Patient Presentation & History
A 32-year-old male, a previously healthy, non-smoking construction worker, presented to the emergency department following a high-energy motorcycle collision with a stationary object. He was an unrestrained rider. The mechanism of injury involved direct impact to the lower leg combined with significant rotational and axial loading forces. He reported immediate, severe pain in his left lower leg, inability to bear weight, and observed gross deformity.
Upon arrival, he was hemodynamically stable. His medical history was unremarkable, with no known allergies or regular medications. There was no history of diabetes, peripheral vascular disease, osteoporosis, or chronic steroid use. His social history was significant for occasional alcohol consumption but denied recreational drug use. He was right-hand dominant.
Initial assessment revealed a closed injury to the left lower leg, with no apparent skin compromise or gross open wounds. However, significant swelling and obvious angulation were present in the mid-diaphyseal region of the left tibia. There were no immediate concerns for associated major injuries to the head, chest, abdomen, or pelvis based on the primary survey.
Clinical Examination
A thorough secondary survey was performed after initial stabilization.
General:
The patient was alert and oriented, in acute distress due to pain. Vital signs were stable.
Local Examination (Left Lower Extremity):
*
Inspection:
Gross deformity of the left tibia was evident, characterized by apex anterior and valgus angulation in the mid-shaft, accompanied by approximately 2-3 cm of perceived shortening. Significant diffuse swelling was present throughout the lower leg, particularly in the anterior and lateral compartments. The skin over the fracture site was intact, but stretched and shiny, with an area of impending tenting over the medial aspect of the apex of the deformity. No open wounds, abrasions, or ecchymosis were noted acutely.
*
Palpation:
Marked tenderness was elicited directly over the tibial mid-diaphysis. Bony crepitus was palpable with gentle manipulation. The calf musculature felt firm, but not tense initially. Temperature was normal compared to the contralateral limb.
*
Range of Motion (ROM):
Active and passive range of motion of the ipsilateral knee and ankle were severely limited by pain. Attempts at passive dorsiflexion and plantarflexion of the ankle exacerbated pain significantly.
*
Neurological Assessment:
*
Peroneal Nerve:
Motor function intact (5/5) for ankle dorsiflexion and great toe extension. Sensation intact (normal light touch) in the first dorsal web space.
*
Tibial Nerve:
Motor function intact (5/5) for ankle plantarflexion and toe flexion. Sensation intact (normal light touch) on the plantar aspect of the foot.
*
Vascular Assessment:
Distal pulses (dorsalis pedis and posterior tibial) were palpable and strong (2+), symmetrical with the contralateral limb. Capillary refill in the toes was brisk (<2 seconds). Skin temperature and color of the foot were normal. Ankle-Brachial Index (ABI) was not formally performed but was not clinically indicated given strong pulses.
Compartment Syndrome Evaluation: Close monitoring was initiated immediately due to the high-energy mechanism and significant swelling. While compartments were initially firm, direct pressure measurement was not deemed necessary at presentation given the absence of classic "5 Ps" (pain out of proportion, paresthesia, pallor, paralysis, pulselessness) and normal sensation. However, a low threshold for reassessment and potential measurement was maintained.
Imaging & Diagnostics
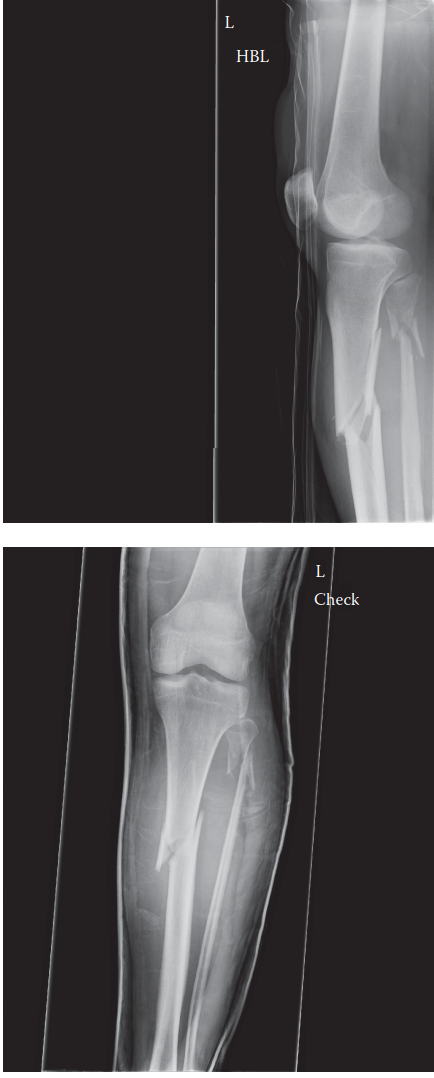
Initial Radiographs:
Standard anteroposterior (AP) and lateral radiographs of the left tibia and fibula were obtained, ensuring inclusion of the knee and ankle joints.

*
Findings:
The radiographs revealed a significantly displaced and comminuted transverse-oblique fracture of the left tibial diaphysis at the junction of the middle and distal thirds (approximately 10 cm proximal to the plafond).
* There was prominent apex anterior angulation (estimated 25-30 degrees) and valgus angulation (estimated 15-20 degrees).
* Significant shortening of approximately 2 cm was observed.
* Rotational deformity was difficult to assess accurately on plain radiographs but suspected clinically.
* The fracture pattern showed a large butterfly fragment on the posterior aspect and significant comminution involving the medial and lateral cortices.
* The fibula was intact.
* Both the knee and ankle joints appeared anatomically congruous with no evidence of intra-articular extension or associated fractures.
Computed Tomography (CT) Scan:
A CT scan of the left tibia was subsequently obtained to further characterize the fracture morphology, particularly regarding rotational deformity and precise comminution, and to exclude occult intra-articular extension given the proximity to the ankle.
*
Findings:
The CT scan confirmed the highly comminuted transverse-oblique fracture with an identifiable large posterior butterfly fragment. It precisely quantified the angulation to be 28 degrees apex anterior and 18 degrees valgus. Crucially, multiplanar reconstructions and 3D imaging demonstrated approximately 20 degrees of external rotation of the distal fragment relative to the proximal tibia. No intra-articular extension was noted. The fibula remained intact.
*
Templating:
Pre-operative templating using contralateral limb radiographs and CT data was performed to estimate appropriate nail length and diameter, confirming the need for a reamed intramedullary nail and considering potential challenges in achieving and maintaining rotational alignment.
Laboratory Studies:
Initial laboratory investigations included a complete blood count (CBC), comprehensive metabolic panel (CMP), coagulation profile, and type and screen. All results were within normal limits, indicating no acute anemia, electrolyte disturbances, or coagulopathy. Inflammatory markers (ESR, CRP) were not indicated acutely.
Differential Diagnosis
The primary diagnosis is an acute, closed, comminuted tibial diaphyseal fracture. However, in the context of acute lower limb trauma with significant pain and deformity, several other conditions must be considered or excluded.
| Feature / Condition | Acute Tibial Diaphyseal Fracture (Primary) | Acute Compartment Syndrome (ACS) | Severe Tibial Contusion / Hematoma | Pathological Fracture (e.g., Fibrous Dysplasia) |
|---|---|---|---|---|
| Mechanism of Injury | High-energy trauma (MVC, fall, direct impact) | Trauma (direct impact, fracture, reperfusion injury, crush) | Direct blunt trauma, falls | Minor trauma or spontaneous, often pre-existing lesion |
| Pain Characteristics | Severe, localized, sharp pain; exacerbated by movement. | Pain "out of proportion" to injury; deep, constant, throbbing; worsens with passive stretch. | Localized pain, aching, improves with rest. | Acute severe pain at fracture site, but may have chronic dull ache prior. |
| Deformity / Swelling | Gross deformity (angulation, shortening, rotation) and significant swelling. | Significant swelling, limb may feel tense and firm to palpation. No intrinsic bony deformity. | Localized swelling, ecchymosis, sometimes palpable hematoma. No bony deformity. | Acute deformity at fracture site; may have subtle pre-existing bowing or enlargement. |
| Skin Integrity | Intact (closed) or open (Gustilo-Anderson). Skin may be tented/blistered. | Intact, stretched, shiny. | Intact, ecchymosis common. | Intact, unless open pathological fracture. |
| Neurovascular Status | Variable: usually intact, but monitor for nerve/vascular compromise. | Early: Paresthesia. Late: Paralysis, Pulselessness. Reduced sensation. | Intact neurovascular function. | Typically intact neurovascular status. |
| Palpation | Focal tenderness, crepitus, abnormal motion. | Tense, firm compartments. Pain with passive stretch of digits. | Focal tenderness, often soft/boggy. | Focal tenderness at fracture site; may feel firm/expanded prior. |
| Radiographic Findings | Displaced fracture lines, comminution, angulation, shortening. | Normal X-rays for compartment syndrome itself, but associated fracture may be present. | Normal X-rays, sometimes soft tissue swelling. | Lytic/blastic lesion, cortical thinning/expansion, "shepherd's crook" deformity (fibrous dysplasia). |
| Definitive Diagnosis | Radiographs, CT. | Clinical signs, confirmed by direct intracompartmental pressure measurement (>30 mmHg or ΔP < 30 mmHg). | Clinical findings. | Biopsy (for underlying lesion), characteristic radiographic features. |
| Management Principle | Reduction and stabilization (operative vs. non-operative). | Emergency fasciotomy. | RICE (Rest, Ice, Compression, Elevation), analgesia. | Surgical stabilization, treatment of underlying pathology. |
Surgical Decision Making & Classification
Given the patient's age, high-energy mechanism of injury, and significant displacement with multi-planar deformity (apex anterior angulation, valgus angulation, and external rotational deformity), operative intervention was indicated as the definitive treatment for this tibial diaphyseal fracture.
Indications for Operative Fixation:
*
Significant displacement and instability:
The degree of angulation, shortening, and rotational deformity exceeded acceptable non-operative parameters for closed tibial shaft fractures (typically <10 degrees angulation in any plane, <10-15 degrees apex anterior/posterior, <1 cm shortening, <10-15 degrees rotation).
*
High-energy mechanism:
Increased risk of soft tissue compromise, progressive deformity, and non-union with non-operative management.
*
Patient factors:
A young, active individual who requires early mobilization and return to function. Non-operative management with prolonged casting would significantly impair his ability to perform his occupation.
*
Impending skin compromise:
The tenting of the skin over the apex of the fracture carried a risk of open fracture development or pressure necrosis, necessitating urgent reduction and stabilization.
Contraindications to Non-Operative Management:
* Inability to achieve or maintain an acceptable reduction.
* Open fractures (though this case was closed).
* Vascular injury requiring repair.
* Associated compartment syndrome.
* Polytrauma where early definitive stabilization is part of damage control orthopedics.
Classification:
*
AO/OTA Classification:
Based on the radiographs and CT, this fracture was classified as
42-C2
.
*
4:
Tibia/Fibula.
*
2:
Diaphyseal.
*
C:
Complex fracture, with a large intermediate fragment (butterfly fragment).
*
2:
Intact fibula (implies relatively more stability in the overall construct compared to a fibular fracture at the same level, but also makes reduction more challenging due to fibular splinting).
*
Gustilo-Anderson Classification:
The fracture remained closed, therefore, it was Gustilo-Anderson Type 0.
Based on these considerations, intramedullary nailing (IMN) was chosen as the treatment of choice due to its biomechanical advantages, load-sharing properties, and high union rates for tibial diaphyseal fractures.
Surgical Technique / Intervention
The patient was taken to the operating theatre on an urgent basis (within 12 hours of injury) after resuscitation and pre-operative workup.
Pre-operative Planning:
Detailed planning included reviewing CT images for fracture pattern, comminution, and rotational profile. Contralateral limb X-rays were used for templating nail length and diameter. The planned approach involved a reamed intramedullary nail with an infrapatellar entry point.
Anesthesia:
General anesthesia was administered, along with a regional nerve block (femoral and sciatic nerve block) for enhanced post-operative pain control.
Patient Positioning:
The patient was positioned supine on a radiolucent operating table. A bump was placed under the ipsilateral hip to ensure the leg was in a neutral position. The knee was flexed approximately 90 degrees using a leg support, allowing access to the infrapatellar region for nail entry. The foot was suspended in a sterile boot or held in manual traction for initial reduction maneuvers. Fluoroscopy was set up to allow for AP and lateral views of the entire tibia, knee, and ankle.
Surgical Approach and Reduction:
1.
Preparation and Draping:
The limb was prepped with chlorhexidine/alcohol solution and draped in a sterile fashion from the thigh to the toes.
2.
Infrapatellar Entry Point:
A 3-4 cm longitudinal incision was made distal to the patella, medial to the patellar tendon. The patellar tendon was retracted laterally, and the infrapatellar fat pad was carefully dissected to expose the entry point on the anterior aspect of the tibia. A starting awl was used to create an entry portal aligned with the anatomical axis of the tibia, typically just lateral to the anterior tibial spine, to prevent iatrogenic malalignment (valgus or apex anterior/posterior).
3.
Initial Reduction:
Achieving reduction was critical due to the significant angulation, shortening, and rotational deformity.
*
Traction:
Initial traction was applied manually or using a fracture table to restore length.
*
Manipulation:
Direct manual manipulation, using the "three-point bending" technique, was applied to correct the apex anterior and valgus angulation under fluoroscopic guidance.
*
Blocking Screws (Poller Screws):
Given the comminution and difficulty in achieving stable reduction, two blocking screws were strategically placed.
* One blocking screw was inserted anteromedially into the proximal fragment, distal to the fracture site, to guide the nail laterally and correct valgus.
* Another blocking screw was inserted posterolaterally into the distal fragment, proximal to the fracture site, to guide the nail anteriorly and correct apex anterior deformity. These screws were placed parallel to the intended nail trajectory, effectively reducing the canal diameter and forcing the nail to align the fragments.
*
Rotational Correction:
Rotational alignment was particularly challenging. Clinical assessment (tibial tubercle aligned with second toe) combined with careful fluoroscopic assessment of the ankle mortise and the relationship of the fibula to the tibia in the distal fragment was paramount. The distal fragment was manually derotated until anatomical alignment was achieved.
4.
Reaming:
Once acceptable reduction (length, alignment, rotation) was achieved and maintained, a guidewire was advanced across the fracture site and into the distal tibial metaphysis, ideally centered in both AP and lateral views. Sequential reaming was performed, gradually increasing reamer size by 0.5 mm increments, until cortical chatter was felt. The decision to ream was based on the fracture pattern (comminuted, which benefits from improved union rates with reaming) and the need for a strong, well-fitting nail.
5.
Nail Insertion:
A reamed intramedullary nail (e.g., solid or cannulated, typically 10-12 mm diameter) of appropriate length was selected and inserted over the guidewire. The nail was advanced carefully across the fracture site, maintaining reduction, and driven until it was flush with or slightly recessed below the articular surface of the knee.
6.
Proximal Locking:
Under fluoroscopic guidance, two proximal locking screws were inserted in a static fashion to prevent shortening and control rotation in the proximal fragment.
7.
Distal Locking:
Crucially, the final rotational alignment was re-assessed after proximal locking. The C-arm was rotated to obtain perfect circles of the distal locking holes in both AP and lateral planes. Two distal locking screws were inserted to provide static locking, ensuring rotational and translational stability of the distal fragment.
8.
Wound Closure:
The incisions were irrigated thoroughly. The patellar tendon and subcutaneous tissues were closed in layers, and the skin was closed with staples. A sterile dressing was applied.
Post-Operative Protocol & Rehabilitation
Immediate Post-Operative Period (Days 0-7):
*
Pain Management:
Multimodal analgesia including regional nerve block, oral opioids, NSAIDs, and acetaminophen.
*
Neurovascular Checks:
Frequent neurovascular assessments (q4h for 24-48h, then q8h) to monitor for potential compartment syndrome or iatrogenic nerve injury.
*
Wound Care:
Daily wound checks for signs of infection or skin breakdown. Staples were typically removed at 2 weeks.
*
Deep Vein Thrombosis (DVT) Prophylaxis:
Pharmacological prophylaxis (e.g., low molecular weight heparin) was initiated.
*
Weight Bearing:
Touch-down weight-bearing (TDWB) of 10-20 lbs was initiated immediately with crutches or a walker. The IMN provides stable fixation, allowing for early controlled loading to promote bone healing.
*
Rehabilitation:
*
Ankle ROM:
Active and passive range of motion exercises for the ankle and foot were started on post-operative day 1 to prevent stiffness.
*
Knee ROM:
Gentle active and passive knee flexion and extension exercises were initiated, working towards full extension and 90 degrees of flexion within the first week to prevent patellar adhesions.
*
Isometric Exercises:
Quadriceps and gluteal isometric exercises.
Early Rehabilitation (Weeks 2-6):
*
Weight Bearing:
Progressive weight-bearing (PWB) was encouraged as pain allowed and with radiographic evidence of early callus formation. This progressed to partial weight-bearing (PWB) of 25-50% body weight.
*
Strengthening:
Introduction of light resistance exercises for quadriceps, hamstrings, and calf muscles.
*
Gait Training:
Focus on normalized gait pattern with assistive devices.
*
Continued ROM:
Maintaining and improving knee and ankle range of motion.
Intermediate Rehabilitation (Weeks 6-12):
*
Weight Bearing:
Full weight-bearing (FWB) was initiated once clinical and radiographic signs of bridging callus were evident.
*
Advanced Strengthening:
Increased resistance exercises, proprioception training, and balance activities.
*
Functional Training:
Stair climbing, uneven terrain walking.
Late Rehabilitation and Return to Activity (Months 3+):
*
Radiographic Follow-up:
Regular X-rays (monthly initially, then bimonthly) to monitor fracture healing. Union was typically expected by 4-6 months, but could extend to 9 months or more for comminuted fractures.
*
Activity Progression:
Gradual return to work, recreational activities, and eventually sport-specific training, guided by clinical stability, pain levels, and radiographic union. High-impact activities were generally deferred until complete union.
*
Hardware Removal:
Elective hardware removal (e.g., locking screws or the nail itself) was considered typically after 12-18 months for symptomatic hardware, implant prominence, or for young, active patients desiring return to high-impact sports, provided the fracture was fully united.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls:
- Thorough Neurovascular Assessment: Always perform and meticulously document pre-operative and serial post-operative neurovascular examinations. Missed compartment syndrome is a catastrophic pitfall.
- Correct Entry Point for IMN: For infrapatellar approach, the entry point should be slightly medial to the lateral edge of the patellar tendon, directing the awl towards the intercondylar notch in line with the anatomical axis of the tibia. This avoids iatrogenic valgus or procurvatum deformity. Suprapatellar nailing is an excellent alternative, offering better alignment control, especially in proximal fractures, or when the knee cannot be significantly flexed.
- Anatomical Reduction First: Strive for the best possible reduction (length, alignment, rotation) before nail insertion. The nail primarily provides stability, not reduction.
- Blocking Screws (Poller Screws): In comminuted fractures or those with inherent deformity, strategically placed blocking screws are invaluable for guiding the nail and achieving/maintaining optimal alignment, especially for preventing apex anterior/posterior and varus/valgus deformities.
-
Rotational Control:
Rotational alignment is the most common cause of malunion in tibial nailing. Utilize multiple techniques:
- Clinical assessment: Compare foot position to patella/tibial tubercle.
- Fluoroscopic assessment: "Perfect circles" of distal locking holes; assess fibular overlap to tibia at the ankle; compare cortical step-off in AP/lateral views.
- Contralateral limb comparison (clinical and radiographic).
- Reaming Benefits: Reamed nailing generally leads to higher union rates in comminuted diaphyseal fractures due to increased cortical contact and introduction of osteoprogenitor cells.
- Prophylactic Fibular Osteotomy: Consider a prophylactic fibular osteotomy in cases of severely displaced or shortened fractures with an intact fibula, as the fibula can act as a "splint," preventing full length restoration or fracture reduction.
- Early Joint Motion: Encourage early range of motion of the knee and ankle to prevent stiffness, which is a common post-operative complication.
- Open Fracture Management: For open fractures (not in this case but relevant for context), immediate debridement, copious irrigation, broad-spectrum antibiotics, and appropriate wound management (e.g., delayed primary closure, V.A.C., local flaps) are paramount.
Pitfalls:
- Missed Compartment Syndrome: A life- and limb-threatening emergency. High index of suspicion with high-energy trauma, especially in tibia fractures. Monitor for "pain out of proportion," pain on passive stretch, paresthesia.
-
Malunion:
- Rotational Malunion: Most frequent and poorly tolerated malunion. Difficult to identify clinically intraoperatively and can lead to significant functional impairment and secondary arthrosis.
- Angulatory Malunion: Often due to improper entry point or inadequate reduction before nailing (e.g., iatrogenic valgus/procurvatum with a medial/anterior entry point).
- Shortening: Can occur if adequate length is not restored and maintained during nailing, or if insufficient locking leads to settling.
- Non-union: Failure of fracture healing, often due to inadequate stability, infection, poor biology (e.g., smoking, comorbidities), or significant bone loss. May necessitate revision surgery (e.g., exchange nailing, bone grafting, plating).
- Infection: Risk, particularly in open fractures or prolonged operative times. Can lead to osteomyelitis and delayed union/non-union.
- Iatrogenic Nerve Injury: Most commonly the saphenous nerve (medial incision, knee pain), superficial peroneal nerve (lateral distal locking), or common peroneal nerve (excessive traction).
- Knee Pain: Common complication after tibial nailing, particularly with infrapatellar entry, due to patellar tendon irritation, fat pad impingement, or prominent hardware. Suprapatellar approach may mitigate this.
- Hardware Prominence/Pain: Common at the proximal or distal locking screws, often requiring eventual removal.
- Synostosis: Iatrogenic tibio-fibular synostosis, especially after trauma or with extensive periosteal stripping, can restrict ankle motion.
- Failure to Recognize Associated Injuries: Especially critical in polytrauma (e.g., floating knee, calcaneal fractures, spine injuries).
