Introduction & Epidemiology
Proximal tibial diaphyseal fractures represent a significant subset of lower extremity trauma, characterized by their proximity to the knee joint and the unique biomechanical challenges they present during surgical fixation. These fractures commonly occur as a result of high-energy mechanisms, such as motor vehicle collisions or falls from height, but can also result from lower-energy rotational forces. While they are extra-articular, their location within the metaphyseal-diaphyseal junction often leads to characteristic deforming forces that complicate reduction and stabilization, particularly with intramedullary (IM) nailing. The epidemiology reflects a bimodal distribution, affecting young, active individuals involved in high-energy trauma and older osteopenic patients susceptible to falls. Associated injuries, including compartment syndrome, vascular damage, and ligamentous knee injuries, are not uncommon and necessitate thorough evaluation.
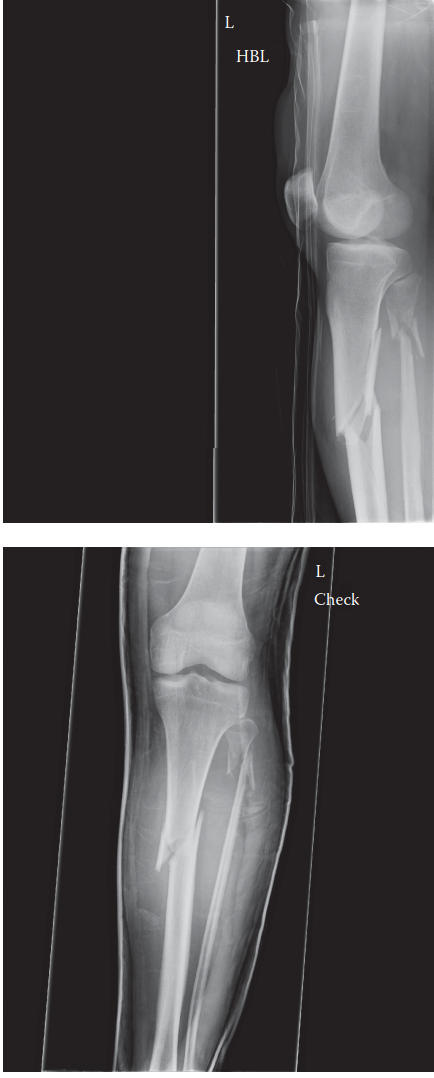
Intramedullary nailing has become the gold standard for the treatment of most tibial diaphyseal fractures due offering distinct advantages over plate fixation, including load-sharing properties, reduced soft tissue stripping, and lower rates of infection and nonunion. However, the unique anatomy of the proximal tibia, specifically its wider medullary canal and the powerful muscular attachments, makes achieving and maintaining anatomical alignment challenging. Deformities such as valgus and procurvatum (apex anterior) are frequently encountered, demanding meticulous surgical technique and often the use of adjunctive reduction tools to ensure optimal outcomes. The radiographs below illustrate a typical presentation of such a fracture:

These are AP and lateral radiographs of the left tibia and fibula showing a proximal tibial diaphyseal fracture. The fracture exhibits significant valgus and procurvatum (apex anterior) deformities. Addressing these specific malalignments is paramount to prevent adverse biomechanical consequences on the knee and ankle joints, which can lead to early degenerative changes, persistent pain, and functional limitations.
Surgical Anatomy & Biomechanics
Successful management of proximal tibial diaphyseal fractures necessitates a comprehensive understanding of the regional surgical anatomy and the biomechanical principles governing fracture displacement and stabilization.
Anatomy of the Proximal Tibia
The proximal tibia transitions from a broad metaphysis, which supports the knee joint, to a narrower diaphyseal shaft.
*
Cortical Bone:
The cortex is thinnest anteriorly and medially in the proximal metaphysis, increasing in thickness distally along the diaphysis. This regional variation influences nail fit and stability.
*
Medullary Canal:
The proximal tibia has a characteristic funnel shape, with a wide, often triangular or oval canal proximally that gradually constricts to a narrower, more circular diameter in the mid-diaphysis. This widening proximally significantly reduces the cortical contact points for an IM nail, making primary stability challenging and increasing the risk of sagittal and coronal plane malalignment.
*
Soft Tissue Envelope:
The proximal tibia is enveloped by critical soft tissue structures.
*
Anterior Compartment:
Contains the tibialis anterior, extensor hallucis longus, extensor digitorum longus, and peroneus tertius muscles, along with the deep peroneal nerve and anterior tibial artery/veins. The bulk of these muscles on the lateral aspect of the tibia contributes to deforming forces.
*
Medial Aspect:
The pes anserinus (sartorius, gracilis, semitendinosus) inserts on the medial aspect of the tibia, approximately 5 cm distal to the joint line. This strong tendinous complex is a primary contributor to valgus deformity.
*
Lateral Aspect:
The fibular head is an important landmark for the common peroneal nerve, which wraps around its neck. The lateral compartment muscles (peroneus longus and brevis) are located more distally and do not exert significant deforming forces on the proximal fragment.
*
Posterior Compartment:
Divided into superficial (gastrocnemius, soleus, plantaris) and deep (tibialis posterior, flexor digitorum longus, flexor hallucis longus) compartments. The soleus bridge effect can sometimes stabilize proximal oblique fractures.
*
Neurovascular Structures:
*
Popliteal Artery:
Bifurcates into the anterior tibial artery and tibioperoneal trunk just distal to the knee. The anterior tibial artery passes through the interosseous membrane to enter the anterior compartment.
*
Common Peroneal Nerve:
Courses around the fibular neck, making it vulnerable to injury from trauma, surgical approaches, or external fixator pins.
Deforming Forces in Proximal Tibial Diaphyseal Fractures
The characteristic deformities observed in proximal tibial diaphyseal fractures are a direct consequence of unopposed muscle pulls and the unique morphology of the proximal segment.
-
Procurvatum (Apex Anterior) Deformity:
- The primary cause is the powerful, unopposed pull of the patellar tendon (quadriceps mechanism) on the proximal fragment. This force tends to pull the proximal fragment anteriorly and proximally.
- Conversely, the distal fragment, lacking direct muscular support at the fracture site, tends to sag posteriorly due to gravity and the pull of the gastrocnemius-soleus complex, which plantarflexes the foot. This relative posterior displacement of the distal fragment creates an apex anterior angulation.
-
Valgus Deformity:
- The strong, unopposed pull of the pes anserinus (composed of the sartorius, gracilis, and semitendinosus muscles) on the medial aspect of the proximal fragment exerts a powerful adduction force.
- Simultaneously, the bulky anterior compartment musculature (tibialis anterior, extensor digitorum longus, extensor hallucis longus) on the lateral aspect of the tibia acts as a buttress, preventing medial displacement and actively contributing to the valgus angulation by pulling the proximal fragment laterally relative to the distal segment. There are no strong, opposing muscle groups attached laterally on the proximal fragment to counteract this medial pull.
-
Rotation: Rotational deformity is variable and less predictable. It can be influenced by the fracture pattern (e.g., spiral components), integrity of the interosseous membrane, and the presence of an associated fibular fracture. The external rotators of the hip and the pull of the ankle musculature can contribute.
Biomechanics of Intramedullary Nailing
Intramedullary nailing functions as a load-sharing device, providing stability through its fit within the medullary canal and locking screws. In the proximal tibia, several biomechanical challenges arise:
*
Metaphyseal Widening:
The wide, funnel-shaped proximal canal provides limited nail-cortical contact. This lack of endosteal support allows for "windshield-wiper" motion of the nail within the proximal fragment, increasing the risk of angulatory malalignment (especially valgus and procurvatum) despite locking screws.
*
Deforming Forces:
The powerful muscle pulls described above can overcome the inherent stability of the nail, particularly if the initial reduction is not anatomical or if the nail is undersized.
*
Entry Point:
The optimal entry point for tibial IM nailing is critical. A slightly medial entry point through the patellar tendon is generally preferred. An entry point that is too lateral can exacerbate or create a valgus deformity, as the nail will be forced against the lateral cortex of the proximal fragment. Similarly, an entry point that is too anterior can contribute to procurvatum.
*
Locking Screws:
While proximal locking screws provide rotational and length stability, they primarily prevent displacement of the proximal fragment relative to the nail. They do not intrinsically correct angulatory malalignment if the nail itself is not perfectly aligned with the proximal fragment's mechanical axis. This limitation underscores the importance of achieving an anatomical reduction
before
nail insertion and locking.
The sum of these anatomical and biomechanical factors necessitates specific reduction maneuvers and adjunctive techniques during intramedullary nailing of proximal tibial diaphyseal fractures to counteract the powerful deforming forces and ensure optimal alignment.
Indications & Contraindications
The decision-making process for the management of proximal tibial diaphyseal fractures involves a careful consideration of fracture characteristics, patient factors, and soft tissue status. Intramedullary nailing is the preferred method for the majority of these fractures, but specific indications and contraindications exist.
Indications for Operative Management (Intramedullary Nailing)
-
Displaced and Unstable Fractures:
- Angulation greater than 5-10 degrees in any plane (valgus/varus, procurvatum/recurvatum).
- Translation greater than 50% of the bone diameter.
- Shortening greater than 1 cm.
- Rotational deformity >10-15 degrees.
- Comminuted or segmental fractures where inherent stability is compromised.
-
Open Fractures:
- Gustilo-Anderson Type I, II, IIIA fractures, following appropriate emergent debridement and irrigation. IM nailing can proceed once the wound is clean and manageable.
-
Polytrauma Patients:
- Early definitive stabilization (within 24 hours of injury) of long bone fractures in hemodynamically stable polytrauma patients is part of damage control orthopedics, reducing the risk of systemic complications such as ARDS or fat embolism syndrome.
-
Floating Knee Injuries:
- Simultaneous ipsilateral femur and tibia fractures often require IM nailing of both bones for stability and functional recovery.
-
Pathological Fractures:
- Fractures occurring through compromised bone (e.g., tumor, metabolic bone disease) require stabilization to prevent further collapse and facilitate patient mobility.
-
Impending Compartment Syndrome:
- While not a primary indication for nailing, early fracture stabilization can sometimes alleviate soft tissue tension, but fasciotomy is often indicated.
-
Failed Non-Operative Management:
- Progressive displacement, delayed union, or nonunion in fractures initially managed conservatively.
Contraindications for Operative Management
-
Active Infection:
- Absolute contraindication for elective IM nailing. For open fractures, infection risk is managed with serial debridement and antibiotics, sometimes requiring initial external fixation before IM nailing.
-
Severe Soft Tissue Compromise:
- Extensive open wounds (Gustilo-Anderson Type IIIB or IIIC) with significant tissue loss, devitalized tissue, or inadequate coverage. These often require initial external fixation, serial debridement, and soft tissue reconstruction before definitive internal fixation is considered.
- Severe burns, crush injuries, or severe vascular compromise where limb salvage is questionable.
-
Severe Medical Comorbidities:
- Patients deemed medically unfit for general anesthesia or prolonged surgery.
-
Extremity at Risk for Amputation:
- In cases of severe vascular injury, irreparable nerve damage, or extensive tissue loss, primary amputation may be a more appropriate course of action.
-
Minimally Displaced, Stable Fractures:
- Rare in the proximal tibia, but exceptionally stable fractures with minimal displacement and no significant deforming forces may be considered for non-operative management in select patients. However, the risk of secondary displacement and malunion with non-operative treatment in this region is high.
Operative vs. Non-Operative Indications
The following table summarizes the general considerations for operative versus non-operative management of tibial diaphyseal fractures, with specific relevance to the challenges of proximal fractures.
| Indication Type | Operative Management (Intramedullary Nailing) | Non-Operative Management |
|---|---|---|
| Fracture Displacement | >5-10° angulation (valgus, procurvatum), >50% translation, >1 cm shortening | Minimally displaced, stable fracture, no significant angulation or shortening |
| Fracture Type | Unstable, comminuted, segmental, spiral, oblique, high-energy | Non-displaced transverse or short oblique, low-energy, stable |
| Open Fractures | Gustilo Type I, II, IIIA (after debridement) | Gustilo Type IIIB/IIIC (often external fixation initially, then definitive) |
| Associated Injuries | Polytrauma, floating knee, impending compartment syndrome | Isolated injury, stable soft tissues, no neurovascular compromise |
| Patient Factors | Medically fit, compliant with rehabilitation, active lifestyle | Significant medical comorbidities, non-ambulatory, poor prognosis |
| Soft Tissue Status | Adequate soft tissue envelope, manageable wound | Uncompromised soft tissues, no significant swelling or blistering |
| Failed Non-Op | Progressive displacement, delayed union, nonunion | Initial stable reduction maintained, uneventful healing |
It is important to note that non-operative treatment for proximal tibial diaphyseal fractures is rarely recommended due to the high risk of malunion, particularly procurvatum and valgus deformities, given the strong deforming muscle forces in this region. The wide metaphyseal canal also makes cast stability difficult to achieve.
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning and precise patient positioning are critical steps to optimize surgical outcomes and mitigate complications in IM nailing of proximal tibial fractures.
Pre-Operative Planning
-
Imaging Review:
- AP and Lateral Radiographs: Essential for initial assessment of fracture pattern, displacement, and angulation. Full-length views of the tibia, including the knee and ankle joints, are crucial to identify any pre-existing deformities and to plan for nail length.
- Contralateral Limb Radiographs: Obtaining AP and lateral radiographs of the uninjured contralateral tibia can be invaluable for templating the ideal nail length and diameter, especially for fractures with significant comminution or shortening.
- Computed Tomography (CT) Scan: Recommended for complex fracture patterns, suspected articular involvement (even in supposedly extra-articular fractures), or when rotational or sagittal plane deformities are difficult to ascertain from plain radiographs. CT provides a detailed understanding of fragment morphology and can guide reduction strategies.
-
Nail Selection:
- Diameter: The largest possible nail diameter that comfortably fits the narrowest part of the medullary canal (typically mid-diaphysis) should be chosen to maximize rigidity and stability. This is usually determined by templating and confirmed intra-operatively with reaming. Typically, diameters range from 8 mm to 11 mm.
- Length: Nail length is determined by measuring the contralateral tibia or estimating from the patient's height. The nail should ideally span from the entry portal to just proximal to the physis or within 1-2 cm of the ankle joint line, ensuring adequate distal locking.
- Proximal Locking Options: Modern tibial nails offer multiple proximal locking options (e.g., multi-planar screws, oblique screws) to enhance stability in the wide proximal metaphysis and resist deforming forces. The surgeon must be familiar with the chosen implant system.
- Nail Type: Standard infrapatellar nails are most common. However, for very proximal fractures, suprapatellar nails or even specialized "proximal tibia nails" with specific angulations or locking configurations may be considered to optimize entry point and fragment control.
-
Patient Optimization:
- Assess and optimize patient comorbidities.
- Administer appropriate prophylactic antibiotics (e.g., Cefazolin) prior to incision.
- Consider regional nerve blocks (e.g., popliteal block) for enhanced post-operative pain control.
- Anticipate potential need for blood transfusion in high-energy injuries.
-
Equipment Preparation:
- Ensure availability of all necessary IM nailing instruments, reamers, guidewires, locking screws, and targeting devices.
- Have adjunctive reduction tools readily available: large pointed reduction clamps, bone hooks, percutaneous reduction tools, external fixator pins (Schanz screws) for joystick maneuvers or "Poller" blocking screws, and potentially a femoral distractor or external fixator for provisional reduction.
Patient Positioning
The most common and effective patient position for tibial IM nailing, especially for proximal fractures, is supine with the knee flexed to 90 degrees.
1.
Supine Position:
The patient lies supine on a radiolucent operating table.
2.
Knee Flexion:
The knee is acutely flexed to 90 degrees or more. This position allows for:
*
Optimal Entry Portal Access:
It relaxes the quadriceps mechanism and displaces the patella superiorly, providing clear access to the infrapatellar entry portal.
*
Proximal Fragment Control:
Placing a bump or bolster under the distal thigh allows the proximal fragment to rest in a more neutral alignment, helping to counteract the procurvatum deformity.
*
Fluoroscopic Visualization:
Facilitates obtaining true AP and lateral views of the proximal tibia without undue soft tissue interference.
3.
Foot Positioning:
* The foot is often placed in a specialized traction boot or held by a sterile-gloved assistant. This allows for controlled longitudinal traction to achieve length restoration and aids in rotational alignment.
* The foot should be positioned to allow full C-arm access for both AP and lateral views of the ankle for distal locking.
4.
C-arm Fluoroscopy Access:
* The C-arm must have unrestricted access to visualize the entire tibia, from the knee to the ankle, in both AP and lateral projections.
* For proximal tibial fractures, it is crucial to ensure a true lateral view of the proximal tibia/knee. This often requires angling the C-arm or rotating the patient's hip slightly, rather than relying on tilting the foot, which can introduce artifactual rotation.
* It's imperative to confirm orthogonal views (true AP and lateral) throughout the procedure, especially during reduction and locking.
5.
Tourniquet:
A thigh tourniquet is routinely applied to minimize blood loss and improve visualization, although it is not always inflated for the entire procedure, especially if there are concerns about limb ischemia or prolonged surgery.
6.
Alternative Positioning (Semi-Extended or Suprapatellar Approach):
* For extremely proximal fractures, those with significant knee stiffness precluding 90-degree flexion, or for specific surgeon preference, a semi-extended or suprapatellar nailing approach can be utilized.
* In this approach, the knee is flexed approximately 15-20 degrees. The entry portal is made through the quadriceps tendon superior to the patella. This offers a more "in-line" reaming trajectory, potentially simplifying reduction of procurvatum and providing a more anatomically aligned entry point for very high fractures. However, it requires specific instrumentation and careful attention to avoid iatrogenic patellofemoral cartilage damage.
Regardless of the chosen positioning, the primary goals are stable, anatomical reduction, unimpeded access to the entry portal, and excellent fluoroscopic visualization of the entire bone.
Detailed Surgical Approach / Technique
The surgical technique for intramedullary nailing of proximal tibial diaphyseal fractures demands precision, particularly in addressing the inherent deforming forces. The goal is an anatomical reduction prior to definitive fixation.
Incisions and Entry Portal
-
Standard Infrapatellar Approach (preferred for most diaphyseal fractures):
- Incision: A longitudinal skin incision of approximately 3-5 cm is made, extending distally from the inferior pole of the patella, slightly medial to the midline. This allows for direct access to the patellar tendon.
- Entry: The patellar tendon is identified. A longitudinal split in the patellar tendon is created, or a small medial paratendinous incision can be made, preserving the central fibers. The fat pad is retracted, and the entry portal is created in the intercondylar notch, aiming for the true axis of the medullary canal.
- Optimal Entry Point: Crucially, the entry point must be in line with the medullary canal of the proximal fragment in both AP and lateral planes. For the proximal tibia, this often means aiming slightly more anterior and medial than one might initially perceive to counteract the procurvatum and valgus tendencies. A common error is an entry point that is too lateral, which can induce or exacerbate a valgus deformity, as the nail will buttress against the lateral wall of the proximal fragment.
-
Suprapatellar Approach (gaining popularity for proximal fractures):
- Incision: A longitudinal incision (2-3 cm) is made superior to the patella, through the quadriceps tendon.
- Entry: A specialized cannula and trocar are used to enter the intercondylar notch while the knee is in slight flexion (15-20 degrees).
- Advantages: This approach offers a more direct, in-line trajectory for the guidewire and nail, potentially making reduction of procurvatum easier and minimizing the "push-back" force on the patella. It may also reduce anterior knee pain compared to infrapatellar approaches.
- Disadvantages: Requires specialized instrumentation, potential for patellofemoral cartilage damage (though clinical significance debated), and careful technique to avoid quadriceps tendon disruption.
Reduction Techniques for Proximal Deformities
Achieving and maintaining reduction is the most challenging aspect of proximal tibial nailing. The powerful deforming forces of the patellar tendon (procurvatum) and pes anserinus/anterior compartment muscles (valgus) must be actively counteracted.
-
Manual Traction and Manipulation:
- Longitudinal traction is applied to restore length.
- Direct pressure with hands on the fracture fragments can help align them.
- For procurvatum, a bump under the distal thigh helps extend the knee, relaxing the patellar tendon and allowing the proximal fragment to fall back. Pressure on the anterior aspect of the proximal fragment can also help.
- For valgus, direct medial pressure on the proximal fragment may be required, or laterally directed pressure on the distal fragment.
-
Pointing the Entry Reamer/Awl:
- Once the guidewire is placed, the initial reamer or awl can be used as a joystick to manipulate the proximal fragment into a better position before passing it across the fracture site.
-
Percutaneous Reduction Tools:
- Pointed Reduction Clamps: Large pointed reduction clamps can be applied percutaneously or through small incisions to grasp and manipulate fragments, particularly to correct angulation or rotation.
- Bone Hooks: A bone hook inserted percutaneously can be used to pull or push fragments.
- Schanz Screws (Joystick Technique): A Schanz screw can be inserted into the proximal fragment (away from the intended nail path and locking screw trajectory) and used as a handle to control its position. A second Schanz screw can be placed in the distal fragment to independently manipulate it. These are particularly useful for rotational control and translating fragments.
- External Fixator for Provisional Reduction: In very unstable or comminuted fractures, a temporary external fixator can be applied to restore length and alignment before conversion to an IM nail. This provides stable reduction during reaming and nailing.
-
Blocking Screws (Poller Screws):
- This technique is highly effective for controlling sagittal (procurvatum) and coronal (valgus) plane deformities in the wide metaphyseal regions of the tibia.
- Mechanism: Blocking screws (often referred to as Poller screws, after Poller and others who first described their use) are bicortical screws inserted before reaming and nail insertion. They are placed strategically to narrow the medullary canal in a specific plane, thereby blocking the nail from migrating into an undesired position and channeling it along the desired anatomical axis. They act as an internal "fulcrum" or "bumper" for the nail.
-
Placement for Valgus Deformity:
- To correct valgus (where the proximal fragment is angled laterally and the nail tends to exit laterally), a blocking screw is placed medially in the proximal fragment. This screw prevents the nail from migrating into the medial cortex and forces it to displace laterally, thus closing the valgus angulation.
-
Placement for Procurvatum Deformity:
- To correct procurvatum (where the proximal fragment is angled anteriorly and the nail tends to exit anteriorly), a blocking screw is placed anteriorly in the proximal fragment. This screw prevents the nail from migrating anteriorly and forces it posteriorly, thus correcting the apex anterior angulation.
-
Technical Considerations:
- Timing: Poller screws must be inserted before reaming and nail insertion.
- Location: Placed unicortically or bicortically, just distal to the entry portal, but proximal to the fracture site and not in the path of the proximal locking screws. They should be close to the anticipated path of the nail without directly obstructing the guidewire or initial reamers.
- Screw Size: Large-diameter cortical screws (e.g., 3.5 mm or 4.5 mm) or thick K-wires/Steinmann pins (e.g., 3/16 inch smooth pins) are effective.
- Fluoroscopic Guidance: Essential for precise placement to ensure they are off-axis to the guidewire but within the reaming envelope and do not interfere with subsequent locking.
- Effectiveness: Poller screws create a "three-point bending" effect with the nail, effectively reducing malalignment.
-
This illustration demonstrates the strategic placement of Poller screws to guide the nail path and correct alignment. For valgus correction, a screw would be placed medially in the proximal fragment. For procurvatum, a screw would be placed anteriorly.
- Pitfalls: Incorrect placement can impede nail insertion, create new deformities, or weaken the bone unnecessarily.
Reaming
- Guidewire Placement: Once reduction is achieved, a guidewire is carefully advanced across the fracture site and down the medullary canal into the distal metaphysis. Ensure it is centrally located in both AP and lateral views.
- Progressive Reaming: The medullary canal is progressively reamed with increasing sizes, typically in 0.5 mm increments. Reaming should continue until cortical chatter is felt, indicating cortical contact, and then generally 1.0 to 1.5 mm larger than the intended nail diameter to allow for easier nail insertion and reduce the risk of jamming or thermal necrosis. Reaming helps to consolidate the fracture, promoting healing, and clears the canal for the nail.
Nail Insertion and Locking
-
Nail Insertion:
- The chosen intramedullary nail is then carefully advanced over the guidewire, through the entry portal, and across the fracture site.
- Continuous fluoroscopic monitoring is essential to ensure maintenance of reduction during nail insertion, as the nail itself can push fragments and cause displacement, particularly in the proximal tibia.
- Ensure the nail is fully seated and its proximal end is flush with or slightly below the entry portal to prevent hardware prominence and anterior knee pain.
-
Distal Locking:
- Distal locking screws are inserted using either a targeting guide or a freehand technique under fluoroscopic guidance.
- Typically, two interlocking screws are inserted in different planes to provide rotational stability and prevent shortening. Evaluate for length stability, especially in comminuted fractures.
-
Proximal Locking:
- Proximal locking screws are inserted using the provided targeting guide.
- Given the wide proximal canal, usually 2-3 screws in varying planes (e.g., AP and ML) are used to maximize stability and prevent toggling of the proximal fragment around the nail. These screws engage the nail and the bone cortex, providing rotational and angular stability to the proximal segment.
- Care must be taken to ensure screws are bicortical and do not interfere with prior blocking screws if used.
-
Final Checks:
- Confirm final alignment (length, rotation, angulation) with AP and lateral fluoroscopic views of the entire tibia, knee, and ankle.
- Check for stability.
- Perform a thorough neurovascular examination.
Wound Closure
- The incision(s) are closed in layers, paying meticulous attention to soft tissue viability. The patellar tendon split (if used) is often repaired, followed by subcutaneous tissue and skin closure.
- A sterile dressing is applied.
By combining meticulous surgical planning with appropriate reduction techniques, including the judicious use of blocking screws, the challenges of valgus and procurvatum deformities in proximal tibial diaphyseal fractures can be effectively managed, leading to improved functional outcomes.
Complications & Management
Despite advancements in surgical techniques and implant design, intramedullary nailing of proximal tibial diaphyseal fractures is associated with a spectrum of potential complications. Understanding their incidence and developing robust management strategies is crucial for academic orthopedic surgeons.
Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence | Salvage Strategies |
|---|---|---|
| Malunion | 10-30% (valgus, procurvatum, rotation) | Minor (<5-10°): Acceptable if asymptomatic and functional. Symptomatic: Corrective osteotomy (opening or closing wedge, dome), revision IMN (rare), plate fixation with acute correction. Pre-operative planning with CT/deformity analysis is essential. |
| Nonunion | 5-15% | Hypertrophic: Exchange nailing (larger diameter, dynamization), bone grafting (autograft/allograft), plate fixation. Atrophic: Debridement of fibrous tissue, bone grafting (autograft is gold standard), plate fixation, vascularized fibula graft for large defects. Adjuvant biologicals (e.g., PRP, BMPs) may be considered. |
| Infection | 1-5% (higher in open fractures, Gustilo III) | Superficial: Oral antibiotics, local wound care. Deep (acute): Surgical irrigation & debridement (I&D), IV antibiotics for 4-6 weeks, implant retention if stable. Deep (chronic): Staged protocol: 1. Explantation of hardware, radical debridement, antibiotic cement spacer/beads, external fixation. 2. IV antibiotics. 3. Delayed reimplantation of new IMN/plate once infection cleared. Possible arthrodesis or amputation for intractable cases. |
| Compartment Syndrome | 2-9% | Immediate and complete fasciotomy (all four compartments of the lower leg). Leave wounds open and perform delayed primary closure or skin grafting once swelling subsides. Monitor for acute kidney injury. |
| Hardware Irritation/Pain | 10-20% (prominent nail, screws) | NSAIDs, physical therapy. Persistent: Hardware removal after radiographic evidence of union (nails typically 12-18 months post-op, locking screws 6-12 months post-op). Careful consideration of weight-bearing restrictions post-removal. |
| Periprosthetic Fracture | Rare (during surgery or after) | Intra-operative: If stable, continue with nailing. If unstable, use longer nail, cerclage wires, or plate augmentation. Post-operative: Treat as a new fracture, usually requiring revision fixation (longer nail, plate, revision IMN). |
| Anterior Knee Pain (AKP) | 20-50% | NSAIDs, physical therapy, activity modification. Persistent/Severe: Proximal hardware removal (nail or prominent locking screws) after fracture union. Counseling on potential for residual pain even after removal. Etiology can be multifactorial (entry portal, patellar tendon scarring, nail prominence). |
| Vascular Injury | <1% (anterior tibial artery) | Immediate surgical exploration. Vascular repair (direct repair, interposition graft, bypass). Often requires concomitant fasciotomy. Pre-operative angiography if high suspicion. |
| Nerve Injury | <1% (common peroneal nerve) | Common peroneal nerve: Observation for neurapraxia. If transected, microsurgical repair/grafting. Deep peroneal nerve: Typically transient. Monitor for recovery. |
| Fat Embolism Syndrome | Rare (0.5-2%, higher in polytrauma) | Supportive care: ventilatory support, hemodynamic stabilization. Prevention: Early fracture stabilization, careful reaming. |
Specific Discussion of Key Complications
Malunion
Malunion is the most frequently encountered complication, particularly for proximal tibial fractures. The unique deforming forces contribute to a high incidence of
procurvatum
(apex anterior angulation) and
valgus
deformities. Rotational malunion is also common but often clinically subtle unless severe.
*
Aetiology:
Inadequate initial reduction, failure to maintain reduction during reaming/nail insertion, incorrect entry portal, or insufficient stability of the IM nail in the wide proximal canal.
*
Clinical Significance:
Symptomatic malunion can lead to knee pain, altered gait mechanics, patellofemoral arthrosis, premature degenerative changes in the knee or ankle, and functional limitations. Even minor deformities can be poorly tolerated.
*
Management:
* Asymptomatic or functionally acceptable minor malunions are observed.
* Symptomatic malunions often require corrective osteotomy. This involves careful pre-operative planning using full-length standing radiographs and CT scans to precisely determine the magnitude and location of the deformity. Corrective osteotomies can be performed as opening-wedge, closing-wedge, or dome osteotomies, stabilized with plates or, rarely, revision IM nails.
Nonunion
Nonunion refers to the failure of a fracture to heal after an appropriate period (typically 6-9 months) or without signs of progression towards healing.
*
Aetiology:
Inadequate stability, poor blood supply, infection, significant soft tissue damage, comminution, or patient factors (e.g., smoking, diabetes).
*
Types:
*
Hypertrophic:
Characterized by abundant callus formation but no bony bridge, indicating sufficient biology but inadequate stability. Managed with exchange nailing (larger diameter nail, dynamization) or plate fixation.
*
Atrophic:
Characterized by minimal or no callus, indicating both poor biology and instability. Requires debridement of fibrous tissue at the fracture site, bone grafting (autograft being the gold standard), and stable fixation (often plate fixation, or exchange nailing with grafting).
*
Management:
Infection must always be ruled out in cases of nonunion.
Anterior Knee Pain (AKP)
AKP is a very common complaint after tibial IM nailing, with reported incidences ranging from 20% to 50%.
*
Aetiology:
Multifactorial, including damage to the infrapatellar fat pad, scarring of the patellar tendon, neuroma formation, prominence of the nail or locking screws, and patellofemoral cartilage damage (especially with infrapatellar approach).
*
Management:
Initially conservative with NSAIDs, physical therapy, and activity modification. If pain is severe and persistent after fracture union, removal of the nail and/or prominent proximal locking screws may provide relief. Patients should be counseled that not all anterior knee pain resolves after hardware removal.
Compartment Syndrome
Proximal tibial fractures are among the highest risk fractures for developing acute compartment syndrome due to the muscle bulk and limited fascial expansion in the lower leg.
*
Aetiology:
Swelling within the confined fascial compartments due to hemorrhage, edema, or reperfusion injury, leading to increased intracompartmental pressure and compromised perfusion.
*
Recognition:
Early recognition is paramount. The classic "6 Ps" (Pain out of proportion, Pallor, Pulselessness, Paresthesia, Paralysis, Poikilothermia) are taught, but pain (especially with passive stretch) and paresthesia are the most reliable early signs.
*
Management:
Immediate four-compartment fasciotomy is required. Delayed diagnosis can lead to irreversible muscle necrosis and nerve damage.
Post-Operative Rehabilitation Protocols
A structured and progressive post-operative rehabilitation protocol is essential for restoring function and preventing long-term disability following intramedullary nailing of proximal tibial diaphyseal fractures. The protocol must be tailored to the individual patient, considering fracture stability, soft tissue status, and comorbidities.
Phase 1: Immediate Post-Operative (Day 0 - Week 2)
Goals:
* Pain and edema control.
* Protect healing fracture and soft tissues.
* Prevent stiffness (knee and ankle).
* Maintain muscle tone in unaffected areas.
Activities:
*
Pain Management:
Multimodal analgesia (NSAIDs, acetaminophen, opioids, nerve blocks).
*
Edema Control:
Elevation of the extremity (above heart level), cryotherapy.
*
Weight-Bearing (WB) Status:
*
Stable Nailing (non-comminuted, good cortical contact):
Touch-down weight-bearing (TDWB) or partial weight-bearing (PWB) of 10-25% body weight, using crutches or a walker.
*
Unstable Nailing (comminuted, poor cortical contact, large defects):
Non-weight-bearing (NWB) with crutches or walker.
*
Note:
The decision regarding WB is guided by the surgeon based on intra-operative stability and fracture characteristics.
*
Range of Motion (ROM):
*
Knee:
Gentle active and passive knee flexion and extension to tolerance, aiming for 0-90 degrees by the end of this phase. Patellar mobilization exercises.
*
Ankle:
Active ankle dorsiflexion and plantarflexion, inversion and eversion.
*
Muscle Activation:
* Isometric quadriceps sets, gluteal sets, and ankle pumps (to prevent DVT).
*
Wound Care:
Monitor incision for signs of infection, keep dressings clean and dry.
Phase 2: Early Mobilization & Strengthening (Weeks 2 - 6)
Goals:
* Gradually increase weight-bearing.
* Improve knee and ankle ROM.
* Initiate gentle strengthening.
* Restore normal gait pattern.
Activities:
*
Weight-Bearing:
Progress from TDWB/PWB to 50% WB as tolerated, depending on radiographic signs of early callus formation and clinical stability.
*
ROM:
Continue knee and ankle ROM exercises. Aim for >110 degrees knee flexion.
*
Strengthening:
*
Knee:
Continue isometric quadriceps. Begin straight leg raises, gentle hamstring curls, knee extensions (short arc), wall slides.
*
Ankle:
Resistive ankle exercises (theraband).
*
Hip:
Hip abduction/adduction, flexion/extension exercises.
*
Gait Training:
Focus on proper gait mechanics with assistive devices.
*
Stationary Cycling:
May be initiated if sufficient knee ROM and no pain.
Phase 3: Progressive Strengthening & Full Weight-Bearing (Weeks 6 - 12)
Goals:
* Achieve full weight-bearing without assistive devices (if fracture healed).
* Significantly improve strength, endurance, and proprioception.
* Restore full, pain-free ROM.
Activities:
*
Weight-Bearing:
Progress to full weight-bearing (FWB) as tolerated, once radiographic evidence confirms early to mid-stage fracture healing (e.g., bridging callus on at least 3 cortices) and clinical stability. Discontinue assistive devices as appropriate.
*
ROM:
Continue to work on any residual deficits.
*
Strengthening:
*
Leg Press:
Gradual progression of resistance.
*
Squats/Lunges:
Shallow initially, progressing deeper as tolerated.
*
Calf Raises:
Bilateral then unilateral.
*
Balance and Proprioception:
Single leg stance, wobble board/BAPS board exercises.
*
Core Strengthening:
Important for overall stability.
*
Cardiovascular:
Continue stationary cycling, consider swimming or elliptical.
Phase 4: Advanced Strengthening & Return to Activity (Weeks 12 onwards, or until full recovery)
Goals:
* Maximize strength, power, and agility.
* Gradual return to sport or high-impact activities.
* Prevent re-injury.
Activities:
*
Advanced Strengthening:
Progressive resistance exercises, plyometrics (jumping, hopping), sport-specific drills.
*
Agility Drills:
Ladder drills, cone drills, changes of direction.
*
Running Program:
Gradual progression from light jogging to running, ensuring no pain or swelling.
*
Return to Sport/Work:
A gradual, structured return to high-impact activities or demanding work is permitted only after full fracture union, symmetrical strength and ROM, and clearance from the surgeon and physical therapist. This may take 6-12 months or longer.
*
Hardware Removal:
If hardware is symptomatic (e.g., anterior knee pain), hardware removal may be considered after 12-18 months, or once the fracture is fully healed and mature. A period of protected weight-bearing may be advised post-removal.
Monitoring:
Regular clinical and radiographic follow-up appointments are crucial to assess fracture healing, monitor for complications, and guide rehabilitation progression. Any signs of pain, swelling, or instability warrant re-evaluation of the protocol. Patient education on activity modification and adherence to the rehabilitation program is paramount for optimal outcomes.
Summary of Key Literature / Guidelines
Intramedullary nailing has become the workhorse for tibial diaphyseal fracture management, and extensive literature supports its efficacy, especially when addressing the complexities of proximal tibia fractures.
Evidence for Intramedullary Nailing
- Gold Standard: Numerous studies and clinical experience have established IM nailing as the preferred treatment for most tibial diaphyseal fractures. Its biomechanical advantages, including load-sharing properties and relative biological friendliness (minimal soft tissue stripping compared to plating), lead to faster time to union and lower complication rates.
- Load Sharing vs. Load Bearing: IM nails function as load-sharing devices, allowing axial forces to be transmitted through the bone, which theoretically promotes callus formation and accelerates healing. In contrast, plates are load-bearing, shielding the bone from stress and potentially contributing to stress protection osteopenia.
- Open Fractures: For Gustilo-Anderson Type I, II, and IIIA open tibial fractures, IM nailing following aggressive debridement and irrigation is associated with lower infection rates compared to external fixation or plate fixation, provided soft tissue coverage is adequate.
Suprapatellar vs. Infrapatellar Nailing
- Infrapatellar Approach: The traditional approach, often requiring hyperflexion of the knee, which can be challenging in polytrauma patients or those with pre-existing knee stiffness. Concerns exist regarding anterior knee pain and potential patellar tendon damage.
-
Suprapatellar Approach:
Growing evidence suggests potential advantages, particularly for proximal tibial fractures.
- Alignment: Studies suggest that the suprapatellar approach may result in better initial alignment, especially for sagittal plane (procurvatum) deformities, due to a more in-line nail trajectory that does not require the nail to change direction as acutely.
- Entry Point: Provides a more favorable entry point for very proximal fractures, potentially reducing malalignment.
- Anterior Knee Pain: While some studies report similar rates of anterior knee pain, others suggest a trend towards lower rates with the suprapatellar approach.
- Complications: While initial concerns regarding patellofemoral cartilage damage were raised, recent meta-analyses have shown comparable rates of patellofemoral pain and chondral injury between suprapatellar and infrapatellar approaches.
- Ease of Use: May be technically easier in obese patients or those with large thigh musculature.
Role of Blocking Screws (Poller Screws)
- Effectiveness: The use of blocking screws is a well-established and highly effective technique to improve and maintain reduction in metaphyseal-diaphyseal fractures, particularly in the proximal tibia where the wide canal and strong deforming forces make sagittal and coronal plane control difficult.
- Literature Support: Numerous clinical studies and biomechanical analyses have demonstrated that blocking screws significantly reduce rates of malunion in proximal and distal tibial fractures treated with IM nailing. They enhance the stability of the nail-bone construct by creating a narrower channel for the nail, thereby improving cortical contact and restricting undesirable angulation.
- Reduced Malunion: Meta-analyses consistently show that the application of blocking screws can significantly decrease the incidence of valgus and procurvatum malunions, which are otherwise common in these challenging fracture patterns.
Timing of Surgery
- Polytrauma: Early definitive fixation (within 24 hours) of tibial fractures in hemodynamically stable polytrauma patients (Early Total Care) is generally recommended to reduce the systemic inflammatory response and potential for complications like ARDS and fat embolism syndrome.
- Damage Control Orthopedics (DCO): In unstable polytrauma patients, DCO may be employed, involving initial temporary external fixation followed by definitive IM nailing once the patient is physiologically optimized.
Antibiotic Prophylaxis
- Standard practice dictates the use of prophylactic antibiotics (e.g., Cefazolin) prior to incision for all operative fracture fixations to reduce the risk of surgical site infection, with adjusted protocols for open fractures based on Gustilo-Anderson classification.
Future Directions
- Navigation and Robotics: Emerging technologies in surgical navigation and robotic assistance may further enhance precision in guidewire placement, reaming, and nail insertion, potentially optimizing alignment and reducing technical errors, especially for complex proximal fractures.
- New Implant Designs: Ongoing development of IM nails with enhanced locking configurations, specialized bend designs, and improved biomaterials continues to aim for better stability and outcomes in challenging fracture patterns.
- Biologics: The use of adjuncts like bone morphogenetic proteins (BMPs) and platelet-rich plasma (PRP) continues to be investigated for their role in enhancing fracture healing, particularly in high-risk fractures or nonunions, though their routine use in primary IM nailing remains controversial and not universally recommended without specific indications.
In conclusion, the management of proximal tibial diaphyseal fractures with IM nailing requires a deep appreciation of surgical anatomy, deforming forces, and meticulous technique. While the challenges are significant, the judicious application of established principles, including precise entry portal placement, active reduction maneuvers, and the strategic use of blocking screws, coupled with modern implant designs, yields predictable and favorable outcomes for the vast majority of patients.
