Comprehensive Introduction and Patho-Epidemiology
The management of the rheumatoid foot represents one of the most complex, multifaceted challenges in operative orthopaedics. Rheumatoid arthritis (RA) is a systemic, chronic autoimmune disease characterized by aggressive synovial inflammation and hyperplasia, which inevitably leads to capsular distension, ligamentous attenuation, and progressive articular destruction. In the foot and ankle, this profound biomechanical derangement manifests as a predictable, debilitating cascade of deformities that severely compromises the patient's ambulatory capacity and overall quality of life. The forefoot is particularly vulnerable; epidemiological studies indicate that up to 90% of patients with long-standing rheumatoid arthritis will develop clinically significant foot and ankle pathology, with forefoot symptoms frequently preceding hindfoot or large joint manifestations.
Historically, pain and swelling in the hindfoot and ankle have been correlated with severe limitation and disability—often more so than isolated pain and swelling of the forefoot. However, extensive clinical observation and patient-reported outcome measures reveal that the duration of the disease and the subjective experience of pain influence the patient's overall disability far more than the objective radiographic damage. The unrelenting nature of the disease process means that even with optimal medical management, the structural integrity of the foot is gradually undermined, leading to a loss of the critical weight-bearing architecture required for normal bipedal locomotion.
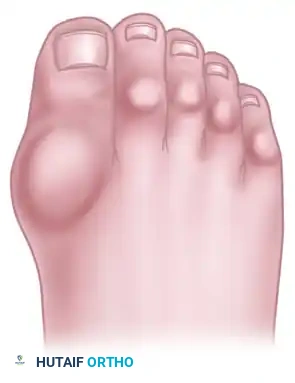
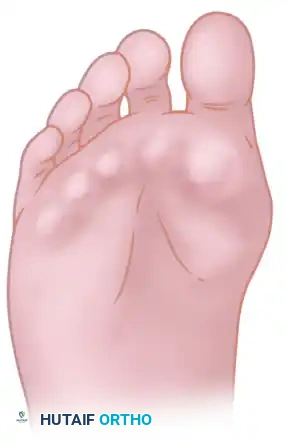
The classic "rheumatoid foot" presents with a highly characteristic constellation of deformities: severe hallux valgus, dorsal subluxation or frank dislocation of the lesser metatarsophalangeal (MTP) joints, claw toes, hammer toes, and the formation of painful adventitial bursae. As the proximal phalanges subluxate dorsally, the plantar metatarsal fat pad is drawn distally by the plantar plate and collateral ligament complex. This distal migration leaves the prominent metatarsal heads directly exposed to plantar pressure without their native fibrofatty cushion, leading to intractable plantar keratoses, severe metatarsalgia, and eventual ulceration. The orthopaedic surgeon must recognize that these structural changes are not isolated events but rather the end-stage manifestations of a systemic inflammatory process that requires a comprehensive, multidisciplinary approach to management.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy and biomechanics of the forefoot is an absolute prerequisite for successfully reconstructing the rheumatoid foot. The first metatarsophalangeal joint is a complex diarthrodial joint stabilized by the medial and lateral collateral ligaments, the sesamoid complex, and the strong plantar plate. In the rheumatoid patient, synovial hypertrophy (pannus) enzymatically degrades these static stabilizers. As the medial capsule attenuates, the abductor hallucis tendon shifts plantarward, losing its abductor moment and paradoxically becoming a flexor and pronator of the proximal phalanx. This allows the unopposed adductor hallucis to pull the hallux into severe valgus, while the first metatarsal head is driven medially, exacerbating the intermetatarsal angle and creating a prominent medial eminence.

In the lesser rays, the biomechanical failure is equally catastrophic. The lesser MTP joints are stabilized by the collateral ligaments and the plantar plate, which serves as the primary restraint against dorsal translation of the proximal phalanx. Rheumatoid synovitis causes massive distension of the joint capsule, leading to attenuation and eventual rupture of the plantar plate and collateral ligaments. Once the plantar plate fails, the extrinsic extensor tendons (extensor digitorum longus and brevis) gain a mechanical advantage over the intrinsic musculature (lumbricals and interossei). This imbalance forces the proximal phalanx into rigid dorsal extension, while the flexor digitorum longus and brevis pull the proximal and distal interphalangeal joints into flexion, creating the classic claw toe deformity.
The biomechanical consequences of these anatomic derangements are profound during the stance phase of gait. Normally, the windlass mechanism (described by Hicks) engages the plantar fascia during hallux dorsiflexion, elevating the longitudinal arch and creating a rigid lever for toe-off. In the rheumatoid foot, the dislocated MTP joints render the windlass mechanism entirely nonfunctional. The foot remains a flexible, unstable construct throughout terminal stance. Furthermore, patients with rheumatoid arthritis have been found to possess an altered "plantar pressure pain threshold," demonstrating decreased plantar foot sensitivity in all regions compared to healthy control groups. Because of this decreased sensitivity, pedobarography (plantar pressure mapping) is highly recommended early in the disease process, allowing the clinician to identify and correct excessive plantar loading before symptoms become severe or ulcerations develop.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention in the rheumatoid forefoot must be made judiciously, weighing the potential for functional improvement against the inherent risks of surgery in an immunosuppressed, systemically ill patient population. Conservative, nonoperative options—including extra-deep shoes, custom total-contact inserts, semirigid orthoses, and rocker soles—must be rigorously exhausted before surgical treatment is entertained. Medical management should be optimized in strict coordination with a rheumatologist. Surgery is indicated primarily for intractable pain, progressive deformity that precludes the use of commercially available or modified footwear, and the presence of impending or recurrent plantar ulcerations beneath the prominent metatarsal heads.
Contraindications to forefoot arthroplasty are absolute and must be respected to prevent catastrophic complications. Active localized or systemic infection is an absolute contraindication; any pre-existing ulcerations must be meticulously managed and ideally healed, or at minimum, free of active purulence and clinically uninfected before elective reconstruction. Severe peripheral vascular disease is another critical barrier to surgery. The healing potential of the distal extremities in rheumatoid patients is already compromised by vasculitis and chronic corticosteroid use; superimposing macrovascular insufficiency virtually guarantees wound dehiscence and gangrene.
Furthermore, patients who are medically unstable due to severe cardiopulmonary manifestations of rheumatoid arthritis (e.g., rheumatoid interstitial lung disease, pericarditis) or those with active, untreated rheumatoid vasculitis are not candidates for elective orthopaedic surgery. The surgeon must also carefully evaluate the patient's psychological readiness and functional expectations. Surgical correction of the rheumatoid deformity is palliative, not curative. Patients expecting a return to high-impact athletics or the ability to wear high-heeled, narrow toe-box shoes are poor candidates and must be extensively counseled to realign their expectations with surgical realities.
| Category | Indications for Forefoot Reconstruction | Absolute / Relative Contraindications |
|---|---|---|
| Clinical Symptoms | Intractable forefoot pain failing $>6$ months of conservative care; severe metatarsalgia. | Painless deformity well-managed with accommodative footwear (Relative). |
| Deformity / Soft Tissue | Severe hallux valgus overriding lesser toes; fixed dorsal dislocation of lesser MTP joints; recurrent plantar keratoses. | Active soft tissue infection; open, infected plantar ulcerations (Absolute). |
| Vascular Status | Adequate perfusion (ABI $/ge$ 0.7, absolute ankle pressure $/ge$ 90 mm Hg, palpable pedal pulses). | Severe peripheral arterial disease; absent pulses with ABI $< 0.5$ (Absolute). |
| Systemic Factors | Medically optimized RA; stable DMARD/biologic regimen; realistic patient expectations. | Active rheumatoid vasculitis; uncontrolled systemic disease; medical instability (Absolute). |
Pre-Operative Planning, Templating, and Patient Positioning
The complication rate in rheumatoid foot surgery is historically high (approximately 32%), emphasizing the absolute necessity for meticulous preoperative planning, comprehensive medical optimization, and extensive patient education. A cornerstone of this preparation is a rigorous vascular assessment. Careful attention must be paid to the presence and intensity of pedal pulses (dorsalis pedis and posterior tibial). If asymmetry exists, or if pulses are non-palpable, a peripheral vascular consultation and non-invasive arterial studies are mandatory. Objective parameters dictate that in nondiabetic patients with rheumatoid arthritis, an absolute ankle pressure of $/ge$ 90 mm Hg, or an Ankle-Brachial Index (ABI) of $/ge$ 0.7, is generally required to ensure forefoot wound healing in 90% of patients.
Equally critical is the dermatologic and neurologic inspection of the lower extremity. The skin of the foot and distal leg must be inspected for rheumatoid vasculitis, which presents as non-blanching macules and papules (often over the anterolateral distal tibia and dorsolateral foot), occasionally with a necrotic preulcerative center. The presence of rheumatoid nodules—caused by vasculitis of the subcutaneous connective tissue—should be documented, as they may interfere with surgical incisions or footwear postoperatively. Neurologically, the surgeon must assess for mononeuritis multiplex, an immune complex–mediated vasculitis of the peripheral nerves. Patients presenting with hyperesthesia (distinct from joint synovitis pain) must be examined for sensory, motor, or mixed deficits. If vasculitis is suspected, a rheumatology consult or skin biopsy is warranted prior to any surgical intervention.

Perioperative medication management requires a delicate balance between preventing disease flares and minimizing surgical site infections. While studies have shown that the perioperative use of methotrexate, gold salts, NSAIDs, or hydroxychloroquine does not significantly increase the risk of healing or infectious complications, biologic agents (e.g., TNF-alpha inhibitors) are typically held for one to two dosing cycles prior to surgery. Corticosteroid use requires specific protocol adjustments. If a patient is taking systemic corticosteroids, the tensile strength of the healing skin is severely compromised. Suture removal must be delayed to 3 weeks (21 days) or longer, rather than the customary 12 to 16 days, to prevent catastrophic wound dehiscence.

Patient positioning and intraoperative setup are standardized to optimize surgical exposure and efficiency. The patient is positioned supine on the operating table with a bump placed under the ipsilateral hip to internally rotate the leg, bringing the foot into a neutral, upward-facing position. A well-padded thigh tourniquet is applied to provide a bloodless surgical field, which is critical for identifying delicate neurovascular structures and ensuring precise bone resection. Preoperative templating of weight-bearing anteroposterior and lateral radiographs is essential to plan the extent of metatarsal resection, aiming to recreate a harmonious metatarsal cascade (the Maestro curve) that prevents postoperative transfer metatarsalgia.
Step-by-Step Surgical Approach and Fixation Technique
Forefoot arthroplasty in the rheumatoid patient is directed primarily at the severe metatarsophalangeal joint deformities. The overarching goals are to relieve pain, correct deformity, improve cosmesis, enhance ambulatory function, and allow the patient to wear a reasonable variety of footwear. For the lesser rays, resection of all five metatarsal heads, or fusion of the first MTP joint combined with resection of metatarsals 2 through 5, have both been shown to produce excellent results. Regardless of the specific surgical approach—whether utilizing a single transverse plantar incision (Hoffman approach) or multiple dorsal longitudinal incisions—adequate bony resection is mandatory. The phalanges must be allowed to realign loosely with the metatarsal remnants without any soft tissue tension.
Lesser Metatarsal Resection Arthroplasty
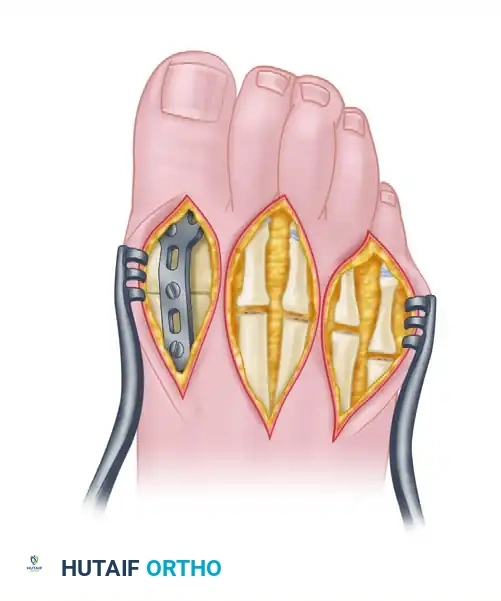
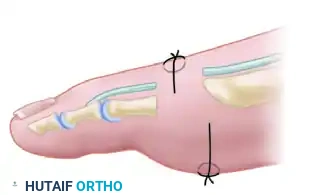
When utilizing dorsal longitudinal incisions, the surgeon typically makes one incision in the first web space to access the first and second MTP joints, and a second incision in the third web space to access the third, fourth, and fifth MTP joints. The extensor tendons are identified and either lengthened or tenotomized depending on the severity of the contracture. A complete dorsal capsulotomy is performed, and the collateral ligaments are released to allow delivery of the metatarsal head into the wound. The metatarsal neck is then osteotomized utilizing an oscillating saw. It is critical that the osteotomy is directed from dorsal-distal to plantar-proximal; this beveling ensures that the plantar aspect of the metatarsal stump does not present a sharp spike to the plantar skin during weight-bearing.

When performing this resection arthroplasty, the surgeon must carefully contour the remaining metatarsal necks. Unequal lengths of the metatarsal remnants, or metatarsals that do not cascade in a gentle, parabolic curve from metatarsals two through five, will inevitably result in transfer metatarsalgia and a severely compromised outcome. The second metatarsal should be the longest, with a sequential shortening of the third, fourth, and fifth metatarsals. Furthermore, any bony fragments or osteophytes left in the forefoot weight-bearing pad will act as symptomatic pebbles, causing severe localized pain. The stumps must be meticulously rasped smooth.

First Metatarsophalangeal Joint Arthrodesis
For the rheumatoid hallux, arthrodesis of the first MTP joint is the undisputed gold standard. This approach yields highly satisfactory results in 80% to 90% of patients. Through a dorsal longitudinal incision over the first MTP joint, the extensor hallucis longus is retracted laterally. The joint capsule is excised, and the severely degenerated articular surfaces of the first metatarsal head and the base of the proximal phalanx are prepared. Modern techniques favor the use of cup and cone reamers to create congruent, cancellous bone surfaces that allow for multi-planar adjustment of the fusion angle while maximizing the surface area for osteogenesis.

The success of a first MTP fusion relies entirely on precise spatial positioning. Improper alignment will lead to gait dysfunction, interphalangeal joint arthritis, and transfer lesions. The hallux must be positioned in approximately 20 degrees of valgus to sit parallel to the second toe. In the sagittal plane, it should be placed in 30 degrees of dorsiflexion in reference to the first metatarsal axis, which equates to approximately 10 to 15 degrees of dorsiflexion in reference to the plantar aspect of the foot (the floor). Finally, the hallux must be placed in absolute neutral rotation, ensuring the toenail faces directly dorsal. Fixation is most robustly achieved using a low-profile dorsal titanium plate in combination with a plantar-to-dorsal interfragmentary lag screw, providing rigid biomechanical stability that permits early heel-weight-bearing.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the complication rate in rheumatoid forefoot reconstruction remains higher than in the osteoarthritic population due to the systemic nature of the disease and the immunosuppressive medications required for its management. Wound healing complications are the most frequent adverse events, occurring in up to 10-15% of patients. The chronic use of systemic corticosteroids fundamentally alters collagen synthesis and cross-linking, leading to a fragile soft-tissue envelope. Superficial wound dehiscence or marginal necrosis must be managed aggressively with local wound care, offloading, and occasionally, negative pressure wound therapy. Deep infection, while less common (2-5%), is a devastating complication that may require hardware removal, extensive débridement, and prolonged intravenous antibiotic therapy.

Nonunion of the first MTP joint arthrodesis occurs in approximately 5-10% of cases. Fortunately, many of these nonunions are asymptomatic fibrous unions that do not require further surgical intervention. However, if a nonunion is painful and accompanied by hardware failure or loss of alignment, revision arthrodesis with autologous bone grafting (often harvested from the proximal tibia or iliac crest) and robust revision plate fixation is mandated. Another significant complication is transfer metatarsalgia, which arises from an improperly constructed metatarsal cascade. If a lesser metatarsal stump is left excessively long, it will bear a disproportionate amount of weight, leading to severe plantar pain and recurrent keratosis.

Recurrent deformity of the lesser toes, often described as "floppy toes" or recurrent dorsal subluxation, is a consequence of inadequate initial bone resection or progressive soft-tissue laxity. Insufficient relaxation of the soft tissues around the MTP joints due to inadequate bone resection will severely compromise the result, leading to recurrent dorsal subluxation and stiffness. Salvage management for recurrent lesser toe deformity typically involves returning to the operating room for further resection of the metatarsal stumps, syndactylization of the flail toes, or in extreme cases of severe instability, amputation of the non-functional digits to allow for better shoe fit and pain relief.
| Complication | Estimated Incidence | Pathophysiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Wound Dehiscence / Delayed Healing | 10 - 15% | Corticosteroid use; microvascular disease; excessive soft tissue tension. | Prolonged suture retention (21+ days); local wound care; offloading; secondary intention healing. |
| First MTP Nonunion | 5 - 10% | Poor bone quality; inadequate fixation; methotrexate/biologic interference; smoking. | Observation if asymptomatic; revision arthrodesis with bone graft and robust plating if painful. |
| Transfer Metatarsalgia | 10 - 20% | Disruption of the Maestro curve; inadequate resection of a specific metatarsal head. | Custom orthotics with metatarsal relief pads; revision surgery to shorten the offending metatarsal stump. |
| Recurrent Lesser Toe Deformity | 20 - 30% (Long-term) | Progressive rheumatoid soft-tissue attenuation; inadequate initial bony resection. | Accommodative footwear; revision resection arthroplasty; toe syndactyly or amputation for flail digits. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation of the rheumatoid foot requires a carefully phased, multidisciplinary approach to ensure optimal healing while preventing the rapid deconditioning that can occur in this vulnerable patient population. Phase I encompasses the immediate postoperative period (0 to 2 weeks). Upon completion of the surgery, the foot is placed in a bulky, compressive Robert Jones dressing to mitigate the severe postoperative edema characteristic of rheumatoid patients. Routine use of a prophylactic broad-spectrum antibiotic is required 30 minutes prior to incision, intraoperatively, and for 48 to 72 hours postoperatively. The patient is instructed to elevate the feet to the maximal tolerable level (above the level of the heart) for the first 48 to 72 hours. Weight-bearing is strictly restricted to heel-touch or non-weight-bearing utilizing an offloading postoperative shoe or boot, depending on the stability of the fixation and the quality of the host bone.

Phase II (2 to 6 weeks) marks the critical period of soft tissue healing. Because of the compromised tensile strength of the skin in patients on systemic corticosteroids, suture removal must be delayed to 3 weeks (21 days) or longer, rather than the customary 12 to 16 days. Premature suture removal is a common error that leads to catastrophic wound dehiscence. Once the incisions are fully healed, the patient may gradually increase weight-bearing in a stiff-soled postoperative shoe. If longitudinal K-wires were utilized to stabilize the lesser toes (a common adjunct in resection arthroplasty), meticulous pin site care is required until the pins are removed in the clinic, typically between 3 and 4 weeks postoperatively. Active and passive range of motion of the ankle and hindfoot are encouraged to prevent stiffness, though the forefoot remains protected.
Phase III (6 to 12 weeks and beyond) focuses on the transition back to functional ambulation and permanent footwear modification. Radiographic evaluation is performed at 6 to 8 weeks to confirm the progression of the first MTP arthrodesis and the maintenance of the lesser metatarsal cascade. Once clinical and radiographic union is evident, the patient is transitioned into a wide, extra-depth accommodative shoe. Collaboration with a skilled orthotist or pedorthist is essential at this stage. Custom total-contact inserts are fabricated to distribute weight evenly across the plantar surface, protecting the metatarsal stumps from excessive focal pressure. Patients must be educated that they will likely require these specialized orthotics and accommodative footwear for the remainder of their lives to protect the surgical reconstruction and prevent the recurrence of painful callosities.
Summary of Landmark Literature and Clinical Guidelines
The evolution of forefoot arthroplasty in the rheumatoid patient is deeply rooted in a rich history of orthopaedic literature. Early pioneers such as Hoffman (1911) and Clayton (1960) established the foundational principles of pan-metatarsal head resection. Hoffman's original description of a single transverse plantar incision for the excision of all five metatarsal heads provided dramatic pain relief for patients with severe, crippling deformities. Clayton later modified this approach, advocating for a dorsal approach and the concurrent resection of the bases of the proximal phalanges to ensure adequate soft-tissue relaxation. While these excisional arthroplasties were revolutionary, long-term follow-up revealed significant issues with recurrent hallux valgus and progressive medial column instability.
The paradigm shift toward combining lesser metatarsal head resection with first MTP joint arthrodesis was championed by master surgeons such as Coughlin and Mann in the late 20th century. Their seminal long-term outcome studies definitively demonstrated that fusing the first MTP joint provides a stable medial column, which acts as a buttress against the lateral drift of the lesser toes, significantly reducing the rate of recurrent deformity. Comparisons between first MTP arthrodesis and excisional arthroplasty (e.g., the Keller procedure) heavily favor arthrodesis. Arthrodesis provides superior pain relief, better dynamic balance, improved cosmesis, and a greater ability to fit the foot into a normal shoe. Modern prospective, randomized studies (such as Grondal et al.) comparing first MTP arthrodesis to first metatarsal head resection found no significant difference in lateral forefoot pressure, but the consensus remains that fusion is a more definitive and satisfactory procedure.

From a comprehensive review of published series on forefoot arthroplasty, several definitive conclusions emerge regarding long-term prognosis. In 80% to 90% of patients, a highly satisfactory result can be expected in the short to medium term. Pain relief, walking endurance, and footwear variety are significantly improved. However, inevitable deterioration occurs; after 3 to 5 years, the percentage of excellent objective results begins to decrease. Recurrence of hallux valgus (if not fused), recurrent plantar callosities, and dorsal posturing of the toes often become apparent. Interestingly, although objective deformity has been reported to recur in more than 50% of patients over time, up to 97% of patients remain subjectively satisfied with their results. This discrepancy is likely because many rheumatoid patients gradually reduce their overall level of physical activity due to the generalized, systemic nature of the disease, rendering the recurrent foot deformities far less symptomatic than they would be in a highly active individual.
In conclusion, surgical reconstruction of the rheumatoid forefoot is a highly effective, albeit palliative, intervention. By adhering to strict preoperative optimization, respecting the fragile soft-tissue envelope, executing precise bony resections and fusions, and understanding the profound biomechanical alterations inherent to the disease, the orthopaedic surgeon can reliably restore ambulatory function and dramatically improve the quality of life for these complex patients.
