INTRODUCTION TO FLEXOR CARPI ULNARIS TRANSFER
The transfer of the flexor carpi ulnaris (FCU) dorsally to a radial wrist extensor is a cornerstone procedure in the reconstructive armamentarium for the spastic or paralytic upper extremity. Most commonly utilized in patients with cerebral palsy, post-stroke spastic hemiplegia, or specific peripheral nerve palsies, this procedure serves a dual biomechanical purpose. First, it removes a primary deforming force that pulls the hand into severe ulnar deviation and volar flexion. Second, it repurposes that same muscle to provide a dynamic force that promotes supination of the forearm and extension of the wrist.
By converting a deforming flexor into an active extensor, the surgeon can dramatically improve both the functional capacity and the cosmetic appearance of the compromised hand. However, the success of this operation is heavily dependent on meticulous patient selection, precise preoperative planning, and flawless surgical execution.
PREOPERATIVE EVALUATION AND INDICATIONS
For the FCU transfer to be effective, the patient must present with a favorable diagnostic profile. Tendon transfers rely on the passive mobility of the joints they cross and the active control of the surrounding musculature.
Prerequisites for Surgery
- Active Finger Extension: The patient must possess the ability to actively extend the digits. If the wrist is brought into extension by the transferred FCU, the tenodesis effect will naturally increase tension on the flexor tendons. Without adequate active finger extension, the patient will lose the ability to open the hand and release objects.
- Passive Flexibility: There must be full passive range of motion (ROM) in the hand, wrist, and forearm.
- Correction of Fixed Deformities: Any fixed flexion or pronation contractures must be aggressively corrected prior to, or concurrent with, the tendon transfer. This is typically achieved through successive serial casting or indicated soft tissue releases (e.g., fractional lengthening of the flexor digitorum superficialis or profundus).
Clinical Pearl: A wrist flexion deformity is frequently accompanied by a primary weakness of the finger extensors. In such cases, a child may only be able to release objects by utilizing the tenodesis effect—flexing the wrist to allow the fingers to passively extend. Transferring the FCU to the wrist extensors in this scenario will only strengthen the grasp, making it significantly more difficult, or impossible, for the child to release objects.
Electromyography (EMG) Considerations
Dynamic electromyography is an invaluable tool in preoperative planning. If EMG demonstrates continuous activity of the FCU during the release phase of the grasp-and-release cycle—especially in the presence of weak finger extension—transferring the FCU directly to the extensor digitorum communis (EDC) is highly recommended over transfer to the wrist extensors.
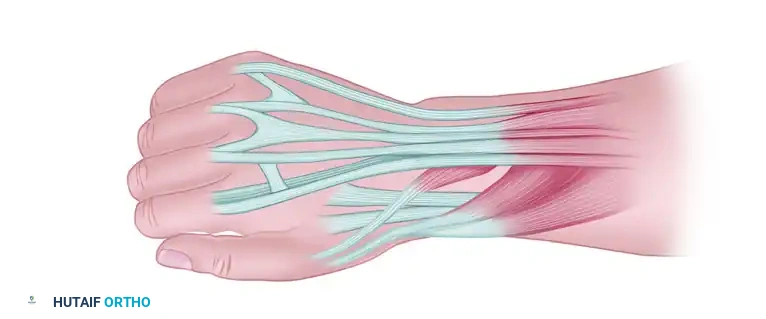
BIOMECHANICS AND RECIPIENT TENDON SELECTION
The choice of the recipient tendon dictates the postoperative biomechanics of the wrist and forearm. The surgeon must carefully evaluate the patient's specific deficits to select the appropriate target.
- Extensor Carpi Radialis Brevis (ECRB): The ECRB inserts centrally at the base of the third metacarpal. Transferring the FCU to the ECRB provides a centralized, balanced pull, making it the preferred choice for pure wrist extension without excessive radial deviation.
- Extensor Carpi Radialis Longus (ECRL): The ECRL inserts at the base of the second metacarpal. Transferring the FCU to the ECRL provides a stronger moment arm for forearm supination and radial deviation of the wrist. Wolf et al. demonstrated that FCU transfer to the ECRL significantly improved both function and cosmesis, achieving an average final wrist resting position of 9 degrees of extension.
- Extensor Digitorum Communis (EDC): Selected when the primary functional deficit is the inability to extend the fingers for object release, provided the wrist can be stabilized by other means.
Routing the Transfer: Subcutaneous vs. Interosseous
The anatomical path chosen for the transferred tendon profoundly affects its action on the forearm axis.
* Subcutaneous Ulnar Routing: Passing the tendon around the ulnar border of the forearm creates a strong supination moment. This is ideal for patients with a pronation deformity.
* Interosseous Membrane Routing: If the patient already possesses active supination prior to surgery, routing the FCU around the ulnar border may result in an over-supination deformity. In these cases, the muscle should be routed directly through a window in the interosseous membrane. This centralizes the force vector, preventing the FCU from acting as a supinator while preserving its new role as a wrist extensor.
Surgical Warning: The FCU transfer should never be performed in conjunction with a release or lengthening of the flexor carpi radialis (FCR). The FCR is the primary antagonist to the transferred FCU. Abolishing the FCR's stabilizing volar force while simultaneously augmenting dorsal extension will predictably result in a severe, debilitating hyperextension deformity of the wrist.
SURGICAL TECHNIQUE: GREEN AND BANKS METHOD
The following step-by-step technique is based on the foundational principles described by Green and Banks, optimized for modern orthopedic practice.
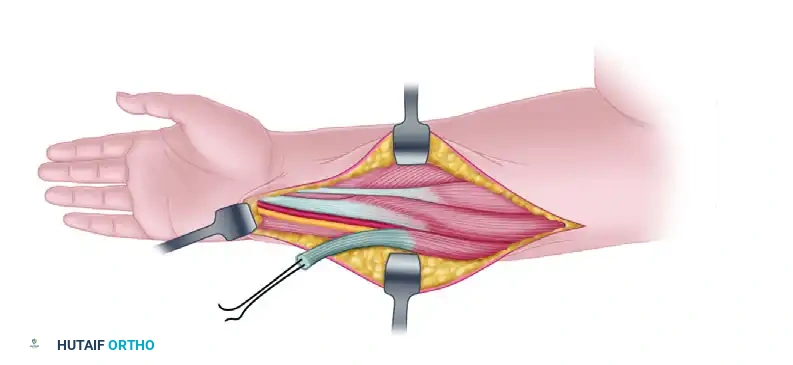
Phase 1: Distal Exposure and Harvest of the FCU
- Positioning and Incision: Place the patient supine with the arm extended on a hand table. Ensure a well-padded pneumatic tourniquet is applied to the proximal arm. Make an anterior longitudinal incision extending from the flexor crease of the wrist proximally for approximately 3 cm. This exposes the insertion of the FCU on the pisiform bone.
-
Tendon Detachment: Identify the FCU tendon at its insertion. Carefully detach the tendon directly from the pisiform bone to maximize length.
-
Distal Dissection: Dissect the tendon proximally. Place a heavy, non-absorbable nylon or core suture (e.g., Krackow or whipstitch) into the distal end of the tendon. By applying gentle traction to this suture, the proximal course of the muscle belly can be easily outlined beneath the forearm fascia.
Phase 2: Proximal Mobilization of the Muscle Belly
-
Proximal Incision: Beginning approximately 5 cm distal to the medial epicondyle of the humerus, make a second longitudinal incision, 7 to 10 cm in length, directly over the palpable belly of the FCU muscle.
-
Fascial Release: Define the lateral margin of the muscle. Incise the deep fascia along this margin to expose the deep surface of the muscle belly.
-
Ulnar Dissection: The attachment of the FCU muscle to the ulna often extends almost the full length of the tendon. Free the muscle from the ulna via sharp dissection, taking meticulous care to leave the ulnar periosteum intact.
Anatomic Pitfall: As the muscle is elevated from the ulna, the ulnar nerve and artery will be visualized in their fascial sheath immediately posterior and lateral to the tendon. Extreme caution must be exercised to protect the neurovascular bundle during this extensive mobilization.
- Muscle Delivery: Pull the detached distal tendon into the proximal incision. Continue to free the muscle belly proximally until it achieves a straight line of pull from its origin across the ulnar border to the dorsal aspect of the wrist.
- Nerve Preservation: Carefully locate and preserve the motor branches of the ulnar nerve entering the proximal third of the FCU muscle. These motor branches dictate the absolute limit of proximal dissection.
Phase 3: Preparation of the Dorsal Compartment
-
Septum Excision: To prevent kinking or tethering of the transferred muscle, identify the intermuscular septum separating the volar and dorsal compartments of the forearm at the medial margin of the ulna. Excise a 4 to 5 cm window of this septum to create a smooth, frictionless path to the dorsal compartment.
-
Dorsal Incision: Make a third incision, approximately 3 cm long, starting just proximal to the transverse skin crease on the dorsum of the wrist and extending proximally. This incision should be centered over the first and second extensor compartments to expose the ECRB and ECRL tendons.
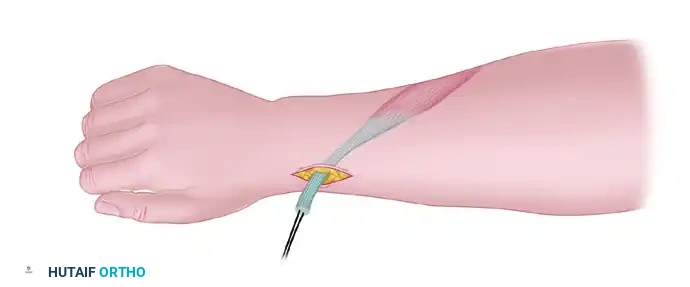
Phase 4: Tendon Routing and Fixation
-
Subcutaneous Passage: Using a curved tendon passer, direct the free end of the FCU from the proximal forearm incision, subcutaneously around the ulnar border of the forearm, and into the dorsal compartment. Guide it along the path of the extensor tendons toward the chosen recipient tendon (ECRB or ECRL). Ensure the tunnel is wide enough to accommodate the muscle belly without constriction.
-
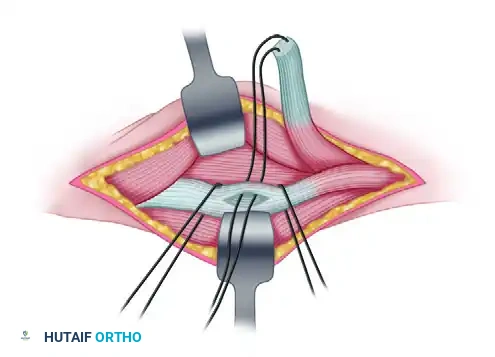
Recipient Preparation: Isolate the chosen recipient tendon (e.g., ECRB). Make a longitudinal buttonhole slit through the center of the recipient tendon.
-
Tendon Weave: Pass the distal end of the FCU tendon through the buttonhole in the recipient tendon. A Pulvertaft weave may be utilized if additional length and surface area are required for a robust repair.
-
Tensioning the Transfer: Setting the correct tension is the most critical step of the procedure.
- Traditional Tensioning: Suture the FCU tendon to the recipient tendon under moderate tension with the forearm held in full supination and the wrist in at least 45 degrees of extension.
- Manske's Modification: Manske prefers to tension the transfer by placing the wrist in slight flexion (15 degrees). This modification is designed specifically to avoid the complication of a postoperative hyperextension deformity. In our experience, hyperextension is rarely encountered provided the FCR has not been overlengthened or released.
- EDC Transfer Tensioning: If the FCU is being transferred to the EDC tendons, it must be sutured under sufficient tension so that when the wrist is held in a neutral position, the metacarpophalangeal (MCP) joints are held in hyperextension.

- Closure: Deflate the tourniquet, achieve meticulous hemostasis, and close the subcutaneous tissues and skin in a standard layered fashion.
POSTOPERATIVE CARE AND REHABILITATION
The success of a tendon transfer is equally dependent on the postoperative rehabilitation protocol. The newly transferred muscle must be protected while it heals, and the patient must undergo extensive motor re-education to learn how to fire the muscle in its new biomechanical role.
Immobilization Phase (Weeks 0-4)
- Immediately following wound closure, apply a well-padded, rigid long-arm cast.
- Cast Positioning: The cast must extend from just distal to the axilla down to the tips of the fingers.
- The limb is immobilized in the following position:
- Wrist: 30 to 45 degrees of extension.
- Forearm: Full supination.
- Fingers: Almost complete extension (MCPs and IP joints).
- Thumb: Full abduction and opposition.
- At 2 weeks postoperative, the initial cast is bivalved or removed to inspect the incisions and remove skin sutures. A new, well-fitting long-arm cast is immediately applied in the exact same position and worn for an additional 4 weeks.
Mobilization and Therapy Phase (Weeks 6 and Beyond)
- At 6 weeks post-surgery, the cast is permanently removed, and formal, intensive hand therapy is initiated.
- Motor Re-education: The primary goal of therapy is cortical remapping. The patient must learn to fire the FCU (originally a flexor) when attempting to extend the wrist. Biofeedback and neuromuscular electrical stimulation (NMES) are highly effective adjuncts during this phase.
- Splinting: Night splints are fabricated by the occupational therapist to maintain the hand and wrist in the corrected, extended position. These splints are used intermittently for several months, or up to a year, to prevent the recurrence of flexion contractures while the transferred tendon gains maximal tensile strength.
- Active range of motion exercises are progressed gradually. Passive stretching against the transfer is strictly avoided for the first 8 to 10 weeks to prevent elongation or rupture of the repair site.
COMPLICATIONS AND PITFALLS
While highly successful when executed correctly, the FCU transfer carries specific risks that the orthopedic surgeon must anticipate:
- Hyperextension Deformity: As previously noted, this is the most devastating complication, almost exclusively occurring when the FCR is simultaneously released. If hyperextension occurs, revision surgery to balance the volar forces may be required.
- Loss of Finger Flexion/Grasp: Over-tensioning the transfer, or transferring the tendon in a patient with unrecognized fixed MCP joint contractures, can severely impair the patient's ability to form a tight fist.
- Tendon Rupture or Attenuation: Usually a result of premature aggressive passive stretching or non-compliance with the postoperative casting protocol.
- Ulnar Nerve Injury: Direct trauma or traction injury to the ulnar nerve during the proximal mobilization of the FCU muscle belly. Careful dissection and visualization of the neurovascular bundle are mandatory.
By adhering strictly to biomechanical principles, respecting the delicate neurovascular anatomy, and ensuring rigorous postoperative rehabilitation, the transfer of the flexor carpi ulnaris remains a highly reliable procedure for restoring function and dignity to the spastic or paralytic upper extremity.
📚 Medical References
- Flexor carpi ulnaris transfer for radial nerve palsy: functional testing of long-term results, J Hand Surg 20A:737, 1995.
- Reid RL: Radial nerve palsy, Hand Clin 4:179, 1988.
- Revol M, Cormerais A, Laffont I, et al: Tendon transfers as applied to tetraplegia, Hand Clin 18:423, 2002.
- Richer RJ, Peimer CA: Flexor superfi cialis abductor transfer with
