Comprehensive Introduction and Patho-Epidemiology
The management of complex fractures involving the extensor mechanism and the distal femoral articular surface presents a formidable and highly nuanced challenge to the orthopedic surgeon. When high-energy trauma results in catastrophic comminution of the patella, or when shearing forces create displaced osteochondral fragments within the knee joint, meticulous surgical decision-making is paramount. Historically, the approach to severe patellar trauma was often aggressive excision; however, modern orthopedic philosophy dictates absolute preservation of the patella whenever biomechanically feasible. This comprehensive guide delineates the precise indications, biomechanical considerations, and exacting surgical techniques for total patellectomy as a salvage procedure, the biological fixation of osteochondral fractures, and the classification-driven management of complex distal femoral fractures.
The epidemiology of these injuries is characteristically bimodal, reflecting two distinct patient populations and injury mechanisms. High-energy trauma, such as motor vehicle collisions (specifically "dashboard injuries") and industrial accidents, predominantly affects young, active individuals. These mechanisms impart massive axial and shear loads across the flexed knee, resulting in severe stellate comminution of the patella, frequently accompanied by osteochondral shearing of the femoral condyles or complex intra-articular distal femur fractures. Conversely, low-energy falls in the osteoporotic elderly population can also result in significant comminution, though the soft tissue envelope is often less compromised. Understanding the energy of the injury is critical, as it directly correlates with the degree of soft tissue devitalization, articular cartilage damage, and the subsequent risk of post-operative complications.
Osteochondral fractures of the patella or distal femur frequently accompany lateral patellar dislocations or direct high-energy shear trauma. The pathoanatomy of these lesions involves the traumatic avulsion or shearing of articular cartilage along with a variable thickness of underlying subchondral bone. If left untreated, these fragments act as loose bodies, causing mechanical symptoms, recurrent effusions, and rapid acceleration of localized post-traumatic osteoarthritis. The management algorithm dictates that these fragments must be addressed acutely; delays in presentation lead to fibrous encapsulation of the fragment and rounding of the donor bed, rendering anatomical reduction and biological fixation nearly impossible.
The evolution of treatment modalities for these complex knee injuries reflects a broader paradigm shift in orthopedic trauma surgery. In the mid-20th century, nonoperative treatment methods or routine total patellectomies were commonplace due to the high failure rates of early internal fixation devices. However, with the advent of the AO foundation's principles of anatomical reduction, stable internal fixation, and preservation of blood supply, operative treatment has become the gold standard. Today, the integration of advanced imaging, locked plating technology, headless compression screws, and bioabsorbable fixation materials allows surgeons to reconstruct highly comminuted articular surfaces, thereby minimizing the need for salvage procedures like total patellectomy and maximizing the potential for early, functional rehabilitation.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy and biomechanics of the extensor mechanism and distal femur is the absolute foundation for successful operative intervention. The patella is the largest sesamoid bone in the human body, embedded within the quadriceps tendon. Osteologically, its posterior surface is divided into medial and lateral facets by a vertical ridge, with a smaller "odd" facet located on the extreme medial border. The arterial supply to the patella is highly precarious, relying on an extra-osseous anastomotic ring formed by the superior and inferior genicular arteries. The primary intra-osseous vascular supply enters the distal pole and travels proximally. Consequently, transverse fractures or aggressive surgical dissection can easily disrupt this retrograde blood supply, leading to avascular necrosis of the proximal pole.
The extensor mechanism is a complex dynamic and static stabilizing structure. The quadriceps femoris muscle group converges into the quadriceps tendon, which inserts into the superior pole of the patella. The patellar tendon originates from the inferior pole and inserts onto the tibial tubercle. Medially and laterally, the extensor mechanism is stabilized by the medial patellofemoral ligament (MPFL) and the lateral patellofemoral ligament (LPFL), respectively, which are contiguous with the broader medial and lateral retinacula. During any surgical exposure or repair, particularly following total patellectomy, the integrity of these retinacular expansions must be meticulously restored to prevent extensor lag and ensure proper tracking of the centralized tendinous repair.
Biomechanically, the patella serves as a critical fulcrum, increasing the moment arm of the quadriceps mechanism. By displacing the quadriceps tendon anteriorly away from the center of rotation of the tibiofemoral joint, the patella enhances knee extension torque by up to 30%. The joint reaction forces across the patellofemoral articulation are immense, ranging from half of body weight during normal level walking to up to seven or eight times body weight during deep squatting or stair climbing. The articular cartilage of the patella is the thickest in the human body, specifically adapted to withstand these extraordinary compressive loads.
The biomechanical consequences of removing the patella are profound and deleterious. Following total patellectomy, the kinematics of the knee joint are significantly altered. The most immediate effect is the decreased moment arm; the quadriceps tendon sits closer to the center of rotation, requiring substantially greater muscular force (up to 30% more) to achieve full active extension. Furthermore, the functional lengthening of the extensor mechanism following excision frequently results in an active extensor lag. Finally, the altered patellofemoral contact mechanics mean that the quadriceps tendon articulates directly with the trochlear groove. This non-anatomical friction inevitably leads to anterior knee pain, mechanical wear, and accelerated trochlear chondrosis over time. Recognizing these biomechanical deficits is crucial for executing surgical techniques that aim to shorten the mechanism and centralize the vector of pull.
Exhaustive Indications and Contraindications
The decision to perform a total patellectomy or to proceed with osteochondral fixation requires a rigorous assessment of the fracture pattern, patient physiology, and the viability of the remaining articular segments. Total patellectomy is strictly reserved as a salvage procedure. The primary objective is always osteosynthesis and preservation of the patella, utilizing tension band wiring, cannulated screw constructs, or partial patellectomy with tendon advancement. Partial patellectomy yields vastly superior biomechanical outcomes compared to total excision, preserving the moment arm and protecting the trochlear cartilage.
Total patellectomy is indicated primarily in scenarios of extreme trauma where comminution is so severe (stellate fractures with massive fragmentation) that no sizable, structurally viable fragments are salvageable for osteosynthesis. Specifically, if neither the proximal nor the distal pole retains at least one-third of the patellar articular surface, reconstruction is generally deemed impossible. Other rare indications include severe, recalcitrant patellofemoral osteoarthritis in low-demand, elderly patients where arthroplasty is contraindicated, or in cases of devastating localized osteomyelitis or primary malignant bone tumors of the patella.
The management of osteochondral fractures involves a different set of indications focused on biological preservation. Fixation is indicated for acute osteochondral fragments that are larger than 1 to 1.5 centimeters in diameter, particularly those located in critical weight-bearing zones of the femoral condyles or the primary articulating facets of the patella. The fragment must possess sufficient subchondral bone to allow for stable fixation. Conversely, immediate excision and marrow stimulation (microfracture) are indicated for small fragments (<1 cm), highly comminuted chondral shear injuries with no bone attached, or delayed presentations where the fragment has become rounded, fibrotic, and incongruous with the donor bed.
Contraindications to these procedures are equally critical to recognize. Total patellectomy is absolutely contraindicated if a viable proximal or distal pole can be retained and securely fixed to the remaining extensor mechanism. Performing a total patellectomy in a young, high-demand patient when a partial patellectomy was feasible is considered a significant surgical error. For osteochondral injuries, fixation is contraindicated in the presence of active intra-articular infection, severe degenerative joint disease, or when the fragment is chronically deformed. Attempting to force a malfitting, chronic osteochondral fragment into a rounded defect will result in an incongruous joint surface and rapid, localized osteoarthritis.
Indications and Contraindications Table
| Procedure | Primary Indications | Absolute/Relative Contraindications |
|---|---|---|
| Total Patellectomy | - Unsalvageable, severe stellate comminution - Lack of viable proximal/distal pole (>1/3rd size) - Devastating localized osteomyelitis - Primary malignant tumor of the patella |
- Salvageable proximal or distal pole (Partial Patellectomy preferred) - Young, high-demand athletes (relative) - Intact extensor mechanism with non-displaced fracture |
| Osteochondral Fixation | - Acute fragment >1.0 cm to 1.5 cm - Location in primary weight-bearing/articulating zone - Sufficient subchondral bone attached to cartilage - Acute presentation with congruous donor bed |
- Chronic, delayed presentation with rounded/fibrotic edges - Fragment <1.0 cm (excision preferred) - Pure chondral shear with no bone for fixation - Active intra-articular infection |
| Distal Femur Fixation (ORIF) | - Displaced intra-articular fractures (AO Types B, C) - Open fractures requiring debridement and stabilization - Polytrauma patients requiring early mobilization |
- Medically unstable patient unfit for anesthesia - Severe, active local infection (requires staging) - Non-ambulatory patient with minimal displacement |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the cornerstone of managing complex extensor mechanism and distal femoral injuries. The clinical evaluation must begin with a meticulous assessment of the soft tissue envelope. High-energy trauma frequently results in significant soft tissue compromise, including severe abrasions, fracture blisters, or Morel-Lavallée lesions (closed degloving injuries). The condition of the soft tissues dictates the timing of surgical intervention; operating through compromised, edematous skin drastically increases the risk of wound dehiscence and deep infection. In cases of severe swelling, surgery must be delayed, and the limb placed in a spanning external fixator or bulky Jones splint until the "wrinkle sign" appears, indicating the resolution of acute edema.
Radiographic evaluation requires standard anteroposterior (AP), lateral, and axial (sunrise or Merchant) views of the knee. However, plain radiographs consistently underestimate the degree of articular comminution and the exact size of osteochondral fragments. Therefore, a fine-cut Computed Tomography (CT) scan with 3D reconstructions is mandatory for all complex distal femoral fractures (AO Type B and C) and highly recommended for comminuted patellar fractures to assess for hidden osteochondral sheer lesions. The CT scan allows the surgeon to map the fracture lines, identify Hoffa fragments (coronal plane fractures of the femoral condyles), and plan the trajectory of fixation screws.
Pre-operative templating involves selecting the appropriate surgical approach, implants, and biological adjuncts. For a planned total patellectomy, the surgeon must ensure the availability of heavy, nonabsorbable sutures (e.g., #5 Ethibond or FiberWire) for the purse-string technique. If an osteochondral fracture is identified, bioabsorbable fixation materials, such as polydioxanone rods or absorbable sutures, must be available. For distal femoral fractures, templating involves selecting the appropriate length and contour of lateral locked plates, determining the need for medial column support, and sizing headless compression screws for articular reconstruction.
Patient positioning and operating room setup must be optimized to allow unhindered access to the knee and fluoroscopic visualization. The patient is placed supine on a radiolucent operating table. A small bump is placed under the ipsilateral hip to correct the natural external rotation of the lower extremity, ensuring the patella points directly toward the ceiling. A sterile tourniquet is applied to the proximal thigh to provide a bloodless surgical field, though it should be deflated prior to final closure to achieve meticulous hemostasis. The C-arm fluoroscopy unit is positioned on the contralateral side of the table, draped sterilely, and tested before the incision to ensure perfect AP and true lateral views of the knee joint can be obtained effortlessly throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of total patellectomy, osteochondral fixation, and distal femoral reconstruction demands precision, respect for soft tissue handling, and adherence to biomechanical principles. The exposure is typically achieved through a midline longitudinal incision, which provides extensile access to the extensor mechanism, the medial and lateral retinacula, and the distal femur. Full-thickness fasciocutaneous flaps are raised to preserve the precarious superficial blood supply.
Total Patellectomy: The Purse-String Rosette Technique
When total patellectomy is deemed unavoidable, the surgical technique must focus on shortening the extensor mechanism and creating a robust, centralized tendon repair to mitigate the inevitable biomechanical deficits. The retinaculum is carefully dissected, and all bony fragments of the comminuted patella are sharply excised. The crucial step here is to preserve as much of the patellar and quadriceps tendons as anatomically possible. The surgeon must meticulously shell the bone out of its tendinous envelope rather than resecting the tendon with the bone. Following excision, the joint undergoes exhaustive pulsatile lavage to clear all microscopic bone chips, marrow fat, and chondral debris, which could act as a nidus for third-body wear or loose body formation.
The core of the reconstruction is the purse-string suture technique. A heavy, nonabsorbable suture (such as #5 FiberWire) is passed through the margins of the patellar tendon, the quadriceps tendon, and the medial and lateral capsular expansions in a continuous, woven purse-string manner. The surgeon then pulls the suture taut, carefully evaginating the tendon ends completely outside the joint space. This evagination is critical to prevent intra-articular impingement of the bulky repair site during flexion. The suture is tightened until the tendinous margins form a tight, centralized circle approximately 2 mm in diameter, creating the "tendon rosette." This rosette provides centralized bulk, mimicking a small patella, and crucially centralizes the vector of the quadriceps pull to optimize tracking within the trochlear groove. Supplemental interrupted sutures are then placed to repair the retinacular tears and reinforce the rosette. If significant soft tissue loss prevents tension-free closure, the Shorbe and Dobson inverted V-plasty of the proximal quadriceps tendon is employed to lengthen the mechanism slightly while maintaining extensor continuity.
Management of Osteochondral Fractures: Pritsch Technique
For acute, salvageable osteochondral fractures, biological fixation is paramount. Modern investigation strongly supports the use of resorbable fixation devices over metallic implants to avoid a second operation for hardware removal and to eliminate the risk of severe chondral damage from migrating metal. The Pritsch absorbable suture technique is particularly effective for fragments consisting of large chondral surfaces attached to only thin slivers of subchondral bone, where rigid pins might cause catastrophic fragmentation.
The technique begins with meticulous anatomical reduction of the fragment into its donor bed. Using a small Kirschner wire (K-wire), three holes are drilled directly through the fragment and the remaining intact bone in a triangular configuration. Three heavy Vicryl sutures are then passed such that each suture traverses two holes, resulting in each drill hole containing two strands of suture material. This configuration distributes the compressive load evenly across the fragile fragment. The free ends of the sutures are tied securely over the anterior cortex of the bone, compressing the fragment into its bed without burying any hardware within the articular cartilage.
Distal Femoral Fractures: AO Principles and Fixation
Understanding the surrounding osseous anatomy and fracture patterns is critical when injuries extend into the distal femur. The surgical exposure often requires navigating complex neurovascular and muscular anatomy, particularly in the posterolateral corner.
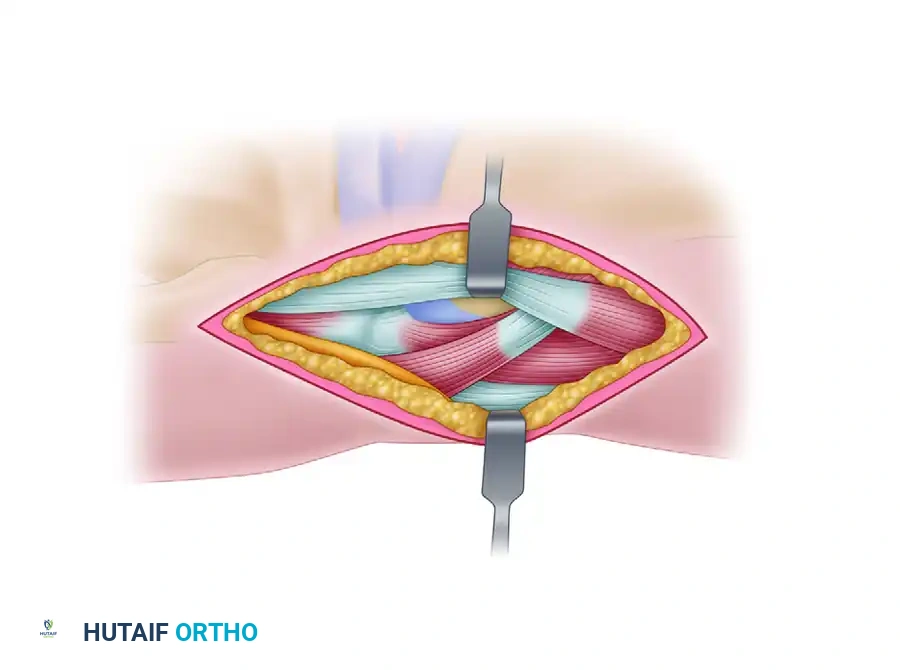
Anatomy and surgical exposure of the posterolateral knee, highlighting the Peroneal nerve, Gastrocnemius muscle, and Biceps femoris tendon. Careful dissection in this interval is critical when addressing posterior condylar or complex distal femoral injuries.
The AO/OTA classification dictates the operative strategy. For Type B3 (Hoffa) fractures, anatomical reduction and absolute stability are required. This is achieved using anterior-to-posterior or posterior-to-anterior headless compression screws, ensuring the threads do not cross the fracture site to allow for dynamic interfragmentary compression.

Intraoperative posteroanterior radiograph demonstrating precise lag screw fixation of a distal femoral condylar fracture, achieving absolute stability of the articular block.
For Type C (complete articular) fractures, the articular block must first be reconstructed anatomically and converted into a Type A (extra-articular) fracture. Once the joint surface is perfectly restored and temporarily held with K-wires, definitive fixation is achieved using a pre-contoured, lateral distal femoral locking plate. The plate is applied using minimally invasive submuscular sliding techniques to preserve the periosteal blood supply to the metaphyseal comminution.

Lateral radiograph confirming the trajectory of the fixation screws, ensuring they do not breach the articular surface or the intercondylar notch.
Complications, Incidence Rates, and Salvage Management
The operative management of complex extensor mechanism and distal femoral injuries is fraught with potential complications, demanding vigilant post-operative monitoring and a deep understanding of salvage pathways. Following total patellectomy, the most ubiquitous complication is an active extensor lag, occurring in up to 60-80% of patients. This results directly from the functional lengthening of the extensor mechanism and the loss of the patellar moment arm. While aggressive closed-chain rehabilitation is the primary treatment, severe, debilitating lags may rarely necessitate a secondary surgical procedure, such as a distal advancement of the tibial tubercle or a proximal quadriceps shortening, though these carry significant morbidity.
Anterior knee pain and accelerated trochlear chondrosis are virtually inevitable long-term sequelae of total patellectomy. The direct articulation of the tendinous repair against the articular cartilage of the trochlear groove creates abnormal shear forces and friction. Over a period of 5 to 15 years, this leads to profound mechanical wear. Management is largely conservative, relying on activity modification, NSAIDs, and intra-articular corticosteroid or hyaluronic acid injections. In end-stage cases, total knee arthroplasty may be considered, though the outcomes are historically less favorable in post-patellectomy patients due to extensor mechanism insufficiency.
Complications following osteochondral fracture fixation include nonunion, fragment necrosis, and hardware irritation. If a bioabsorbable pin or suture fails to maintain compression, the fragment may displace, acting as a loose body and causing acute mechanical locking of the joint. Salvage management for failed osteochondral fixation requires immediate arthroscopic or open removal of the loose fragment. The remaining defect is then managed based on its size and location; small defects (<2 cm²) are treated with marrow stimulation (microfracture) to induce a fibrocartilage healing response, while larger defects in young patients may require Osteochondral Autograft Transfer System (OATS) procedures or Autologous Chondrocyte Implantation (ACI).
Infection and wound breakdown remain catastrophic complications, particularly in high-energy open fractures or patients with compromised soft tissue envelopes. Deep surgical site infections require aggressive, immediate intervention, including serial operative debridements, copious pulsatile lavage, and targeted intravenous antibiotic therapy based on intra-operative cultures. If internal fixation hardware is present, its retention depends on the stability of the construct and the virulence of the organism; unstable hardware must be removed and replaced with external fixation.
Complications and Salvage Management Table
| Complication | Estimated Incidence | Pathophysiology/Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Extensor Lag | 60% - 80% (Post-Patellectomy) | Loss of moment arm, functional lengthening of extensor mechanism. | Aggressive closed-chain rehab; rarely surgical shortening or tibial tubercle advancement. |
| Trochlear Chondrosis | >85% at 10 years | Direct friction of tendon on trochlear cartilage. | NSAIDs, injections, activity modification; Total Knee Arthroplasty for end-stage disease. |
| Osteochondral Nonunion | 10% - 20% | Inadequate fixation, avascularity of fragment, premature weight-bearing. | Excision of loose body; microfracture, OATS, or ACI depending on defect size/patient age. |
| Deep Joint Infection | 2% - 5% (Higher in open trauma) | High-energy injury, compromised soft tissue, prolonged operative time. | Serial I&D, IV antibiotics, removal of unstable hardware, possible flap coverage. |
Phased Post-Operative Rehabilitation Protocols
The success of both total patellectomy and osteochondral fixation relies heavily on strict adherence to phased, biologically sound post-operative rehabilitation protocols. The rehabilitation strategy must navigate the delicate balance between protecting the fragile surgical repair from excessive tension or shear forces and preventing debilitating arthrofibrosis and joint stiffness. The timeline is dictated by the biological healing rates of tendon-to-tendon repair (in patellectomy) versus osteochondral integration.
Phase I: Maximum Protection (Weeks 0-4)
Immediately following total patellectomy, the knee is immobilized in full extension using a rigid cylinder cast or a locked hinged knee brace. This position minimizes tension on the purse-string rosette repair and the retinacular closures. Weight-bearing is typically allowed as tolerated with the knee securely locked in extension. Isometric quadriceps sets, straight leg raises, and ankle pumps are initiated immediately to prevent muscle atrophy and mitigate deep vein thrombosis risk. For patients who underwent osteochondral fracture fixation or complex distal femoral plating, weight-bearing is strictly prohibited (non-weight-bearing status) to protect the articular reconstruction, though continuous passive motion (CPM) may be utilized to nourish the cartilage if the fixation is deemed absolutely stable.
Phase II: Controlled Mobilization (Weeks 4-8)
At the four-week mark, early biological healing allows for controlled mobilization. The hinged knee brace is unlocked to allow progressive, passive, and active-assisted flexion. The typical progression aims for 0 to 30 degrees initially, advancing by 15 degrees weekly. Active extension is strictly avoided during this phase to prevent stretching or rupturing the healing tendon rosette. For osteochondral repairs, CPM continues, and touch-down weight-bearing may be initiated based on radiographic evidence of integration. The primary goal of this phase is to restore joint kinematics and prevent capsular contracture without jeopardizing the structural integrity of the repair.
Phase III: Strengthening and Functional Return (Weeks 8-12+)
By the eighth week, the brace is gradually weaned, and the focus shifts entirely to progressive resistance exercises and overcoming the inevitable extensor lag associated with patellectomy. Aggressive closed-chain quadriceps strengthening exercises, such as mini-squats and leg presses, are introduced. Open-chain extension exercises are added cautiously. For distal femoral and osteochondral fractures, weight-bearing is progressed to full as tolerated, guided by clinical and radiographic healing. Return to high-impact activities or heavy labor is generally delayed until 6 to 9 months post-operatively, contingent upon the recovery of at least 85% of the contralateral limb's quadriceps strength and the absence of mechanical symptoms.
Summary of Landmark Literature and Clinical Guidelines
The operative principles governing the management of extensor mechanism and distal femoral injuries are deeply rooted in decades of evolving biomechanical research and clinical outcome studies. A thorough understanding of this landmark literature is essential for the academic orthopedic surgeon to justify treatment algorithms and anticipate prognostic outcomes.
The historical
