Comprehensive Introduction and Patho-Epidemiology
Keratotic lesions of the foot—encompassing hard corns (heloma durum), soft corns (heloma molle), and intractable plantar keratoses (IPK)—represent a hyperkeratotic physiological response to focal, repetitive biomechanical stress. While frequently dismissed in primary care settings as minor dermatological nuisances, these lesions are fundamentally orthopedic in nature. They arise from underlying osseous prominences, structural forefoot deformities, or altered forefoot kinematics that subject the glabrous skin of the foot to pathological levels of shear and compressive forces. For the practicing orthopedic surgeon, successful management requires a paradigm shift from superficially treating the cutaneous symptom to definitively addressing the underlying structural and biomechanical pathology. Failure to recognize the osseous etiology inevitably leads to rapid recurrence, profound patient dissatisfaction, and severe potential complications.
The pathophysiology of these lesions is rooted in the physiological behavior of the stratum corneum. In response to intermittent, localized pressure and friction, the basal layer of the epidermis accelerates cellular proliferation. This results in a thickened stratum corneum, which initially serves as a protective mechanism. However, as the hyperkeratotic mass enlarges, it becomes a space-occupying lesion that paradoxically increases the focal pressure against the underlying bony prominence. This vicious cycle leads to the formation of a dense, centralized keratinous core that drives deep into the dermis, compressing cutaneous nerve endings and generating severe, sharp pain during weight-bearing or shoe wear. Beneath the lesion, chronic shear forces often lead to the development of a painful adventitial bursa, which can become inflamed, fibrotic, or infected.
Epidemiologically, keratotic foot lesions are overwhelmingly prevalent in female populations, a demographic skew directly correlated to the widespread use of restrictive, narrow-toe-box, and high-heeled footwear. Such footwear forcefully compresses the forefoot, exacerbating underlying deformities such as hallux valgus, hammer toes, and claw toes. Age is an independent risk factor; as the plantar fat pad atrophies and migrates distally with advancing age, the metatarsal heads lose their primary soft-tissue cushioning, dramatically increasing the incidence of IPKs in the geriatric population.
In immunocompromised or diabetic populations, the patho-epidemiology takes on a limb-threatening dimension. Peripheral neuropathy deprives the patient of the protective pain sensation that would normally prompt offloading or footwear modification. Consequently, the keratotic lesion acts as a continuous source of deep tissue trauma. The hyperkeratotic plaque ultimately causes ischemic necrosis of the underlying dermis, leading to subclinical tissue breakdown, abscess formation, and eventual full-thickness ulceration. In these vulnerable cohorts, what begins as a simple heloma durum or molle can rapidly escalate into deep space infection, osteomyelitis, and the need for digital or ray amputation. Therefore, aggressive and definitive orthopedic management is not merely elective but highly limb-salvaging.
Detailed Surgical Anatomy and Biomechanics
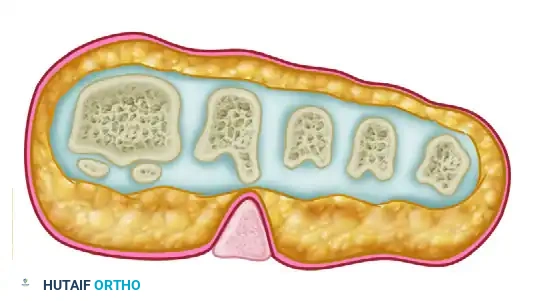
A profound understanding of forefoot anatomy and biomechanics is the cornerstone of effectively managing keratotic lesions. The forefoot functions as a complex, dynamic weight-bearing unit where forces are distributed across the metatarsal parabola during the stance phase of gait. The first ray (first metatarsal and hallux) is biomechanically designed to bear approximately 50% of the forefoot's load during the propulsive phase, while the remaining 50% is distributed relatively evenly across the lesser metatarsals. The metatarsophalangeal (MTP) joints are stabilized by a robust capsuloligamentous complex, including the collateral ligaments, the deep transverse metatarsal ligament, and the plantar plate—a thick, fibrocartilaginous structure that resists dorsal subluxation of the proximal phalanx.
The development of lesser metatarsal callosities and IPKs is frequently a secondary manifestation of first ray pathology, most notably hallux valgus or hallux rigidus. When the first ray becomes structurally incompetent or hypermobile, its weight-bearing capacity is severely compromised. This biomechanical failure necessitates a lateral shift of ground reaction forces, a phenomenon known as transfer metatarsalgia. The second and third metatarsal heads, which are anatomically fixed and lack the robust sesamoid complex of the first ray, are suddenly subjected to pathological loads. This extrinsic overload drives the plantar condyles of the metatarsal heads into the plantar soft tissues, initiating the hyperkeratotic cascade.
The anatomy of the interdigital web spaces is particularly relevant to the formation of heloma molle (soft corns). The fourth web space is the most frequent site of these highly painful lesions. Anatomically, this space is constrained, and the osseous architecture of the fourth and fifth rays frequently predisposes them to impingement. A slightly short fifth metatarsal places the head of the fifth proximal phalanx in direct transverse alignment with the lateral base of the fourth proximal phalanx.

When extrinsic lateral pressure from a narrow toe box or a severe hallux valgus deformity forces the fifth toe into adduction, these two bony prominences act as a mortar and pestle.
The skin of the web space is caught between the medial condyle of the head of the fifth proximal phalanx and the lateral base of the fourth proximal phalanx. The confined, diaphoretic environment of the web space macerates the resulting hyperkeratosis, producing the characteristic "soft" corn.

Regarding hard corns (heloma durum), the pathoanatomy is intimately tied to sagittal plane deformities of the lesser toes, specifically hammer toe and claw toe deformities. A hammer toe is characterized by MTP joint extension and proximal interphalangeal (PIP) joint flexion. This abnormal posture elevates the dorsal aspect of the PIP joint, specifically the head and neck of the proximal phalanx, creating a focal point of friction against the shoe vamp. The extensor digitorum longus tendon, which runs centrally over the PIP joint, is often contracted, further rigidifying the deformity. The skin overlying the PIP joint is thin and lacks subcutaneous fat, leaving the stratum corneum highly vulnerable to shear forces and subsequent hard corn formation.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention for keratotic foot lesions must be predicated on a rigorous evaluation of the patient's symptoms, structural pathology, and response to conservative management. Initial management must remain strictly nonoperative until the patient has exhausted a variety of conservative modalities. These include friction-absorbing silicone sleeves, wide toe-box footwear, custom orthoses with metatarsal offloading pads, and routine podiatric debridement. Nonoperative management is considered to have failed only if the patient remains highly symptomatic despite compliant use of these devices, or if the daily application becomes excessively detrimental to their quality of life.
Surgical indications are absolute in the presence of impending tissue breakdown. In neuropathic patients, a pre-ulcerative lesion—often heralded by sub-keratotic hemorrhage or a localized adventitial bursitis—requires urgent prophylactic surgery to prevent full-thickness ulceration and subsequent osteomyelitis. In sensate patients, recalcitrant pain that alters the patient's gait mechanics (antalgic gait) and causes secondary proximal joint pain (e.g., knee or hip pain due to altered kinematics) constitutes a strong indication for osseous resection or realignment. Furthermore, if a keratotic lesion is accompanied by a rigid, non-reducible structural deformity (such as a fixed hammer toe or a severe hallux valgus causing transfer metatarsalgia), surgical correction of the primary deformity is indicated to achieve long-term resolution of the secondary skin lesion.
Contraindications to surgical intervention are primarily related to systemic host factors that preclude safe wound healing. Severe peripheral vascular disease (PVD) is an absolute contraindication to elective forefoot surgery. Ankle-brachial index (ABI) less than 0.5, absent pedal pulses, or transcutaneous oxygen tension (TcPO2) less than 30 mmHg indicate insufficient perfusion for incisional healing, risking postoperative gangrene. Uncontrolled diabetes mellitus (HbA1c > 8.0%) significantly increases the risk of postoperative infection and nonunion. Active local infection, unless the surgery is specifically designed for incision, drainage, and debridement of an infected corn, precludes elective osseous realignment.
| Parameter | Indications for Surgery | Contraindications for Surgery |
|---|---|---|
| Clinical Symptoms | Recalcitrant pain failing 3-6 months of conservative care; antalgic gait. | Asymptomatic lesions; pain easily managed with simple shoe modifications. |
| Tissue Status | Pre-ulcerative changes (sub-keratotic hemorrhage); recurrent ulceration in neuropathic feet. | Active cellulitis or deep space abscess (relative contraindication for elective osseous procedures; requires I&D first). |
| Deformity Type | Rigid, non-reducible structural deformities (fixed hammer toe, long metatarsal). | Flexible deformities fully correctable with orthoses or taping. |
| Vascular Status | Intact pedal pulses; ABI > 0.9; biphasic/triphasic Doppler signals. | Severe PVD (ABI < 0.5); absent pulses; TcPO2 < 30 mmHg (Absolute). |
| Systemic Health | Well-controlled diabetes (HbA1c < 7.5%); medically optimized. | Uncontrolled diabetes (HbA1c > 8.0%); severe immunocompromise; non-compliant patient. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is critical for achieving optimal surgical outcomes and minimizing the risk of recurrence or iatrogenic transfer lesions. The clinical evaluation begins with a meticulous physical examination. The surgeon must differentiate a true intractable plantar keratosis (IPK) from a verruca plantaris (plantar wart). An IPK is characterized by a central keratinous core that is intensely painful upon direct palpation but less painful with lateral compression (the "pinch test"). Furthermore, normal dermatoglyphics (skin lines) will pass through an IPK but are interrupted by a verruca.

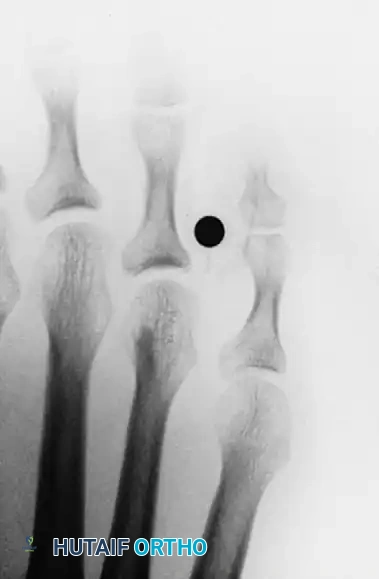
Weight-bearing radiographs of the foot (anteroposterior, lateral, and sesamoid axial views) are mandatory. These images allow the surgeon to assess the metatarsal parabola, identify excessively long or plantarflexed metatarsals, and evaluate the presence of concomitant hallux valgus or MTP joint subluxation.
For IPKs, the lateral view may demonstrate a prominent plantar condyle driving into the soft tissues.

Pedobarography (dynamic footprint analysis) is an invaluable, though not strictly mandatory, adjunct in preoperative planning. It provides a highly accurate, quantitative map of plantar pressures during the stance phase of gait, allowing the surgeon to precisely correlate the hyperkeratotic lesion with the specific area of peak focal pressure.
When planning an osteotomy, such as a Weil osteotomy for a long metatarsal, preoperative templating is essential. The surgeon must calculate the exact amount of shortening required to restore a harmonious metatarsal parabola (typically the second metatarsal should be slightly longer or equal to the first, and a smooth cascade should follow to the fifth). Over-shortening a metatarsal is a catastrophic error that will inevitably lead to a severe transfer lesion on the adjacent ray. The angle of the osteotomy cut must also be planned; a cut strictly parallel to the weight-bearing surface achieves pure shortening, whereas an angled cut will induce a degree of plantarflexion or elevation, depending on the orientation.
Patient positioning for forefoot surgery is standardized but requires careful attention to detail. The patient is placed in the supine position with the feet positioned at the very edge of the operating table to allow unrestricted access for the surgeon and the fluoroscopy unit (C-arm). A bump may be placed under the ipsilateral hip to correct natural external rotation of the lower extremity, ensuring the foot rests in a neutral, plantigrade position. A pneumatic calf tourniquet or an ankle tourniquet is applied over copious soft padding. Regional anesthesia, typically an ultrasound-guided popliteal block supplemented with a saphenous nerve block, or a highly specific ankle block, is administered to provide profound intraoperative anesthesia and extended postoperative analgesia.
Step-by-Step Surgical Approach and Fixation Technique
Interdigital Soft Corns (Heloma Molle): Fourth Web Space Condylectomy
When conservative measures fail for a recalcitrant fourth web space soft corn, surgical excision of the underlying bony prominence is required. The procedure aims to eliminate the osseous impingement while preserving the structural integrity of the toes.
- Incision and Exposure: A dorsal longitudinal incision is made directly over the fourth web space, carefully biased toward the toe containing the primary osseous prominence (usually the medial aspect of the fifth proximal phalanx). The incision is deepened through the subcutaneous tissues using blunt dissection to protect the delicate dorsal cutaneous nerves. The interdigital neurovascular bundle, located in the plantar aspect of the web space, must be meticulously identified and protected with a small retractor.
- Osseous Resection: The capsule overlying the prominent medial condyle of the fifth proximal phalanx head is incised longitudinally and elevated via sharp subperiosteal dissection. Using a micro-sagittal saw or a sharp, double-action rongeur, a partial condylectomy is performed. The resection must be generous enough to remove the flare of the condyle completely, making the bone flush with the diaphyseal shaft.
- Dynamic Assessment: The surgeon must manually compress the fourth and fifth toes together to ensure that absolutely no osseous impingement remains. If the lateral base of the fourth proximal phalanx is also prominent, a similar conservative resection of this flare is performed through the same incision.
- Closure: The wound is irrigated with copious sterile saline to remove all bone debris, which could act as a nidus for heterotopic ossification. The skin is closed with non-absorbable monofilament sutures (e.g., 4-0 nylon) using a simple interrupted or vertical mattress technique. A bulky, compressive web-space dressing utilizing lamb's wool or a specialized foam spacer is applied to prevent hematoma formation and ensure the web space heals in an open, non-macerated position.
Intractable Plantar Keratosis (IPK): Plantar Condylectomy vs. Weil Osteotomy
The surgical approach for an IPK depends entirely on whether the pathology is an isolated prominent condyle (requiring a DuVries arthroplasty) or a globally plantarflexed/long metatarsal (requiring a Weil osteotomy).
Isolated Plantar Condylectomy (DuVries Approach)
- Incision: A dorsal longitudinal incision is made over the affected MTP joint. Plantar incisions are strictly avoided, as plantar scars frequently become hypertrophic and more painful than the original IPK.
- Capsulotomy and Release: The extensor digitorum longus tendon is identified and retracted laterally (or lengthened via a Z-plasty if contracted). A dorsal capsulotomy is performed. The collateral ligaments are sharply released from the metatarsal head to allow acute plantarflexion of the toe, fully exposing the metatarsal head.
- Resection: A McGlamry elevator is passed plantarly to free the plantar plate and flexor tendons from the metatarsal head. Using a micro-sagittal saw, the prominent plantar condyle (typically the lateral condyle, as it bears more weight during pronation) is resected flush with the metatarsal shaft. Approximately 2-3 mm of plantar bone is removed. The edges are smoothed with a rasp.
- Closure: The capsule is repaired with absorbable sutures, ensuring the toe is resting in neutral alignment. The skin is closed, and a compressive dressing is applied.
Metatarsal Shortening/Elevating Osteotomy (Weil Osteotomy)
- Exposure: Through a similar dorsal approach, the metatarsal head and distal shaft are exposed.
- Osteotomy: A micro-sagittal saw is used to create an intra-articular osteotomy starting at the dorsal margin of the articular cartilage and exiting proximally in the plantar metatarsal shaft. The cut must be perfectly parallel to the plantar weight-bearing surface of the foot.
- Translation and Fixation: The capital fragment is translated proximally by the pre-calculated amount (typically 2-4 mm) to shorten the ray. Because the cut is parallel to the ground, proximal translation inherently elevates the metatarsal head, effectively offloading the IPK. The osteotomy is provisionally held with a K-wire and definitively fixed with one or two 2.0 mm or 2.4 mm snap-off cortical screws directed dorsal-proximal to plantar-distal.
- Plantar Plate Repair: If a plantar plate tear is identified, it is repaired concurrently to prevent postoperative dorsal subluxation (floating toe).
Hard Corns (Heloma Durum): PIP Joint Resection Arthroplasty
- Incision: An elliptical incision is made directly over the hard corn on the dorsolateral aspect of the PIP joint. The hyperkeratotic tissue is excised en bloc with the skin ellipse, completely removing the cutaneous pathology.
- Joint Exposure: The extensor tendon is transected transversely or split longitudinally. The collateral ligaments of the PIP joint are sharply divided, allowing the joint to be "shotgunned" (hinged open plantarly), exposing the articular surfaces.
- Bone Resection: Using a bone-cutting forceps or a micro-sagittal saw, the distal portion of the proximal phalanx (the head and neck) is resected. The resection must be perpendicular to the long axis of the phalanx.
- Evaluation and Closure: Adequate bone must be removed so that the toe is flaccid and no longer impinges against the shoe or adjacent toes. The extensor tendon is generally not repaired, allowing it to retract. The skin is closed with simple interrupted sutures. The toe is splinted in a corrected, straight position using cohesive bandages or buddy-taped to the adjacent toe.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following the operative management of keratotic lesions are well-documented. The most frustrating complication for both surgeon and patient is the recurrence of the keratotic lesion. Recurrence is almost universally due to an inadequate resection of the osseous prominence or a failure to address the primary deforming force (e.g., performing a lesser metatarsal osteotomy without correcting a severe hallux valgus).
Transfer metatarsalgia is a highly specific and problematic complication associated with metatarsal osteotomies, particularly the Weil osteotomy. If a metatarsal is excessively shortened, the adjacent metatarsal heads will bear the brunt of the forefoot load, rapidly developing a new, iatrogenic IPK. This highlights the critical importance of preoperative templating and precise intraoperative execution.
The "floating toe" deformity is another frequent sequela of the Weil osteotomy, occurring in up to 15-30% of cases. Proximal translation of the metatarsal head alters the intrinsic muscle biomechanics, specifically loosening the plantar plate and intrinsic flexors while relatively tightening the extensors. This results in a dorsal contracture of the MTP joint, causing the toe to elevate off the ground during stance.
Infections, while relatively rare in healthy patients (incidence < 2%), can be catastrophic in diabetic or immunocompromised individuals. Postoperative deep space infections require aggressive surgical debridement and intravenous antibiotic therapy. Neurovascular injury, particularly to the delicate interdigital nerves during web space procedures, can result in painful neuromas or permanent digital numbness.
| Complication | Estimated Incidence | Etiology/Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Recurrent Keratosis | 5% - 10% | Inadequate bone resection; uncorrected primary deformity (e.g., Hallux Valgus). | Revision osteotomy/condylectomy; definitive correction of the primary first ray pathology. |
| Transfer Metatarsalgia | 10% - 15% | Over-shortening of a metatarsal during Weil osteotomy; altering the metatarsal parabola. | Conservative offloading first; if failed, elevating osteotomy of the newly affected adjacent ray. |
| Floating Toe Deformity | 15% - 30% | Altered intrinsic biomechanics post-Weil osteotomy; failure to repair plantar plate. | Flexor-to-extensor tendon transfer (Girdlestone-Taylor procedure); MTP joint capsular release. |
| Nonunion / Malunion | < 2% | Poor fixation technique; premature weight-bearing; smoking; uncontrolled diabetes. | Revision internal fixation with bone grafting; prolonged immobilization. |
| Deep Space Infection | 1% - 3% | Diabetic neuropathy; poor wound hygiene; hematoma formation in web spaces. | Urgent surgical I&D; targeted IV antibiotics; potential ray amputation if osteomyelitis develops. |
Phased Post-Operative Rehabilitation Protocols
Regardless of the specific procedure performed, strict adherence to a phased postoperative rehabilitation protocol is essential for optimal wound healing, minimizing edema, and preventing recurrence. The rehabilitation timeline is dictated by the biological healing of the soft tissues and, if applicable, the osseous union of osteotomies.
Phase I: Acute Healing (Weeks 0-2)
The primary goals during this phase are wound healing, edema control, and pain management. Patients are typically allowed immediate heel-weight-bearing or flat-foot weight-bearing in a rigid postoperative shoe. The rigid sole prevents dorsiflexion of the MTP joints, protecting capsular repairs and osteotomies. Strict elevation of the operative limb above the level of the heart is mandated for the first 72 hours to minimize throbbing pain and swelling. Dressings must remain clean, dry, and intact. For web space procedures, a specialized spacer (such as sterile gauze or lamb's wool) must be maintained between the toes to prevent maceration and ensure the web space heals in an open configuration. Sutures are generally removed at 14 to 21 days, contingent upon the vascular status of the patient and the complete epithelialization of the wound edges.
Phase II: Transitional Rehabilitation (Weeks 2-6)
Once the sutures are removed and the incisions are stable, patients begin a guided transition back to normal footwear. If a Weil osteotomy was performed, aggressive plantarflexion taping of the involved toe is initiated and maintained for 4 to 6 weeks. This taping protocol is critical to counteract the extensor overpull and mitigate the risk of developing a floating toe deformity. Active and passive range-of-motion exercises of the MTP and PIP joints are introduced to prevent arthrofibrosis. Patients are instructed to wear wide toe-box, stiff-soled athletic shoes. High-impact activities and prolonged standing are strictly prohibited. Radiographs are obtained at the 6-week mark to confirm osseous union of any osteotomies.
Phase III: Long-Term Maintenance (Weeks 6 and Beyond)
Following complete clinical and radiographic healing, the focus shifts to long-term prevention. Patients must be thoroughly educated that while surgery successfully corrects the osseous prominence, returning to poor, restrictive footwear will inevitably cause recurrent skin irritation and subsequent keratosis formation. Transitioning permanently to wide toe-box shoes with a deep vamp is highly recommended. For patients who presented with transfer metatarsalgia, custom-molded orthotics with specific metatarsal offloading pads or a metatarsal bar are prescribed to permanently redistribute plantar pressures and protect the lesser metatarsal heads.
Summary of Landmark Literature and Clinical Guidelines
The surgical management of keratotic foot lesions is supported by a robust body of orthopedic literature that has evolved from simple soft-tissue excisions to sophisticated biomechanical realignments.
The foundational principles of plantar condylectomy were established by DuVries, who demonstrated that isolated plantar keratoses beneath the metatarsal heads could be effectively managed by resecting the prominent plantar condyle via a dorsal approach. His landmark texts emphasized the avoidance of plantar incisions, a principle that remains a strict clinical guideline today due to the high morbidity associated with plantar scarring.
The management of transfer metatarsalgia and IPKs was revolutionized by the introduction of the Weil osteotomy. Coughlin et al. published extensive outcome studies validating the Weil osteotomy as a highly effective procedure for shortening and elevating the lesser metatarsals. Their research highlighted that while the procedure reliably resolves the plantar keratosis, surgeons must be acutely aware of the biomechanical shifts that lead to floating toe deformities, advocating for concurrent plantar plate repair and postoperative plantarflexion taping.
Furthermore, the intimate relationship between first ray pathology and lesser toe keratoses was definitively quantified by Lee et al. Their landmark studies demonstrated that over 90% of patients with lesser metatarsal callosities experienced significant, long-term improvement or complete resolution of their pain following the anatomical correction of a concomitant hallux valgus deformity alone, without direct surgical intervention on the lesser rays. This established the modern clinical guideline that first ray stability must be achieved before, or concurrently with, addressing lesser ray keratotic lesions.
In conclusion, the comprehensive surgical management of keratotic foot lesions demands a rigorous understanding of forefoot biomechanics, meticulous preoperative planning, and precise surgical execution. By accurately identifying and resecting the offending osseous prominences—whether through condylectomy, arthroplasty, or corrective osteotomy—the orthopedic surgeon can provide definitive, limb-salvaging relief for these debilitating lesions.
