MPS is heavily influenced by the specific syndrome type and the patient's overall life expectancy.
* Hurler Syndrome (Type I): Historically associated with rapid neurological and cardiopulmonary decline, with death often occurring before age 10. In untreated patients, extensive spinal surgery is rarely indicated. However, with the advent of hematopoietic stem cell transplantation (HSCT) and enzyme replacement therapy (ERT), life expectancy is increasing, making surgical management of the spine more relevant.
* Morquio Syndrome (Type IV): These patients often have normal intelligence and can survive well into adulthood. Progressive, rigid kyphosis in these patients is treated aggressively with combined anterior release/fusion and posterior instrumented arthrodesis, utilizing similar biomechanical principles as described for postlaminectomy deformities. Meticulous care must be taken during anesthesia and positioning to protect the highly unstable cervical spine.
You Might Also Like


