Introduction to Extensor Mechanism and Articular Knee Injuries
The management of complex fractures involving the extensor mechanism and the distal femoral articular surface presents a formidable challenge to the orthopedic surgeon. When high-energy trauma results in catastrophic comminution of the patella, or when shearing forces create displaced osteochondral fragments within the knee joint, meticulous surgical decision-making is paramount. This comprehensive guide delineates the indications, biomechanical considerations, and precise surgical techniques for total patellectomy, the fixation of osteochondral fractures, and the classification-driven management of distal femoral fractures.
Total Patellectomy
The patella serves as a critical biomechanical fulcrum, increasing the moment arm of the quadriceps mechanism and enhancing knee extension torque by up to 30%. Consequently, preservation of the patella is always the primary objective. However, in scenarios of extreme trauma, preservation may be impossible.
Indications and Patient Selection
Total patellectomy is strictly reserved as a salvage procedure. It is indicated primarily in fractures where comminution is so severe that no sizable, structurally viable fragments are salvageable for osteosynthesis.
⚠️ Surgical Warning
Never perform a total patellectomy if a viable proximal or distal pole can be retained. Partial patellectomy with tendon advancement yields vastly superior biomechanical outcomes compared to total excision. Total patellectomy inevitably results in a permanent reduction in quadriceps strength and a high risk of extensor lag.
Biomechanical Consequences
Removal of the patella alters the kinematics of the knee joint significantly:
* Decreased Moment Arm: The quadriceps tendon sits closer to the center of rotation of the knee, requiring greater force to achieve full extension.
* Extensor Lag: Due to the functional lengthening of the extensor mechanism following excision, patients frequently develop an active extensor lag.
* Altered Patellofemoral Contact: The tendon directly articulates with the trochlear groove, which can lead to anterior knee pain and accelerated trochlear chondrosis over time.
To mitigate these consequences, the surgical technique must focus on shortening the extensor mechanism and creating a robust, centralized tendon repair.
Surgical Technique: Total Patellectomy
The following technique emphasizes the preservation of tendinous tissue and the creation of a centralized "rosette" to mimic the patellar bulk and optimize tracking.
Step 1: Exposure and Fragment Excision
* Utilize a midline longitudinal or standard anterior parapatellar incision.
* Carefully dissect the retinaculum. Excise all bony fragments of the comminuted patella sharply.
* Crucial Step: Preserve as much of the patellar and quadriceps tendons as anatomically possible. Shell the bone out of its tendinous envelope rather than resecting the tendon with the bone.
Step 2: Joint Debridement
* Clear the joint of all microscopic bone chips, marrow fat, and chondral debris through exhaustive pulsatile lavage and thorough manual inspection of the gutters and intercondylar notch.
Step 3: The Purse-String Suture Technique
* Place a heavy, nonabsorbable suture (e.g., #5 Ethibond or FiberWire) through the margins of the patellar tendon, the quadriceps tendon, and through the medial and lateral capsular expansions.
* This suture must be woven in a continuous purse-string manner.
Step 4: Tendon Evagination and Knot Tying
* Pull the purse-string suture taut.
* Evaginate the tendon ends completely outside the joint space to prevent intra-articular impingement of the repair site.
* Tighten the suture until the tendinous margins form a tight circle approximately 2 mm in diameter, then tie it securely.
💡 Clinical Pearl: The Tendon Rosette
Although small, this evaginated rosette of tendon provides a centralized bulk that gives the clinical appearance of a small patella. More importantly, it centralizes the vector of the quadriceps pull, improving tracking within the trochlear groove.
Step 5: Supplemental Repair and Retinacular Closure
* Use supplemental interrupted sutures (e.g., #2 or #1 nonabsorbable) to repair the medial and lateral capsular ruptures (retinaculum).
* Appose the quadriceps and patellar tendon ends further to reinforce the rosette.
* The purse-string technique inherently shortens the quadriceps mechanism, which is a vital biomechanical step to help prevent the extensor lag that is notoriously common after patellectomy.
Step 6: Management of Insufficient Tendon (Inverted V-Plasty)
* If the trauma has resulted in significant soft tissue loss and insufficient tendon is available to suture the quadriceps and patellar tendons primarily without excessive tension, a quadriceps tie-down technique must be employed.
* Shorbe and Dobson Technique: An inverted V-plasty of the proximal quadriceps tendon can be utilized to lengthen the mechanism slightly, allowing for a tension-free closure at the joint line while maintaining overall extensor continuity.
Management of Osteochondral Fractures
Osteochondral fractures of the patella or distal femur frequently accompany patellar dislocations or direct high-energy shear trauma. The management algorithm dictates that these fragments should be fixed if they are large and located in weight-bearing or critical articulation zones.
Fixation Strategies and Materials
Historically, metallic implants were used, but they required subsequent removal and risked severe chondral damage if they migrated. Modern investigation into resorbable fixation devices has produced robust clinical and experimental evidence supporting their use.
- Resorbable Polydioxanone Rods: These provide satisfactory, low-profile fixation of osteochondral fractures without the need for a second operation for hardware removal.
- Absorbable Suture Fixation (Pritsch et al. Technique): This technique is specifically proposed for osteochondral fractures of the patella that consist of large chondral fragments attached to only thin slivers of subchondral bone, where pins or screws might cause fragmentation.
Surgical Technique: Pritsch Absorbable Suture Fixation
- Reduction: The osteochondral fragment is anatomically reduced into its donor bed.
- Drilling: Three holes are drilled using a small Kirschner wire (K-wire). These holes pass directly through the fragment and the remaining patella in a triangular configuration.
- Suture Passage: Three Vicryl sutures (Ethicon, Johnson & Johnson, Somerville, NJ) are utilized. They are placed so that each suture passes through two holes. Consequently, each drill hole contains two strands of suture material, distributing the load evenly.
- Securing: The free ends of the sutures are tied over the anterior border of the patella, compressing the fragment securely into its bed without burying hardware in the articular cartilage.
Management of Delayed Presentations
If the diagnosis and subsequent surgery are delayed, the pathoanatomy of the fracture changes. The edges of the osteochondral fragment and the recipient defect become rounded, covered with fibrous tissue, and exact anatomical fitting becomes impossible.
⚠️ Surgical Pitfall: Delayed Osteochondral Fragments
Do not attempt to force a malfitting, chronic osteochondral fragment into a rounded defect. This will result in an incongruous joint surface and rapid localized osteoarthritis.
Salvage Technique for Delayed Fragments:
* The fragment should be completely excised.
* The cancellous bed where the fragment originated must be smoothed and debrided to bleeding bone to stimulate a fibrocartilage healing response (microfracture principles).
* Any detached or frayed edges of the surrounding healthy cartilage should be excised sharply and vertically. They must not be beveled or shaved down, as vertical walls provide better containment for the forming fibrocartilage clot.
* If the involved area is small and does not involve a primary weight-bearing surface, excision usually results in little, if any, long-term functional disability.
Distal Femoral Fractures: Classification and Operative Principles
Understanding the surrounding osseous anatomy and fracture patterns is critical, especially when osteochondral injuries extend into the distal femur. The surgical exposure often requires navigating complex neurovascular and muscular anatomy.
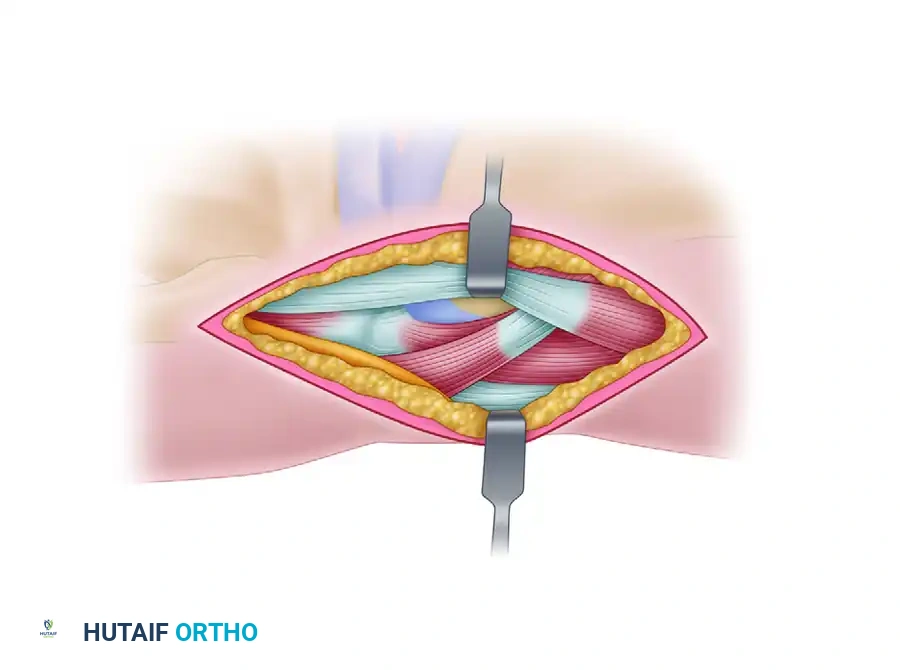
Anatomy and surgical exposure of the posterolateral knee, highlighting the Peroneal nerve, Gastrocnemius muscle, and Biceps femoris tendon. Careful dissection in this interval is critical when addressing posterior condylar or complex distal femoral injuries.
The AO/OTA Classification System
The classification of distal femoral fractures originally described by Müller et al., and subsequently expanded into the comprehensive AO/OTA classification, is the gold standard for determining treatment algorithms and prognosis. It evaluates all fractures within the transepicondylar width of the knee.
- Type A (Extra-articular): Involve the distal femoral shaft only, with varying degrees of comminution, sparing the joint surface.
- Type B (Partial Articular / Condylar):
- Type B1: Sagittal split of the lateral condyle.
- Type B2: Sagittal split of the medial condyle.
- Type B3: Coronal plane fracture (Hoffa fracture), which is highly unstable and requires anterior-to-posterior or posterior-to-anterior lag screw fixation.
- Type C (Complete Articular): T-condylar and Y-condylar fractures where the articular surface is dissociated from the diaphysis.
- Type C1: Articular simple, metaphyseal simple.
- Type C2: Articular simple, metaphyseal comminuted.
- Type C3: Intra-articular comminution (the most challenging to reconstruct).
Evolution of Treatment Modalities
In the 1960s, nonoperative treatment methods, such as skeletal traction and cast bracing, paradoxically produced better results than operative treatment. This was primarily due to the lack of adequate internal fixation devices, leading to catastrophic hardware failures and infections.
With the development of improved internal fixation devices and biological plating principles by the AO group, treatment recommendations shifted dramatically. Today, operative treatment produces vastly superior results compared to nonoperative management, especially for intercondylar and extra-articular fractures.

Intraoperative posteroanterior radiograph demonstrating precise lag screw fixation of a distal femoral condylar fracture, achieving absolute stability of the articular block.

Lateral radiograph confirming the trajectory of the fixation screws, ensuring they do not breach the articular surface or the intercondylar notch.
While intra-articular fractures (Type C3) historically had more unsatisfactory results overall regardless of modality, modern locked plating and headless compression screws have equalized or surpassed historical nonoperative outcomes by allowing early range of motion and preventing joint stiffness.
Postoperative Rehabilitation Protocols
The success of both total patellectomy and osteochondral fixation relies heavily on strict adherence to postoperative rehabilitation phases.
Following Total Patellectomy
- Phase I (0-4 Weeks): The knee is immobilized in full extension in a cylinder cast or locked hinged knee brace. Weight-bearing is typically allowed as tolerated with the knee locked in extension to protect the retinacular and tendon repair. Isometric quadriceps sets are initiated immediately.
- Phase II (4-8 Weeks): The brace is unlocked to allow progressive, controlled flexion (e.g., 0-30 degrees, advancing 15 degrees weekly). Active extension is avoided to prevent stretching the rosette repair.
- Phase III (8+ Weeks): Progressive resistance exercises are introduced. The primary goal is overcoming the inevitable extensor lag through aggressive closed-chain quadriceps strengthening.
Following Osteochondral Fracture Fixation
Postoperative care for surgically fixed osteochondral fractures is dictated by the security of the fixation and the anatomical location of the lesion.
* Immobilization: Consists of 3 to 6 weeks of immobilization or highly restricted range of motion, often utilizing continuous passive motion (CPM) machines to nourish the cartilage without applying shear stress.
* Weight-Bearing: Requires 6 to 12 weeks of strictly protected (touch-down or non-weight-bearing) status. Weight-bearing is delayed longer for lesions on the weight-bearing axis of the femoral condyles compared to patellar lesions.
Conclusion
Total patellectomy, while a procedure of last resort, requires exacting surgical technique to optimize the remaining extensor mechanism. The purse-string rosette technique provides the best biomechanical compromise when the patella cannot be salvaged. Concurrently, the management of associated osteochondral and distal femoral fractures demands a deep understanding of AO principles, utilizing modern absorbable sutures, resorbable pins, and rigid internal fixation to restore joint congruity and allow for early, safe rehabilitation.
