Trauma Case 60 TIBIAL DIAPHYSEAL FRACTURE (PROXIMAL)
Patient Presentation & History
A 38-year-old male presented to the emergency department following a high-energy motorcycle accident. He was the driver and was ejected from the vehicle after colliding with a stationary object. Initial assessment by paramedics noted a deformed right lower leg and significant pain, with no gross open wounds. The patient was hemodynamically stable on arrival.
His past medical history was significant for well-controlled Type 2 Diabetes Mellitus (HbA1c 6.8%) and a smoking history of 15 pack-years. He reported no known allergies. His regular medications included metformin. He had no prior surgical history. The last oral intake was approximately 6 hours prior to the accident.
Upon initial trauma survey, the patient had no evidence of head injury, chest trauma (bilateral air entry, normal breath sounds), or abdominal injury (soft, non-tender abdomen). Pelvis was stable to compression. The primary injury concern was to the right lower extremity.
Clinical Examination
Following the primary survey and stabilization in the trauma bay, a focused secondary survey was performed, with particular attention to the injured extremity.
Initial Assessment
- General: Patient was alert and oriented, in moderate to severe pain, but cooperative.
- Vitals: BP 130/80 mmHg, HR 92 bpm, RR 16 breaths/min, SaO2 99% on room air.
Local Examination of the Right Lower Extremity
- Inspection: Gross deformity of the right lower leg with obvious angulation in the proximal third. Significant swelling and ecchymosis were noted, particularly over the anteromedial aspect of the proximal tibia. The skin integrity was intact, with no evidence of open wounds or significant skin tenting suggestive of impending compromise, though blistering was not yet present. No visible bone fragments.
-
Palpation:
- Marked tenderness to palpation circumferentially around the proximal tibia, consistent with a fracture.
- Crepitus was elicited with gentle manipulation.
- Assessment of compartment pressures was performed due to the high-energy mechanism and significant swelling. All four compartments (anterior, lateral, deep posterior, superficial posterior) felt tense but soft, without the classic "wood-like" feel, and pain with passive stretch of toes was not disproportionate. Serial assessments were planned.
-
Range of Motion (ROM):
- Active and passive knee ROM was severely limited due to pain.
- Ankle dorsiflexion and plantarflexion were painful but achievable, though limited by pain and swelling. No specific instability detected in the knee or ankle, but a full ligamentous exam was deferred due to pain and fracture instability.
-
Neurovascular Assessment:
-
Vascular:
- Distal pulses (dorsalis pedis and posterior tibial) were palpable and strong bilaterally (2+/4+).
- Capillary refill time in the toes was less than 2 seconds.
- Skin temperature and color were normal. No expanding hematoma.
-
Neurological:
-
Motor:
- Ankle dorsiflexion (deep peroneal nerve): Present, 4/5.
- Great toe extension (deep peroneal nerve): Present, 4/5.
- Ankle plantarflexion (tibial nerve): Present, 4/5.
- Toe flexion (tibial nerve): Present, 4/5.
- Peroneal longus/brevis (superficial peroneal nerve): Present, 4/5.
-
Sensation:
- First web space (deep peroneal nerve): Intact.
- Dorsum of foot (superficial peroneal nerve): Intact.
- Plantar aspect of foot (tibial nerve): Intact.
- Medial aspect of leg (saphenous nerve): Intact.
- Lateral aspect of foot (sural nerve): Intact.
-
Motor:
-
Vascular:
The clinical findings were highly suggestive of a closed, displaced, proximal tibial diaphyseal fracture. Given the high-energy mechanism and findings, imaging was immediately pursued.
Imaging & Diagnostics
Radiographs
Initial plain radiographs of the right lower leg were obtained in the emergency department, including anterior-posterior (AP) and lateral views encompassing the entire tibia, from the knee to the ankle joint.
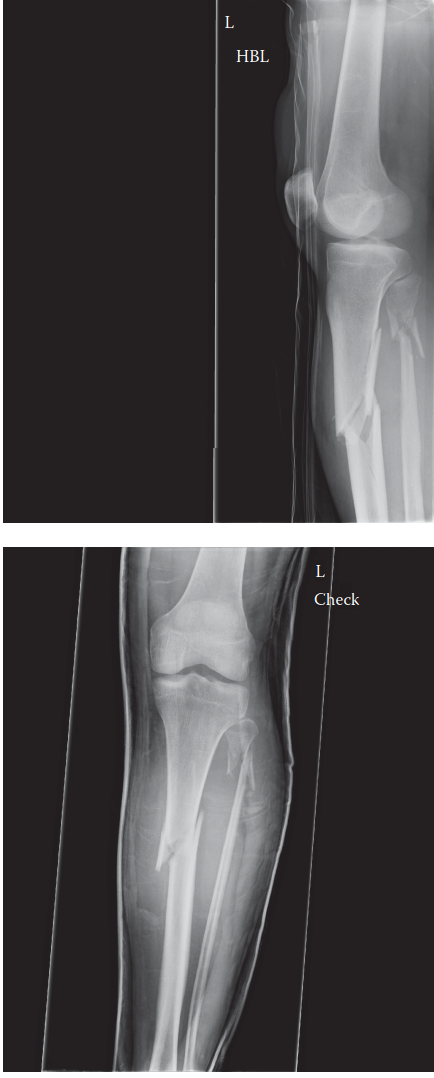
- Findings from Image Analysis (interpreting the provided image as an example): The radiographs demonstrate a displaced, comminuted fracture involving the proximal third of the tibial diaphysis. The fracture pattern appears oblique with a significant butterfly fragment on the medial aspect. There is apex posterior angulation, approximately 15 degrees, and approximately 10 degrees of valgus angulation. Shortening is estimated at 1.5-2 cm. No clear intra-articular extension into the knee or ankle joint was immediately evident on plain films, though this would need to be thoroughly evaluated. The fibula also shows a fracture at the level of the tibial fracture, which is common in high-energy tibial shaft fractures.
Computed Tomography (CT) Scan
A CT scan of the right tibia, including the knee, was subsequently performed to further delineate the fracture characteristics, assess for occult intra-articular extension, and aid in pre-operative planning.
*
Indications:
Complex fracture pattern, concern for intra-articular involvement despite plain film appearance, and detailed assessment of comminution and fragment displacement.
*
Findings:
The CT confirmed the highly comminuted oblique fracture of the proximal tibial diaphysis, classified as an AO/OTA 42-C2 fracture. It ruled out significant intra-articular involvement of the tibial plateau or plafond. The fibular fracture was also confirmed, with no significant displacement or impact on ankle stability. CT also provided valuable information regarding the size and location of cortical defects and the presence of any additional occult fracture lines, which are crucial for implant selection and planning reduction maneuvers.
Other Diagnostics
- Laboratory Tests: Routine pre-operative blood work including complete blood count, basic metabolic panel, coagulation profile, and type and screen was ordered. All were within acceptable limits for surgery. Given the patient's diabetic status, an updated HbA1c was obtained and found to be 6.8%, indicating reasonably controlled diabetes.
- Vascular Studies: Given palpable pulses and normal capillary refill, no immediate arterial doppler or angiography was indicated. However, in cases of diminished pulses or suspicion of vascular injury, these would be paramount.
Templating
Pre-operative templating was performed using digital imaging software. This involved:
* Measuring the length of the intact contralateral tibia (if accessible) or estimating based on radiographic landmarks.
* Determining the appropriate intramedullary nail length and diameter. The anticipated nail diameter was 10-11mm, with a length of 280-300mm.
* Planning the entry point for the intramedullary nail (infrapatellar vs. suprapatellar).
* Considering the placement of blocking screws (Poller screws) to address the apex posterior and valgus deformity often encountered in proximal tibial diaphyseal fractures.
Differential Diagnosis
The primary diagnosis is a closed, comminuted, displaced proximal tibial diaphyseal fracture. However, it is essential to consider other potential diagnoses or concurrent injuries in the differential, especially in the setting of high-energy trauma.
| Feature | Proximal Tibial Diaphyseal Fracture (Primary) | Proximal Tibial Metaphyseal Fracture | Tibial Plateau Fracture | Stress Fracture of Tibia |
|---|---|---|---|---|
| Location | Diaphysis, proximal third | Metaphyseal region of the proximal tibia | Intra-articular, involving the tibial condyles | Anywhere in tibia, often mid-distal shaft |
| Mechanism of Injury | High-energy direct/indirect trauma (e.g., MVC, fall from height, pedestrian vs. car) | High-energy axial load or angular forces, often with valgus/varus stress | High-energy axial load with valgus/varus force, or direct trauma to knee | Repetitive microtrauma, overuse, sudden increase in activity |
| Clinical Presentation | Gross deformity, severe pain, swelling, inability to bear weight. Possible neurovascular compromise. | Similar to diaphyseal, but pain often localized closer to the knee joint. | Marked knee effusion, instability, severe pain localized to knee. Possible ligamentous injury. | Insidious onset of pain with activity, relieved by rest. Focal tenderness. No gross deformity. |
| Imaging Findings (X-ray) | Oblique, transverse, spiral, or comminuted fracture of the shaft. +/- associated fibula fracture. | Fracture line extending into the metaphysis, but typically not intra-articular. | Fracture lines extending into the articular surface of the tibial condyles. Joint step-off, widening, depression. | Subtle cortical break or periosteal reaction. Often negative on initial films; may require MRI. |
| Associated Injuries | Compartment syndrome, neurovascular injury, ipsilateral knee ligamentous injury (floating knee). | Similar to diaphyseal; potential for knee ligamentous or meniscal injury. | Meniscal tears, ligamentous injuries (ACL, PCL, MCL, LCL), popliteal artery injury, common peroneal nerve injury. | Rarely associated acute injuries; chronic overuse phenomenon. |
| Management Principles | Operative: Intramedullary nailing (gold standard). Plate fixation for specific patterns. | Operative: Plate fixation (LCPs), often requiring contouring. External fixation as temporary measure. | Operative: ORIF with plate/screws for articular reconstruction. Non-operative for stable, minimally displaced fractures. | Non-operative: Rest, activity modification, bracing. Seldom operative unless non-union or high-risk location. |
Surgical Decision Making & Classification
Operative vs. Non-operative
Given the patient's closed, displaced, comminuted proximal tibial diaphyseal fracture, operative intervention was the definitive treatment of choice.
*
Indications for Operative Fixation in this case:
*
Displacement and Instability:
Significant displacement, angulation, and comminution preclude successful non-operative management, which would inevitably lead to malunion and functional impairment.
*
Comminution:
The butterfly fragment and overall comminution suggest an unstable fracture pattern.
*
High-Energy Mechanism:
Implies significant soft tissue injury and a higher risk of complications with non-operative care.
*
Patient Demands:
A 38-year-old active male requires restoration of limb alignment and stability to facilitate early mobilization and return to function.
*
Contraindications to Immediate Operative Fixation:
*
Compromised Soft Tissue Envelope:
While not present at admission, close monitoring for skin blistering or impending compartment syndrome is critical. In such cases, a staged approach with external fixation might be considered.
*
Patient Instability:
Uncontrolled polytrauma or medical instability requiring damage control orthopedics, which was not the case here.
Fracture Classification
The fracture was classified using the
AO/OTA Classification System
and described by its location and pattern:
*
Location:
4 (tibia/fibula), 2 (diaphysis) ->
42
.
*
Pattern:
C2
(complex, comminuted fracture with a segmental fragment and extensive soft tissue injury).
* Specifically, a
42-C2.3
fracture, indicating a complex, comminuted fracture of the proximal third of the tibial diaphysis.
If the fracture had been open, the
Gustilo-Anderson Classification
would have been applied:
*
Type I:
<1 cm wound, clean.
*
Type II:
1-10 cm wound, moderate contamination, no extensive soft tissue damage.
*
Type III:
>10 cm wound, extensive soft tissue damage, high contamination. Further subdivided into IIIA, IIIB, IIIC (vascular injury).
For this patient, given it was a closed fracture, the Gustilo-Anderson classification was not applicable.
Timing of Surgery
The surgery was planned for the following day (within 12-24 hours) as an urgent, but not emergent, procedure. This allowed for adequate pre-operative workup, medical optimization (diabetes control), limb elevation to reduce swelling, and thorough surgical planning. This falls under the concept of Early Total Care (ETC) within a safe time window, optimizing outcomes and minimizing complications like fat embolism and prolonged hospital stay.
Surgical Technique / Intervention
The gold standard for fixation of tibial diaphyseal fractures is intramedullary nailing, offering excellent biomechanical stability, load sharing, and high union rates.
Pre-Operative Preparation
- Consent: Detailed consent obtained, discussing risks including infection, nonunion, malunion, neurovascular injury, compartment syndrome, hardware irritation, and the need for future hardware removal.
- Antibiotics: Pre-operative intravenous antibiotics (e.g., Cefazolin) administered within 60 minutes of incision.
- Pain Management: Appropriate pre-emptive analgesia provided.
- Anesthesia: General anesthesia was chosen.
Patient Positioning
The patient was positioned supine on a radiolucent operating table.
* The affected right leg was placed on a traction table, with a boot applied to the foot to allow for sustained traction and manipulation for reduction. Alternatively, a bump could be placed under the ipsilateral hip to internally rotate the limb and facilitate access.
* The knee was flexed approximately 90 degrees to expose the infrapatellar region, allowing for an infrapatellar entry point.
* A tourniquet was placed high on the thigh but typically not inflated unless bleeding control became an issue, to preserve soft tissue perfusion.
* Image intensifier (fluoroscopy) was positioned to allow for clear AP and lateral views of the entire tibia, knee, and ankle.
Surgical Approach & Entry Point
A standard infrapatellar approach was chosen.
* A small longitudinal incision, approximately 3-4 cm, was made just medial to the patellar tendon, distal to the patella.
* The patellar tendon was retracted laterally, and the infrapatellar fat pad was gently mobilized.
* The entry portal into the medullary canal was established at the junction of the medial and central thirds of the intercondylar notch, just anterior to the anterior cruciate ligament (ACL) footprint. This specific location is crucial to prevent valgus/varus malalignment of the nail. A guide wire was advanced under fluoroscopic guidance to ensure correct positioning and trajectory down the shaft.
* Reaming of the entry portal was performed using a cannulated reamer to create a funnel shape, preventing stress risers and facilitating nail insertion.
Reduction Techniques
Achieving and maintaining reduction of a proximal tibial diaphyseal fracture can be challenging due to the deforming forces of the gastrocnemius (causing apex posterior angulation) and the pes anserinus muscles (causing valgus deformity).
*
Traction:
Initial length was restored using traction table.
*
Manual Manipulation:
The surgeon or an assistant applied manual forces (distraction, translation, rotation) to align the fragments.
*
Direct Reduction:
While minimally invasive, direct reduction using a pointed reduction clamp or a small Hohmann retractor was sometimes necessary for the large butterfly fragment.
*
Blocking Screws (Poller Screws):
This was a critical step in this case given the proximal fracture location and propensity for malalignment.
* To correct apex posterior angulation: One or two screws were placed
anteriorly
into the proximal fragment, away from the planned nail path, effectively blocking the nail from pushing the distal fragment posteriorly.
* To correct valgus angulation: One or two screws were placed
medially
into the proximal fragment to prevent the nail from entering in a more lateral trajectory and pushing the distal fragment into valgus.
* Fluoroscopy was used meticulously to ensure proper placement of blocking screws without compromising the nail path or neurovascular structures.
*
External Fixator-Assisted Reduction:
In some complex cases or when indirect methods fail, a temporary external fixator can be used to achieve and hold reduction prior to IMN. This was not required in this particular case.
Intramedullary Nailing
Once satisfactory reduction was achieved and confirmed fluoroscopically:
* A ball-tipped guide wire was advanced across the fracture site and into the distal tibial metaphysis, ensuring it was centrally placed in both AP and lateral views.
*
Reaming:
The medullary canal was progressively reamed over the guide wire. Incremental reaming (0.5 mm increments) was performed until cortical chatter was felt, typically 1.0-1.5 mm larger than the chosen nail diameter. Reaming helps to consolidate the fracture, enhance stability, and improve biological healing.
*
Nail Insertion:
The appropriately sized intramedullary nail (10mm diameter, 290mm length) was inserted over the guide wire. The nail was gently advanced across the fracture site and down into the distal fragment, ensuring central placement and maintaining reduction. The curved tip of the nail typically facilitates passage.
*
Proximal Locking:
Once the nail was seated to the desired depth (distal to the knee joint line but allowing for at least two proximal locking screws), proximal interlocking screws were placed. Two mediolateral screws were used to provide rotational stability and prevent shortening.
*
Distal Locking:
Distal locking screws were placed using a freehand technique or a targeting guide. Two screws in AP projection were inserted, ensuring appropriate length to achieve bicortical purchase. Dynamic locking was considered if there was concerns about delayed union, but static locking was chosen for robust stabilization in this high-energy comminuted fracture.
* Final fluoroscopic images confirmed proper nail position, locking screw placement, and acceptable alignment (less than 5 degrees of angulation in any plane, less than 5 degrees of rotation, and less than 1 cm of shortening).
Wound Closure
The incision was thoroughly irrigated. The wound was closed in layers: deep fascia, subcutaneous tissue, and skin with sutures or staples. A sterile dressing was applied.
Post-Operative Protocol & Rehabilitation
Immediate Post-Operative Care (Days 0-7)
- Pain Management: Multimodal analgesia including opioids, NSAIDs (if no contraindications), and regional nerve blocks.
- Wound Care: Daily dressing changes, monitoring for signs of infection (erythema, swelling, discharge). Staples/sutures typically removed at 2 weeks.
- Neurovascular Checks: Frequent monitoring of distal pulses, capillary refill, motor, and sensory function.
- Compartment Syndrome Monitoring: Close observation for disproportionate pain, paresthesias, pain with passive stretch, and tense compartments.
- DVT Prophylaxis: Pharmacological (e.g., LMWH) and mechanical (e.g., SCDs) prophylaxis initiated.
- Weight Bearing: Non-weight bearing (NWB) or touch-down weight bearing (TDWB) of 10-15 kg with crutches or a walker. This allows for soft tissue healing and minimizes stress on the fracture site while encouraging early motion.
- Range of Motion: Gentle active and passive range of motion exercises for the knee and ankle, within pain limits, to prevent stiffness. Continuous passive motion (CPM) may be utilized for knee ROM.
Early Rehabilitation (Weeks 2-6)
- Physical Therapy: Formal physical therapy initiated.
-
Weight Bearing Progression:
- Gradual progression to protected weight bearing (PWB) as pain allows and radiographic signs of early callus formation are noted. This often begins around 4-6 weeks post-op.
- Emphasis on maintaining proper gait mechanics with crutches/walker.
- Strengthening: Isometric quadriceps, hamstring, and calf strengthening exercises.
- ROM: Continue with knee and ankle ROM exercises to restore full flexion and extension.
Intermediate Rehabilitation (Months 2-4)
- Radiographic Assessment: Regular follow-up radiographs (e.g., at 6 weeks, 3 months, 6 months) to monitor fracture healing, callus formation, and alignment.
- Weight Bearing: Progression to full weight bearing (FWB) once there is clear radiographic evidence of bridging callus in at least three cortices and absence of pain with weight-bearing. This often occurs around 12-16 weeks.
- Strength and Conditioning: Progressive resistance exercises for major muscle groups of the affected limb.
- Proprioception and Balance: Begin balance and proprioceptive training.
- Functional Activities: Work on walking endurance, stair climbing, and regaining activities of daily living.
Late Rehabilitation & Return to Activity (Months 4+)
- Full Union: Radiographic confirmation of complete fracture union.
- Advanced Strengthening: Plyometrics, sport-specific training for athletes, or occupational-specific training.
- Return to Work/Sport: Gradual return to full activities, guided by clinical and radiographic union, strength, and functional capacity.
- Hardware Removal: Considered for symptomatic hardware (pain, bursitis, impingement), or in younger, active individuals after complete union, typically 12-18 months post-op. This is an elective procedure with its own risks.
Monitoring for Complications
Throughout the post-operative period, close monitoring for potential complications is essential:
*
Infection:
Superficial or deep.
*
Nonunion/Delayed Union:
Lack of healing by 6-9 months or progression to nonunion.
*
Malunion:
Persistent angulation, rotation, or shortening that impacts function.
*
Hardware Failure:
Breakage or loosening of the nail or screws.
*
Compartment Syndrome:
Although rarer after definitive fixation, still a possibility.
*
Neurovascular Injury:
New or persistent deficits.
*
Chronic Regional Pain Syndrome (CRPS).
*
Hardware Irritation:
Particularly from prominent proximal or distal locking screws.
*
Fat Embolism Syndrome (FES):
Although higher risk during reaming, monitoring continues post-op.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls for Proximal Tibial Diaphyseal Fractures
- Thorough Pre-operative Planning: This is paramount. Understand the fracture morphology from AP, lateral, and CT images. Template nail size, anticipate reduction challenges, and plan for blocking screws.
- Correct Entry Point for IMN: The entry point significantly influences alignment. Medial parapatellar infrapatellar entry is preferred to prevent valgus deformity and avoid the Hoffa's fat pad. Suprapatellar entry can be an option for very proximal fractures, obese patients, or those with significant knee flexion contractures, offering a more direct trajectory. Avoid a lateral entry point as it often leads to valgus malalignment.
- Recognize Deforming Forces: The gastrocnemius causes apex posterior angulation, while the pes anserinus (sartorius, gracilis, semitendinosus) can contribute to valgus deformity. Anticipate these and plan reduction strategies.
-
Strategic Use of Blocking Screws (Poller Screws):
These are invaluable for controlling proximal tibial shaft fractures.
- To correct apex posterior angulation: Place screws anteriorly in the proximal fragment.
- To correct valgus angulation: Place screws medially in the proximal fragment.
- Place them parallel to the nail path, outside the reamed canal, to guide the nail centrally and maintain reduction.
- Achieve and Maintain Rotational Alignment: Compare the alignment of the foot and ankle to the patella (foot-thigh angle) throughout the procedure. Malrotation is a common and functionally debilitating complication.
- Full Length Radiographs: Always obtain full-length AP and lateral radiographs to ensure the entire fracture is visualized, including the knee and ankle joints, and to assess for associated injuries.
- Serial Compartment Monitoring: High-energy tibial fractures carry a significant risk of compartment syndrome. Maintain a high index of suspicion and perform serial clinical exams, or consider compartment pressure monitoring if warranted.
- Soft Tissue Management: Preserve the soft tissue envelope as much as possible. Minimally invasive approaches are preferred for IMN. In open fractures, meticulous debridement and appropriate wound management are critical.
Pitfalls to Avoid
- Inadequate Reduction: Particularly apex posterior angulation (flexion deformity) and valgus malalignment are common in proximal tibial diaphyseal fractures due to muscle pull. Failure to correct these leads to symptomatic malunion and gait disturbances.
- Malrotation: This is often clinically evident only post-operatively and can be very debilitating. Always check rotational alignment intraoperatively (e.g., by comparing foot position to patella or by visualizing the ankle mortise).
- Missing Associated Injuries: Especially ipsilateral knee ligamentous injuries (e.g., ACL, PCL, collateral ligaments) or occult ankle fractures. A "floating knee" injury (ipsilateral femoral and tibial fractures) requires careful management.
- Aggressive Reaming in Unstable Patients: While reaming offers benefits, it can increase the risk of fat embolism in polytrauma patients. Consider unreamed nails in severely compromised patients if indicated.
-
Iatrogenic Injury:
- Neurovascular Damage: During approaches, drilling, or screw placement.
- Patellar Tendon Injury: During entry point creation.
- Meniscal or Cartilage Damage: With an improper entry point or excessive manipulation.
- Damage to Infrapatellar Branch of Saphenous Nerve: Common cause of numbness around the incision.
- Under-sizing the Nail: Using a nail that is too small in diameter or too short can lead to implant failure, insufficient stability, and increased risk of delayed union/nonunion.
- Premature Weight Bearing: Leading to implant failure, loss of reduction, or delayed union.
- Inadequate Management of Open Fractures: Failure to appropriately debride, irrigate, and manage soft tissues in open fractures drastically increases infection risk and leads to poor outcomes.
- Ignoring the Fibular Fracture: While often a stable fracture, assess its contribution to overall stability and potential for affecting rotational alignment or ankle stability (e.g., in very distal fibular fractures). In most diaphyseal cases, the fibula is not directly addressed.
