Comprehensive Introduction and Patho-Epidemiology
The management of ankle ligamentous and syndesmotic injuries has evolved significantly over the past several decades, driven by a deeper understanding of ankle kinematics, advanced high-resolution imaging modalities, and rigorous biomechanical studies. The overarching goal of both operative and non-operative treatment remains the restoration of a congruent ankle mortise and the prevention of chronic micro-instability. Failure to recognize and appropriately manage these complex injuries invariably leads to altered joint mechanics, asymmetrical cartilage loading, and early-onset post-traumatic osteoarthritis. As orthopedic surgeons, we must approach these injuries with a high index of suspicion, recognizing that the ankle is not merely a simple hinge joint, but a highly complex, multi-axial articulation dependent on both osseous architecture and dynamic ligamentous restraints.
The fundamental biomechanical principle guiding all ankle trauma surgery was definitively established by Ramsey and Hamilton in their seminal biomechanical studies. They demonstrated that a mere 1-mm lateral shift of the talus within the ankle mortise produces a staggering 42% reduction in the tibiotalar contact area. Because stress per unit area increases exponentially as the total contact area decreases, even microscopic displacement or subtle syndesmotic diastasis contributes to poor functional outcomes and accelerated articular degradation. This principle underscores the absolute necessity for anatomical reduction; "acceptable" alignment in the context of the ankle mortise is an anachronism. The margin for error is virtually nonexistent, demanding meticulous surgical technique and rigid adherence to biomechanical principles.
Epidemiologically, ankle sprains are among the most ubiquitous musculoskeletal injuries, with an estimated incidence of 1 in 10,000 individuals per day. While the vast majority involve the lateral collateral ligament complex and resolve with functional rehabilitation, a significant subset involves the distal tibiofibular syndesmosis or the medial deltoid complex. Syndesmotic sprains, often termed "high ankle sprains," account for approximately 1% to 18% of all ankle sprains, with a markedly higher prevalence in collision sports, elite athletics, and military training environments. These injuries carry a significantly longer recovery time and a higher propensity for chronic pain and instability compared to standard lateral sprains.
Ankle instability may result from isolated ligamentous disruption, osseous avulsion fractures, or a complex combination of both. Clinicians must maintain a heightened vigilance; what may appear as a pure ligamentous injury with talar shift on initial standard radiographs may actually represent a severe rotational injury. The classic Maisonneuve variant, characterized by a proximal fibular fracture with complete disruption of the interosseous membrane and syndesmotic complex, serves as a prime example. Failure to evaluate the entire length of the fibula and accurately assess the medial clear space can lead to catastrophic missed diagnoses, resulting in chronic diastasis, severe pain, and the rapid progression of degenerative joint disease.
Detailed Surgical Anatomy and Biomechanics
The Lateral Collateral Ligament Complex
The lateral ligamentous complex consists of three distinct structures: the anterior talofibular ligament (ATFL), the calcaneofibular ligament (CFL), and the posterior talofibular ligament (PTFL). The ATFL is the weakest of the lateral ligaments and is the primary restraint to anterior translation of the talus, particularly when the ankle is in plantarflexion. It originates from the anterior margin of the lateral malleolus and inserts on the body of the talus anterior to the lateral articular facet. The CFL is an extra-articular, cord-like structure that spans the tibiotalar and subtalar joints, originating from the tip of the lateral malleolus and inserting on the lateral surface of the calcaneus. It serves as the primary restraint to inversion when the ankle is dorsiflexed. The PTFL is the strongest of the three, originating from the posterior aspect of the lateral malleolus and inserting on the posterior tubercle of the talus; it is rarely torn except in severe, massive dislocations.
The Medial Deltoid Ligament Complex
The deltoid ligament is a robust, multifascicular structure divided into superficial and deep layers. The superficial layer, comprising the tibionavicular, tibiocalcaneal, and posterior tibiotalar ligaments, primarily resists hindfoot eversion and valgus stress. The deep layer, consisting of the anterior and posterior deep tibiotalar ligaments, is the critical stabilizer of the medial ankle. It acts as the primary restraint against lateral translation and external rotation of the talus within the mortise. Incompetence of the deep deltoid, even in the presence of an intact lateral malleolus, permits lateral talar shift and subsequent uncoupling of the normal tibiotalar articulation.
The Distal Tibiofibular Syndesmosis
The syndesmotic complex is vital for maintaining the integrity of the ankle mortise during the physiologic widening that occurs with dorsiflexion (as the wider anterior dome of the talus engages the mortise). It consists of four primary structures: the anterior inferior tibiofibular ligament (AITFL), the posterior inferior tibiofibular ligament (PITFL), the transverse ligament, and the interosseous membrane (IOM). The AITFL traverses obliquely from the anterior tubercle of the tibia (Chaput tubercle) to the anterior tubercle of the fibula (Wagstaffe tubercle). The PITFL is significantly stronger and thicker, running from the posterior tibial margin (Volkmann's triangle) to the posterior fibula. The IOM acts as a proximal continuation of the joint, providing resistance against axial and lateral displacement of the fibula.
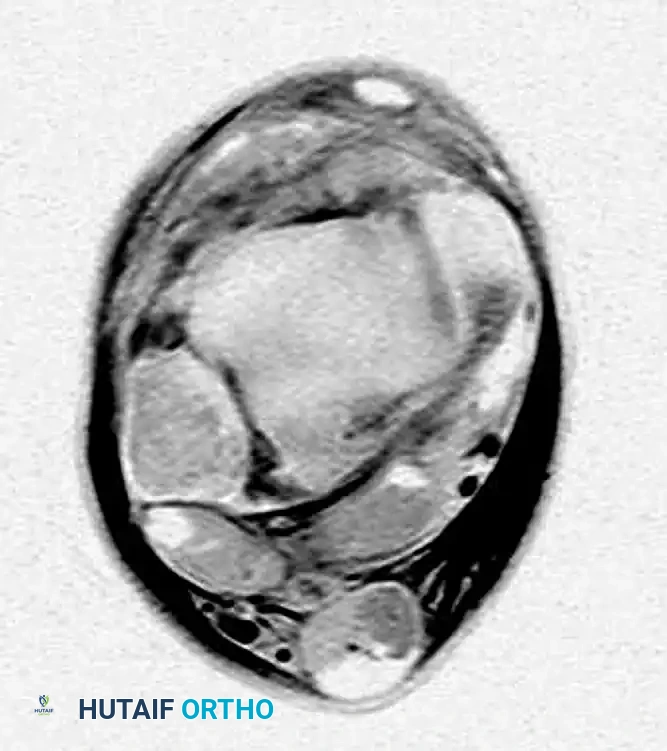
FIGURE 89-6: Axial MRI of a patient with a syndesmosis injury; note the distinct tear of the anterior inferior tibiofibular ligament (AITFL), highlighting the diagnostic utility of advanced imaging in assessing the syndesmotic complex.
Radiographic and MRI Evaluation
Accurate interpretation of standard radiographs remains the cornerstone of initial evaluation. The relationships evaluating the tibiofibular articulation are critical for diagnosing subtle diastasis. The tibiofibular clear space (measured 1 cm proximal to the plafond) should be less than 6 mm on both AP and mortise views. The tibiofibular overlap should be greater than 6 mm on the AP view and greater than 1 mm on the mortise view. The medial clear space should be equal to or less than the superior clear space (typically < 4 mm).
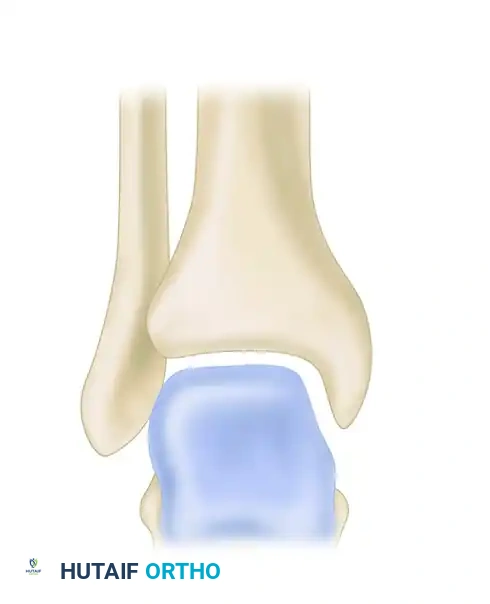
FIGURE 89-7: Radiographic relationships important in evaluating the tibiofibular articulation. Line EF represents the medial clear space; line AB represents the tibiofibular clear space.
More powerful, high-resolution, three-dimensional MRI studies have revolutionized the diagnostic accuracy of ankle and hindfoot injuries. Axial MRI with a local gradient provides optimal visualization of the anterior and posterior talofibular ligaments and the deep layers of the medial collateral ligament. Coronal MRI allows a comprehensive assessment of the calcaneofibular, posterior talofibular, and tibiocalcaneal ligaments. Interestingly, literature suggests no direct correlation between tibiofibular clear space measurements on standard radiographs and MRI-confirmed syndesmotic injuries in subtle cases, making MRI an invaluable adjunct when clinical suspicion remains high despite "normal" radiographs.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention must be meticulously tailored to the individual patient, weighing the severity of the anatomical disruption against the patient's functional demands, comorbidities, and baseline activity level. While the majority of isolated lateral ligament injuries are successfully managed non-operatively, complex rotational injuries, syndesmotic disruption, and combined medial/lateral instability patterns frequently necessitate surgical stabilization to prevent catastrophic joint failure.
Indications for Operative Intervention
Acute surgical repair of the lateral ligament complex is rarely indicated but should be considered in cases of large, displaced bony avulsions, severe combined medial and lateral ligamentous damage (indicating a transient dislocation), or in elite athletes with massive disruptions where expedited return to play is mandated. Chronic lateral instability failing 3 to 6 months of aggressive physical therapy and proprioceptive training is a classic indication for a modified Broström-Gould reconstruction.
For deltoid ligament injuries, isolated complete ruptures are exceedingly rare. They are typically associated with lateral malleolar fractures or syndesmotic disruption. The primary indication for medial exploration and direct deltoid repair is an irreducible ankle mortise. If, after anatomical fixation of the fibula, the medial clear space remains widened, soft tissue interposition—most commonly the posterior tibial tendon or the proximal stump of the avulsed deltoid ligament—must be suspected, mandating open medial exploration.
Syndesmotic injuries require fixation when there is frank diastasis on static radiographs or dynamic instability demonstrated on intraoperative stress testing (the "Hook Test" or external rotation stress views). Failure to stabilize an incompetent syndesmosis inevitably leads to chronic widening of the mortise, lateral talar subluxation, and rapid-onset osteoarthritis.
Contraindications
Absolute contraindications to operative management include active localized infection, severe peripheral vascular disease precluding wound healing, and profound peripheral neuropathy (e.g., severe Charcot arthropathy) where hardware failure and catastrophic breakdown are imminent. Relative contraindications include poorly controlled diabetes mellitus, severe osteoporosis (which compromises hardware purchase), and patient non-compliance, as strict adherence to postoperative weight-bearing restrictions is paramount for successful outcomes.
Summary Table of Indications and Contraindications
| Injury Type | Operative Indications | Non-Operative Indications | Absolute/Relative Contraindications |
|---|---|---|---|
| Lateral Ligaments | Large displaced avulsions; transient dislocation; chronic instability failing >6 months PT. | Grade I-III isolated sprains; first-time injuries; low-demand patients. | Active infection; severe vascular disease; localized soft tissue compromise. |
| Medial Deltoid | Irreducible mortise (soft tissue interposition); persistent medial clear space widening >4mm post-fibular fixation. | Deltoid disruption with anatomically reducible and stable fibular fixation. | Uncontrolled diabetes (relative); severe peripheral neuropathy (Charcot). |
| Syndesmosis | Frank diastasis on static x-rays; positive intraoperative Hook Test; combined unstable rotational fractures. | Stable syndesmosis on stress testing; isolated AITFL sprain without mortise widening. | Non-ambulatory patient; severe osteoporosis precluding screw purchase (relative). |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and Provocative Testing
Pre-operative planning begins with a rigorous clinical examination, particularly focusing on provocative testing to unmask subtle instability patterns. For syndesmotic injuries, the clinical diagnosis relies on specific tests performed only after ruling out proximal fibular fractures.
The Squeeze Test, described by Teitz and Harrington, involves compression of the calf musculature at the mid-calf level. This maneuver causes separation of the distal fibula and tibia, eliciting sharp pain at the distal syndesmosis in the presence of an injury.
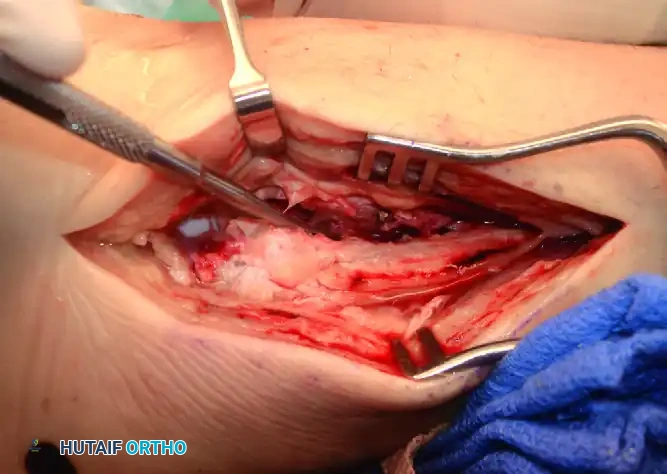
FIGURE 89-11: The Squeeze test is performed by compressing the fibula to the tibia above the midpoint of the calf.

Diagrammatic representation of the Squeeze test mechanism, demonstrating the fulcrum effect that separates the distal tibiofibular joint.
The External Rotation Stress Test is another critical diagnostic maneuver. The examiner stabilizes the leg with the knee flexed to 90 degrees to relax the gastrocnemius, then applies an external rotation force to the foot. Pain elicited over the anterior or posterior tibiofibular ligaments strongly correlates with syndesmotic disruption.

FIGURE 89-12: External rotation testing to evaluate syndesmotic integrity.
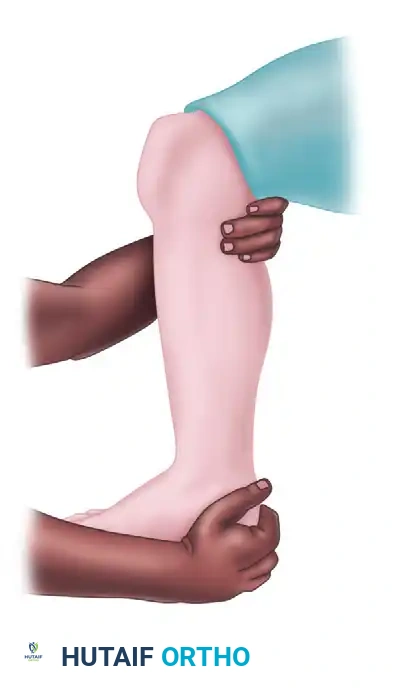
Diagrammatic representation of the External Rotation stress test, highlighting the stress applied to the AITFL and deep deltoid ligaments.
Imaging and Templating
Pre-operative imaging must include weight-bearing orthogonal views of the ankle, full-length tibia/fibula radiographs to rule out a Maisonneuve fracture, and frequently, advanced imaging. CT scans are highly valuable for identifying subtle avulsion fractures (e.g., Wagstaffe or Chaput fragments) and evaluating the precise rotational alignment of the fibula within the incisura fibularis. Pre-operative templating involves determining the optimal trajectory for syndesmotic screws or suture buttons, which should ideally be angled 20 to 30 degrees anteromedially from the fibula to the tibia to match the anatomical axis of the syndesmosis.
Patient Positioning and Setup
The patient is typically positioned supine on a radiolucent operating table. A bump is placed under the ipsilateral hip to internally rotate the leg, bringing the lateral malleolus and fibula into a neutral, strictly lateral position, which facilitates true AP and mortise fluoroscopic imaging. A well-padded pneumatic thigh tourniquet is applied. The C-arm fluoroscopy unit is positioned on the contralateral side of the table, allowing for unobstructed imaging in both the AP, mortise, and lateral planes. The surgeon must ensure that the foot can be freely manipulated through a full range of motion, particularly dorsiflexion, during the reduction and fixation phases of the procedure.
Step-by-Step Surgical Approach and Fixation Technique
Lateral Ligament Repair (Modified Broström-Gould Technique)
When acute or chronic lateral instability necessitates surgical intervention, the modified Broström-Gould technique remains the gold standard. A curvilinear incision is made just anterior and inferior to the lateral malleolus. The superficial peroneal nerve and sural nerve branches are meticulously protected. The extensor retinaculum is identified and mobilized. The capsule, ATFL, and CFL are incised, and the lateral gutter is inspected for osteochondral lesions or loose bodies. The fibular footprint is decorticated to bleeding bone to promote healing. Suture anchors (typically 2.5mm to 3.0mm) are placed into the distal fibula. The ATFL and CFL are then advanced and imbricated using horizontal mattress sutures with the ankle held in neutral dorsiflexion and slight eversion. The Gould modification involves mobilizing the inferior extensor retinaculum and pulling it over the repaired ligaments, suturing it to the fibula to provide secondary reinforcement and limit inversion.
Deltoid Ligament Exploration and Repair
In cases of an irreducible mortise following lateral fixation, medial exploration is mandatory. A longitudinal incision is made centered over the medial malleolus. The surgeon must carefully dissect through the subcutaneous tissue, protecting the saphenous nerve and vein. The flexor retinaculum is incised if necessary. The medial clear space is directly visualized. Frequently, the ruptured proximal stump of the deltoid ligament or the posterior tibial tendon is found incarcerated within the joint space. This enfolded tissue is extracted.

FIGURE 89-9A: Anteroposterior view showing a small avulsion fragment off the medial malleolus and a lateral shift of the talus.

FIGURE 89-9B: Oblique view demonstrating gross widening of the joint space on the medial side of the ankle.

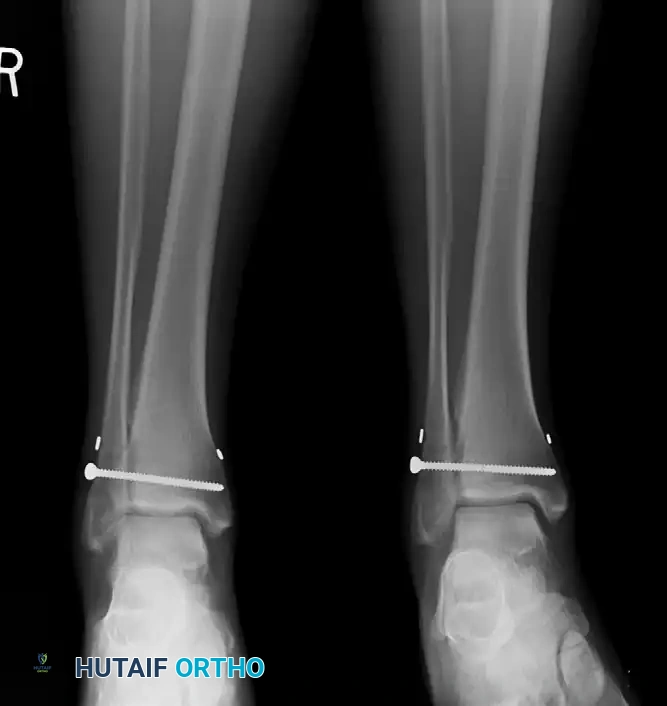
FIGURE 89-9C: Open reduction and internal fixation of the lateral malleolus. Note that the medial clear space must be evaluated post-fixation.

FIGURE 89-9D: Postoperative radiograph showing reduction of the talus into the ankle mortise. In this instance, the deltoid ligament did not require direct repair once the lateral column was restored.
If direct repair of the deltoid is required, suture anchors are placed into the medial malleolus. The deep layer of the deltoid is repaired first, followed by the superficial layer. It is critical to perform this repair with the talus anatomically reduced within the mortise to prevent over-tightening or capturing the talus in an eccentric position.
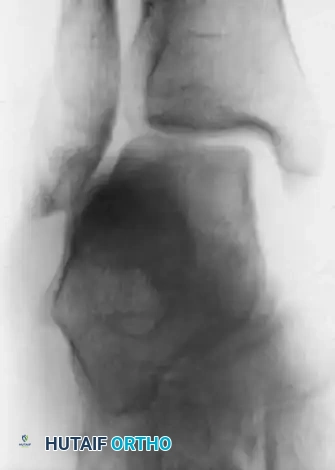
FIGURE 89-8A: Acute tear of the deltoid ligament associated with an oblique fracture of the fibula and lateral shift of the talus in the ankle mortise.

FIGURE 89-8B: Postoperative radiograph demonstrating restoration of the mortise after repair of the deltoid ligament and fibular fixation.
Syndesmotic Reduction and Fixation
The management of syndesmotic injuries requires absolute precision, as malreduction is the single greatest predictor of poor functional outcomes. We strongly advocate for direct open visualization of the anterior syndesmosis rather than relying solely on closed reduction and percutaneous clamping. An incision is made over the anterolateral distal leg, and the interval between the tibia and fibula is exposed. Debris and hematoma are cleared from the incisura.
The fibula is reduced into the incisura fibularis. A large reduction clamp is placed. Surgical Warning: The clamp must be placed precisely on the neutral axis of the tibia and fibula. Placing the clamp too anteriorly on the fibula or tibia will cause an iatrogenic anterior translation or internal rotation malreduction of the fibula. The ankle must be held in neutral to slight dorsiflexion during clamping to ensure the widest portion of the talar dome is seated within the mortise, preventing over-compression.
Intraoperative stress view demonstrating severe syndesmotic widening prior to fixation.

Post-fixation radiograph confirming anatomical restoration of the tibiofibular relationship.
Fixation Constructs: Screws vs. Suture Buttons
Historically, metal screws have been the gold standard. A 3.5-mm or 4.5-mm cortical screw is placed 2 to 3 cm proximal and parallel to the distal tibial articular surface, angled 20 to 30 degrees anteromedially. Quadricortical fixation is preferred for heavier patients or highly unstable injuries, while tricortical fixation allows for physiological micromotion.
Recently, there has been a paradigm shift toward dynamic fixation using suture button constructs (e.g., Arthrex TightRope). This device uses two metallic endobuttons secured by a No. 5 braided ultra-high-molecular-weight polyethylene suture. A drill hole is created across the syndesmosis, the implant is passed, and the suture is tensioned over the buttons.

FIGURE 89-14: Fixation of the syndesmosis utilizing a dynamic suture button construct.

Radiographic appearance of the suture button device maintaining the syndesmotic reduction while allowing physiological micromotion.
The advantages of suture button fixation include allowing for physiologic micromotion at the syndesmosis (potentially accelerating rehabilitation), eliminating the need for routine hardware removal, and reducing the risk of hardware breakage and subsequent osteolysis.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following the operative management of ankle ligament and syndesmotic injuries remain a significant clinical challenge. The surgeon must be adept at recognizing these complications early and instituting appropriate salvage protocols.
Malreduction of the syndesmosis is the most critical complication, historically reported in up to 16% to 39% of cases relying solely on fluoroscopic closed reduction. Malreduction alters the contact mechanics of the tibiotalar joint, leading to rapid cartilage wear. If recognized post-operatively, early revision surgery with open reduction and re-fixation is mandatory.
Hardware failure is common with rigid screw fixation. Syndesmotic screws are designed to hold the fibula in place during ligamentous healing; however, because the syndesmosis is a dynamic joint, rigid screws will eventually loosen or break upon resumption of full weight-bearing. While broken screws within the tibial canal are often asymptomatic, screws breaking at the clear space can cause localized osteolysis and pain, necessitating complex removal procedures.
Infection and wound dehiscence are particular concerns on the lateral aspect of the ankle due to the tenuous soft tissue envelope. Deep infections require aggressive surgical debridement, hardware removal (if stability allows or via staged procedures), and culture-directed intravenous antibiotic therapy.
At long-term follow-up, many patients with severe syndesmotic sprains develop heterotopic ossification or synostosis of the interosseous membrane. While often asymptomatic, in high-demand professional athletes, symptomatic ossification may require delayed surgical excision to allow a return to elite sports. In cases of chronic, painful instability or failed primary fixation, salvage procedures such as anatomical reconstruction using autologous grafts (e.g., gracilis tendon) or formal surgical arthrodesis of the syndesmosis may be required.
Summary Table of Complications and Salvage Strategies
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Treatment |
|---|---|---|---|
| Syndesmotic Malreduction | 16% - 39% (Closed) | Eccentric clamp placement; failure to open the joint; lack of CT verification. | Early revision ORIF; take-down of callus; open debridement of incisura. |
| Hardware Breakage (Screws) | 10% - 30% | Early weight-bearing on rigid screws; use of smaller diameter (3.5mm) screws. | Observation if asymptomatic; removal of symptomatic fragments; use of dynamic suture buttons. |
| Wound Dehiscence / Infection | 2% - 5% | Poor soft tissue envelope; smoking; diabetes; early aggressive ROM. | Local wound care; oral/IV antibiotics; surgical debridement; hardware removal if deep. |
| Tibiofibular Synostosis | 5% - 10% | Massive IOM tearing; bone debris left in the interval; aggressive early mobilization. | Observation if painless; delayed surgical excision (>6 months) if symptomatic in athletes. |
| Chronic Instability | 5% - 15% | Failure of ligament healing; unrecognized secondary restraints (deltoid) incompetence. | Allograft/autograft reconstruction; formal syndesmotic arthrodesis for end-stage failure. |
Phased Post-Operative Rehabilitation Protocols
Following operative stabilization of complex ankle ligamentous and syndesmotic injuries, a strict, phased rehabilitation protocol is absolutely essential to optimize functional outcomes and protect the surgical reconstruction. The rehabilitation timeline must be individualized based on the specific structures repaired, the rigidity of the fixation construct, and the patient's baseline physiological status.
Phase I: Maximum Protection (0-2 Weeks)
Immediately post-operatively, the patient is placed in a well-padded, short-leg splint with the ankle strictly immobilized in a neutral position. Strict non-weight-bearing (NWB) is enforced using crutches or a knee scooter. This phase is critical to protect the delicate soft tissue envelope, minimize edema, and allow the initial inflammatory phase of ligamentous healing to commence without disruption. Elevation above the level of the heart and aggressive cryotherapy are critical components to mitigate swelling and reduce narcotic consumption.
Phase II: Controlled Mobilization (2-6 Weeks)
At the first post-operative visit (10-14 days), sutures are removed, and the patient is transitioned to a controlled ankle motion (CAM) boot. The weight-bearing status during this phase is highly dependent on the fixation method. If rigid screw fixation was utilized for the syndesmosis, the patient typically remains NWB to prevent premature screw breakage. However, if a dynamic suture button construct was utilized, progressive partial weight-bearing may be initiated based on surgeon preference and the stability of the construct. Active, non-weight-bearing dorsiflexion and plantarflexion exercises are encouraged to prevent capsular stiffness and promote parallel alignment of the healing collagen fibers. Inversion and eversion are strictly prohibited to protect lateral and medial ligament repairs.
Phase III: Strengthening and Proprioception (6-12 Weeks)
During this phase, full weight-bearing (FWB) is progressively achieved. The CAM boot is gradually weaned, and the patient transitions to a supportive lace-up ankle brace. Physical therapy becomes aggressive,
