Comprehensive Introduction and Patho-Epidemiology
The tibial nerve represents the larger, medial, and biomechanically dominant division of the sciatic nerve. Composed of ventral rami fibers from the L4, L5, S1, S2, and S3 nerve roots, it is fundamentally responsible for the motor innervation of the entire posterior compartment of the leg, as well as the intricate intrinsic musculature of the plantar foot. Furthermore, it provides critical sensory feedback to the plantar aspect of the foot, a function that is absolutely paramount for normal human gait, weight-bearing mechanics, proprioception, and the prevention of devastating neurotrophic ulceration. The biomechanical contribution of the tibial nerve cannot be overstated; it powers the triceps surae complex, which is the primary generator of the propulsive push-off phase during the terminal stance of the gait cycle.
Injuries to the tibial nerve, whether sustained through high-energy blunt trauma, penetrating injuries, complex knee dislocations, or iatrogenic transection, result in profound and often permanent functional deficits. The epidemiological profile of tibial nerve injuries is diverse. While less frequently injured than its lateral counterpart, the common peroneal nerve, during multiligamentous knee injuries, the tibial nerve is highly susceptible to penetrating trauma in the popliteal fossa, severe crush injuries of the lower leg, and iatrogenic damage during complex orthopedic and vascular procedures. Iatrogenic etiologies include aggressive retraction during proximal tibial osteotomies, blind passage of instruments during meniscal repairs, complicated Baker’s cyst excisions, and posterior approaches to the tibial plateau.
The pathophysiological cascade following a complete transection (neurotmesis) or severe crush (axonotmesis) involves Wallerian degeneration distal to the zone of injury. The loss of plantar flexion severely impairs the push-off phase, resulting in a highly inefficient, energy-consuming calcaneal gait pattern. More insidiously, the loss of plantar sensation frequently leads to unrecognized microtrauma. Without protective nociception and proprioception, patients are at an exceptionally high risk of developing chronic plantar ulcerations, deep soft-tissue infections, osteomyelitis, and eventually, Charcot neuroarthropathy. Consequently, the surgical management of tibial nerve lesions demands a rigorous understanding of its topographical anatomy, precise clinical evaluation, and absolute mastery of advanced microsurgical repair techniques.
The overarching goal of tibial nerve reconstruction is twofold: the restoration of protective plantar sensation to prevent limb-threatening complications, and the reinnervation of the posterior compartment musculature to restore dynamic ankle plantar flexion. Given the considerable distance between the popliteal fossa and the intrinsic muscles of the foot, motor recovery of the foot intrinsics is exceedingly rare following proximal injuries, even with optimal microsurgical repair. Therefore, the surgeon must set realistic expectations, focusing primarily on proximal motor recovery (gastrocnemius and soleus) and distal sensory restoration.
Detailed Surgical Anatomy and Biomechanics
Proximal Course and the Popliteal Fossa
The tibial nerve formally begins its independent anatomical course in the distal third of the posterior thigh, just proximal to the apex of the popliteal fossa. This marks the anatomical bifurcation of the sciatic nerve, where the common peroneal nerve diverges laterally to follow the medial border of the biceps femoris. The tibial nerve continues a direct, linear trajectory distally, bisecting the popliteal fossa longitudinally. It is enveloped within a distinct epineurial sheath, which provides a degree of structural integrity and protection against longitudinal traction.
As it courses through the popliteal fossa, the tibial nerve maintains a highly predictable, albeit vulnerable, relationship with the major regional vascular structures. It lies superficial (posterior) and slightly lateral to the popliteal vein and artery, making it the most accessible and first-encountered major neurovascular structure when approaching the posterior knee. Before passing deep to the tendinous arch of the soleus muscle, the tibial nerve yields several critical motor branches. These branches typically arise from the posterior and lateral aspects of the main trunk and supply the plantaris, soleus, popliteus, and the medial and lateral heads of the gastrocnemius.
The branching pattern within the popliteal fossa is notoriously variable and presents a significant hazard during surgical exploration. The branches to the gastrocnemius and soleus often arise as a common trunk or are tethered closely to the main tibial nerve by dense connective tissue. Aggressive retraction or blind dissection in this area, without prior meticulous intraneural neurolysis, can easily result in the avulsion of these proximal motor branches. Furthermore, the medial sural cutaneous nerve arises from the tibial nerve in this region, descending between the two heads of the gastrocnemius to eventually join the sural communicating branch from the common peroneal nerve, forming the definitive sural nerve.
Deep Compartment Transit and Terminal Branching
After exiting the popliteal fossa, the tibial nerve dives beneath the dense, fibrous tendinous arch of the soleus muscle, transitioning into the deep posterior compartment of the leg. This anatomical bottleneck is a potential site for entrapment, particularly following severe tibial fractures or compartment syndrome. Within the deep posterior compartment, the nerve travels alongside the posterior tibial vessels, resting directly on the posterior surface of the tibialis posterior muscle.
In this deep segment, the tibial nerve provides sequential motor branches to the deep flexor group: the tibialis posterior, the flexor digitorum longus (FDL), and the flexor hallucis longus (FHL). The topographical arrangement of fascicles within the nerve trunk at this level is highly organized, with motor fascicles destined for specific muscles grouping together well before they physically branch from the main epineurial sheath. This internal topography is a critical consideration when performing interfascicular grafting or nerve transfers.
As the nerve approaches the ankle, it becomes superficial once again, entering the fibro-osseous tarsal tunnel posterior to the medial malleolus. Here, it is constrained by the flexor retinaculum. Within or just distal to the tarsal tunnel, the tibial nerve bifurcates into its terminal branches: the medial plantar nerve, the lateral plantar nerve, and the medial calcaneal nerve. These terminal branches are exclusively responsible for the complex motor function of the intrinsic foot muscles and the vital sensory innervation of the plantar weight-bearing surfaces.
Exhaustive Indications and Contraindications
The decision-making process regarding the surgical exploration and repair of the tibial nerve requires a meticulous synthesis of the mechanism of injury, the timing of presentation, the patient's overall physiological status, and the condition of the surrounding soft tissue envelope. Surgical intervention is not universally indicated, and inappropriate timing or patient selection can lead to catastrophic outcomes, including severe infection or limb loss.
Primary repair is strictly indicated for acute, sharp transections (e.g., knife wounds, glass lacerations) where the zone of injury is highly localized, and the nerve ends can be coapted without tension. In these scenarios, immediate exploration within the first 72 hours allows for direct end-to-end neurorrhaphy before the distal stump undergoes significant retraction and before the fascicular architecture becomes obscured by fibrotic scar tissue. Conversely, blunt trauma, severe crush injuries, and avulsions dictate a delayed approach. In these high-energy mechanisms, the exact longitudinal extent of intraneural damage (the "zone of injury") is impossible to determine acutely.
Delayed reconstruction, typically performed 3 to 4 weeks post-injury, allows for the demarcation of viable and non-viable nerve tissue. By this time, the epineurium has thickened, holding sutures more securely, and the surgeon can accurately resect the damaged nerve ends back to healthy, pouting fascicles ("bread-loafing" technique) prior to grafting. Contraindications are equally critical to recognize. Severe physiological instability, active deep space infections, and massive soft tissue defects lacking adequate vascularized coverage absolutely preclude complex peripheral nerve reconstruction.
| Clinical Scenario / Factor | Indications for Surgical Intervention | Absolute or Relative Contraindications |
|---|---|---|
| Mechanism of Injury | Sharp, clean lacerations (Primary); High-energy crush/avulsion with documented lack of recovery at 3-6 months (Delayed). | Severe crush injury with an unsalvageable limb requiring primary amputation. |
| Timing | Acute (<72 hours) for sharp cuts; Subacute (3-4 weeks) for blunt trauma demarcation; Chronic (up to 12-18 months) for grafting. | Chronic injuries >18-24 months where irreversible motor endplate degradation has occurred (Relative). |
| Soft Tissue Envelope | Clean wound bed, adequate vascularized tissue coverage, absence of active infection. | Active purulence, massive soft tissue loss requiring free flap coverage before nerve repair can be considered. |
| Neurological Status | Complete loss of motor/sensory function (Neurotmesis) confirmed by serial exams and EMG/NCS. | Documented clinical or electromyographic signs of progressive spontaneous recovery (Neurapraxia/Axonotmesis). |
| Patient Factors | Medically optimized, compliant with rigid post-operative immobilization and long-term rehabilitation. | Severe systemic instability, profound peripheral vascular disease preventing healing, non-compliance. |
Pre-Operative Planning, Templating, and Patient Positioning
Accurate clinical evaluation of the tibial nerve requires isolating the specific muscles it innervates and meticulously mapping its autonomous sensory zones. The muscles supplied by the tibial nerve proximal to the soleus arch (gastrocnemius, soleus) are tested via active ankle plantar flexion against resistance. However, evaluating the deep flexors requires nuanced palpation. The Flexor Hallucis Longus (FHL) tendon is readily palpable posterior to the medial malleolus during active great toe flexion. The Tibialis Posterior is tested by assessing active foot inversion in a plantar-flexed position. The autonomous sensory zone encompasses the sole of the foot, the lateral heel, and the plantar toes.
Advanced diagnostic modalities are indispensable for operative planning. Because the tibial nerve lies deep within the adipose tissue of the popliteal fossa, transcutaneous electrical stimulation is notoriously unreliable. Electromyography (EMG) and Nerve Conduction Studies (NCS) are strictly indicated to differentiate between complete axonotmesis/neurotmesis and neurapraxia. A baseline EMG at 3 to 4 weeks post-injury is critical to detect fibrillation potentials and positive sharp waves, confirming denervation. High-Resolution Ultrasound (HRUS) and Magnetic Resonance Neurography (MRN) have revolutionized pre-operative templating. These imaging modalities can precisely localize the level of transection, quantify the length of the nerve gap, and identify neuromas-in-continuity, allowing the surgeon to anticipate the need for autograft harvesting.
Patient positioning is a critical component of the surgical setup. The patient is placed in the prone position on a radiolucent Jackson table or standard operating table with chest and pelvic rolls to ensure adequate pulmonary excursion and avoid abdominal venous compression. All bony prominences, particularly the patellae and anterior superior iliac spines, are heavily padded. The operative limb is prepped and draped circumferentially from the gluteal fold to the toes to allow for dynamic intraoperative manipulation of the knee and ankle joints.
A pneumatic tourniquet is applied to the proximal thigh to ensure a completely bloodless surgical field, which is absolutely critical for identifying delicate fascicular structures, performing microvascular hemostasis, and avoiding catastrophic injury to the popliteal vessels. The tourniquet time must be strictly monitored, not exceeding 120 minutes, to prevent ischemic reperfusion injury to the already compromised distal musculature. Furthermore, the contralateral lower extremity should be prepped and draped into the sterile field to facilitate the harvest of the contralateral sural nerve, should an extensive autogenous interfascicular cable graft be required.
Step-by-Step Surgical Approach and Fixation Technique
Incision Design and The Mayfield Approach
Exposure of the tibial nerve in the popliteal fossa is a technically demanding procedure indicated for the exploration of penetrating trauma, complex tumor resection, or the repair of severe nerve lacerations. The approach must be meticulously planned to avoid debilitating postoperative contractures. The skin of the popliteal fossa is subject to constant dynamic tension during knee flexion and extension. A fundamental surgical pitfall is the utilization of a straight longitudinal incision directly across the popliteal crease. A perpendicular incision across these dynamic skin folds will inevitably lead to severe hypertrophic scarring, rigid flexion contractures of the knee, and potential skin ulceration upon extension.

To mitigate this, the surgeon must utilize the Mayfield incision or a geometrically precise curvilinear "S" shaped incision. The incision begins proximally on the posterior thigh, curving gently laterally or medially as it approaches the popliteal crease. It must traverse the popliteal crease obliquely or transversely, strictly following the resting skin tension lines. If necessary, the skin incision is extended distally along the medial side of the hamstring tendons, continuing onto the leg just posterior to the medial border of the tibia.

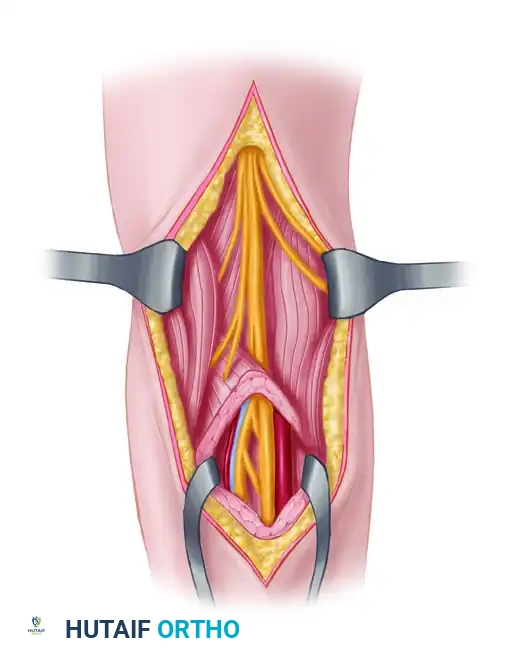
Deep Dissection and Gap Management
The deep dissection begins by dividing the superficial fascia in line with the skin incision. The lesser saphenous vein and the medial sural cutaneous nerve serve as reliable anatomical landmarks; they are identified superficially and traced proximally to locate the main trunk of the tibial nerve. The hamstring muscles (semimembranosus and semitendinosus medially; biceps femoris laterally) are mobilized and retracted to expose the proximal apex of the fossa. The tibial nerve is identified superficially, while the popliteal artery and vein lie deep and slightly medial. The nerve is traced distally, requiring meticulous microdissection to preserve the highly variable motor branches to the gastrocnemius and soleus.
The primary challenge in peripheral nerve surgery is achieving a completely tension-free neurorrhaphy. When a segment of the tibial nerve is destroyed, closing the resulting gap requires a strategic combination of mobilization, joint positioning, and occasionally, nerve transposition. Extensive exposure is mandatory; mobilizing the proximal part of the tibial nerve high into the posterior thigh is almost always necessary. All muscular branches must be stripped back intraneurally for several centimeters. This careful microdissection separates the fascicles supplying the muscles from the main trunk, allowing the main trunk to advance distally without tethering the proximal muscle bellies.
Transposition and Microsurgical Repair
Manipulating the joints can provide significant nerve excursion. Flexing the knee to 90 degrees is the most effective method for gaining length, allowing for the closure of a gap of up to 10 cm. However, plantar flexing the ankle to gain distal length is strictly contraindicated, as it frequently leads to a rigid, disabling equinus contracture. Occasionally, the tibial nerve can be transposed either between the soleus and the gastrocnemius, or superficial to both, to gain additional length. If the soleus is detached for transposition, it must be securely sutured back to its origin before the neurorrhaphy is performed.
When the gap is too large to be closed by mobilization and knee flexion, autogenous interfascicular grafting is the absolute gold standard. The sural nerve is harvested and cut into appropriate lengths to form a cable graft. Under operating microscope magnification, the damaged nerve ends are serially resected ("bread-loafed") until healthy, unscarred fascicles pout from the epineurium. The sural nerve cables are interposed to match the cross-sectional fascicular topography of the proximal and distal stumps. Coaptation is achieved using 9-0 or 10-0 monofilament nylon sutures placed strictly through the epineurium, often augmented with fibrin tissue adhesive to ensure a watertight, tension-free construct.
Complications, Incidence Rates, and Salvage Management
The surgical management of tibial nerve injuries is fraught with potential complications, ranging from technical failures of the repair to profound physiological consequences of prolonged denervation. The most devastating complication is the complete failure of nerve regeneration, which can occur despite a technically flawless microsurgical repair. This is particularly common in delayed repairs, massive crush injuries with extensive zones of trauma, or when excessively long interpositional cable grafts (>10-12 cm) are utilized.
Another frequent and highly problematic complication is the formation of a symptomatic neuroma-in-continuity or a terminal neuroma at the repair site. This occurs when regenerating axonal sprouts escape the epineurial repair site and proliferate haphazardly into the surrounding fibrotic scar tissue. Patients present with exquisite, localized point tenderness, a strongly positive Tinel’s sign that does not advance distally over time, and severe neuropathic pain that is often refractory to standard pharmacological management. Surgical exploration, neuroma excision, and revision grafting or targeted muscle reinnervation (TMR) may be required for salvage.
Joint contractures represent a massive iatrogenic risk, directly related to the techniques used for gap closure and post-operative immobilization. If the knee was flexed to 90 degrees to facilitate a primary repair, the patient is at a high risk of developing a rigid flexion contracture of the knee. Even more disastrous is the equinus contracture of the ankle, which occurs if the surgeon inappropriately utilizes extreme plantar flexion to gain distal nerve length. An equinus deformity severely impairs the stance phase of gait and creates abnormal pressure distributions on the insensate plantar forefoot, rapidly accelerating the development of neurotrophic ulcerations.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Prevention |
|---|---|---|---|
| Failure of Regeneration | 15 - 30% (Higher in long grafts) | Extensive zone of injury, delayed repair >6 months, graft length >10cm, advanced patient age. | Prevention: Tension-free repair, healthy fascicles. Salvage: Ankle-Foot Orthosis (AFO), Pantalar arthrodesis for stability. |
| Neuroma Formation | 10 - 20% | Escaped axonal sprouts, repair under tension, inadequate resection of fibrotic nerve ends. | Excision of neuroma, revision grafting, burying nerve stump in muscle, or Targeted Muscle Reinnervation (TMR). |
| Knee Flexion Contracture | 5 - 15% | Prolonged immobilization in >60 degrees of flexion, failure to adhere to gradual extension protocols. | Prevention: Limit intra-op flexion, strict hinged brace protocol. Salvage: Serial casting, surgical posterior capsular release. |
| Equinus Ankle Contracture | High if positioned poorly | Utilizing extreme ankle plantar flexion to gain distal nerve length during surgery. | Prevention: NEVER plantar flex the ankle to close a nerve gap. Salvage: Achilles tendon lengthening (Z-plasty), rigid AFO. |
| Neurotrophic Ulceration | 20 - 40% (Long-term) | Loss of protective plantar sensation combined with altered foot biomechanics and unrecognized microtrauma. | Aggressive daily foot inspection, custom offloading orthotics, total contact casting for active ulcers, Charcot reconstruction. |
Phased Post-Operative Rehabilitation Protocols
The post-operative management of a tibial nerve repair is highly specialized and is strictly dictated by the surgical methods utilized to achieve a tension-free closure. The rehabilitation protocol must balance the critical need to protect the delicate microsurgical neurorrhaphy from tensile disruption with the imperative to prevent rigid joint contractures and maintain the viability of the denervated distal musculature.
Phase 1: Strict Immobilization (Weeks 0 to 4)
If knee flexion was utilized to close a nerve gap, the limb is immediately immobilized in the operating room in a well-padded, long-leg cast or a rigid, locked hinged knee brace. The knee is locked in the exact degree of flexion required to maintain zero tension on the repair (up to, but ideally not exceeding, 90 degrees). Crucially, the ankle must be maintained in a strictly neutral position (0 degrees of dorsiflexion/plantarflexion) to prevent the devastating complication of an equinus contracture. This rigid immobilization is maintained continuously for 3 to 4 weeks. This duration allows the epineurial repair site to undergo initial fibroblastic healing, acquiring sufficient tensile strength to withstand gradual mobilization.
Phase 2: Gradual Extension and Mobilization (Weeks 4 to 8)
After the initial 4-week immobilization period, the process of gradual knee extension begins. This is a highly controlled phase, usually accomplished by adjusting the locking mechanism of the hinged knee brace. The knee is permitted to extend by an increment of exactly 10 to 15 degrees per week. Rapid or uncontrolled extension is strictly prohibited, as it will cause catastrophic longitudinal traction injury to the newly repaired nerve, potentially rupturing the coaptation or inducing severe intraneural ischemia. During this phase, passive range of motion of the ankle and digits is initiated to prevent capsular adhesions, provided these movements do not transmit tension proximally to the knee.
Phase 3: Active Rehabilitation and Strengthening (Weeks 8 to 12+)
Once full, passive knee extension is successfully achieved without neurological symptom exacerbation, aggressive physical therapy is initiated. The focus shifts to restoring active joint mobility, breaking down extraneural soft tissue adhesions, and maintaining the suppleness of the denervated distal musculature. Electrical muscle stimulation (EMS) of the denervated gastrocnemius and soleus may be employed to retard muscle atrophy, although its definitive efficacy remains debated in the literature. Active-assisted and eventually active resistance exercises are introduced for the antagonistic muscle groups (anterior compartment) to maintain overall limb function.
Phase 4: Sensory Protection and Long-Term Surveillance (Months 3 to 24+)
Because axonal regeneration occurs at a painfully slow rate of approximately 1 mm per day (or 1 inch per month), plantar sensation will be completely absent for an extended period, often exceeding 12 to 18 months depending on the level of the injury. During this prolonged denervation phase, patients must be rigorously educated on meticulous foot care. Daily visual skin inspections using a mirror are mandatory. The patient must be fitted with custom orthotic, offloading footwear or a specialized Ankle-Foot Orthosis (AFO) to prevent unrecognized microtrauma, pressure necrosis, and the subsequent development of neurotrophic ulcerations or Charcot neuroarthropathy. Serial clinical exams and EMGs are performed every 3 to 6 months to monitor the advancing Tinel's sign and document objective signs of motor reinnervation.
Summary of Landmark Literature and Clinical Guidelines
The surgical management of peripheral nerve injuries, particularly the complex tibial nerve, is heavily grounded in decades of foundational neurobiological research and evolving microsurgical clinical guidelines. The seminal works of Sir Herbert Seddon and Sir Sydney Sunderland remain the absolute bedrock of peripheral nerve injury classification. Seddon’s classification (Neurapraxia, Axonotmesis, Neurotmesis) and Sunderland’s subsequent five-degree expansion provided the first physiological framework for understanding Wallerian degeneration and predicting the potential for spontaneous recovery versus the absolute necessity for surgical intervention.
Landmark clinical studies by Kline and Hudson in the late 20th century revolutionized the intraoperative assessment of neuromas-in-continuity. Their extensive series demonstrated the critical utility of intraoperative Nerve Action Potential (NAP) monitoring. According to their established guidelines, if a NAP can be transmitted across a neuroma-in-continuity at 8 to 12 weeks post-injury, neurolysis alone is indicated, yielding superior functional outcomes compared to resection. Conversely, the absence of a NAP definitively mandates neuroma resection and interpositional grafting. This physiological triage remains a cornerstone of modern peripheral nerve surgery.
The evolution of autogenous nerve grafting, heavily championed by Millesi and later Mackinnon, shifted the paradigm away from repairs performed under high tension. Millesi’s landmark papers established that a tension-free interfascicular cable graft, despite introducing two coaptation sites (proximal and distal), results in vastly superior axonal regeneration compared to a single primary repair performed under tension. Tension induces profound intraneural ischemia, leading to massive fibroblastic proliferation and impenetrable scar blockades.
Modern clinical guidelines emphasize the critical importance of timing and graft length. Literature consistently demonstrates that motor recovery is significantly inversely proportional to both the delay in surgery and the length of the nerve graft required. Grafts exceeding 10 to 12 centimeters in the lower extremity have a notoriously poor prognosis for meaningful distal motor recovery (e.g., intrinsic foot musculature), primarily due to the irreversible degradation of motor endplates that occurs before the slowly regenerating axons can traverse the extensive gap. Consequently, contemporary guidelines strongly advocate for early exploration of sharp transections, timely intervention (within 3-6 months) for non-recovering blunt injuries, and the prioritization of protective sensory recovery and proximal motor function (plantar flexion) when counseling patients on expected surgical outcomes.
