The wrist and hand

1
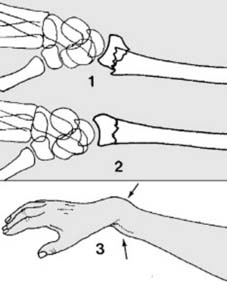
Colles fracture:
A Colles fracture is a fracture of the radius within 2.5 cm of the wrist (1), with a characteristic deformity if displaced. It is the commonest of all fractures. It is seen mainly in middle-aged and elderly women, and osteoporosis is a frequent contributory factor. It usually results from a fall on the outstretched hand (2), and generally the distal radial fragment remains intact. (See Frame 45 et seq. for those other cases where the radiocarpal joint is involved.)
2
Displacements (a):
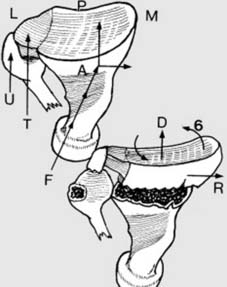
The
six
characteristic features of a displaced Colles fracture (see later for details) are shown in this foreshortened view of the pronated right arm, viewed from below. The slight obliquity of impact (F) produces the two most striking features of
dorsal and radial displacement
(D & R) of the distal fragment. (T = triangular fibrocartilage; U = ulnar styloid; M = medial; L = lateral)

3
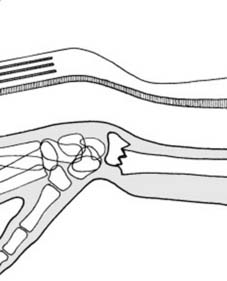
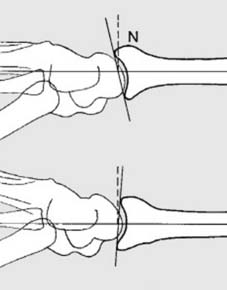
Displacements (b):
The deformity can be followed by studying the wrist in the two planes in which the radiographs are usually taken. The impact (F) fractures the radius through the cancellous bone of the metaphysis. With greater violence the anterior periosteum tears, and the distal fragment tilts into
anterior angulation
(1) with loss of the 5° anterior tilt of the joint surface.
4
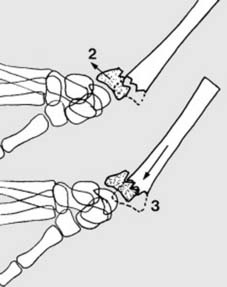
Displacements (c):
With greater violence there is
dorsal displacement of the distal fragment
(2). The shaft of the radius is driven into the distal fragment leading to impaction (3). (The dotted lines indicate the position of the distal fragment prior to any displacement.)
5
Displacements (d):
The altered contour of the wrist in a badly displaced Colles fracture is striking, and is referred to as a ‘dinner fork deformity’. When viewed from the side, the wrist has the same curvature as a fork, with the tines resembling the fingers.

6
Displacements (e):
This radiograph shows a typical displaced Colles fracture. The anterior angulation, dorsal displacement, and impaction are obvious (deformities 1,2,3).
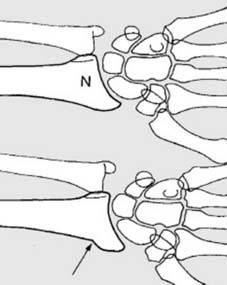
7
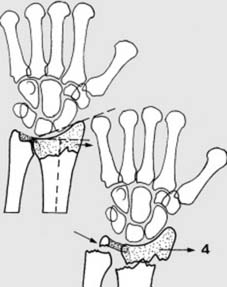
Displacements (f):
In the AP plane, a small lateral component of the force of impact causes
lateral (radial) displacement of the distal fragment
(4). The distal fragment is attached to the ulnar styloid by the triangular fibrocartilage, and generally this leads to avulsion of the ulnar styloid. Note that in the AP projection of the normal wrist that the joint surface has a tilt of 22°.

8
Displacements (g):
Sometimes the triangular fibrocartilage is torn; in either case there is disruption of the inferior radio-ulnar joint. The distal fragment tilts laterally into
ulnar angulation
(5) (reducing the tilt to less than 22°) and impacts. The sixth feature is a rotational or torsional deformity (6 in Frame 2), not obvious in either AP or lateral projections.

9
Displacements (h):
In this AP radiograph of a Colles fracture, note the features just mentioned, i.e. radial deviation, ulnar angulation and impaction of the distal fragment.

10
Diagnosis:
1. If there is pain in the wrist and tenderness over the distal end of the radius after a fall, radiographs must be taken in every case. The site of maximum tenderness will help to differentiate fracture of the scaphoid (but see scaphoid fractures). 2. Where there is marked displacement the characteristic appearance leaves little diagnostic doubt. Note that in the normal wrist the radial styloid lies 1 cm distal to the ulnar.
11
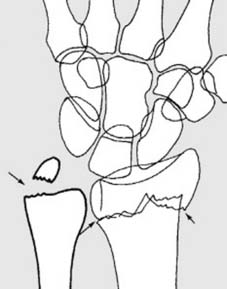
Radiographs (a):
In the majority of cases the fracture is easily identified. Sometimes it may be missed because impaction has rendered the fracture line inconspicuous. If in doubt, look at the angle between the distal end of the radius and the shaft in the lateral radiograph. Decrease to less than 0° is suggestive of fracture (but enquire about previous injury).
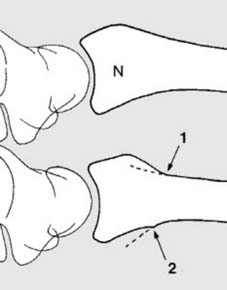
12
Radiographs (b):
The minimally displaced fracture will also reveal itself in the lateral projection by an increase in the posterior radial concavity, often with local kinking (1) or by a separate or accompanying break in the smooth curve of the anterior surface of the radius (2).
13
Radiographs (c):
In the AP view of the wrist, look for any irregularity in the smooth lateral aspect of the radius.
If there is any doubtful radiographic feature suggesting fracture, return to the patient
and confirm whether there is any localised tenderness over the suspect area

14
Diagnosis
ctd:
As stated, a Colles fracture is generally caused by a fall on the outstretched hand – a mechanism common to many upper limb fractures. Although other injuries in the arm occurring in association with Colles fracture are
uncommon
, clinically the scaphoid, elbow and shoulder should be examined, and on the radiographs the scaphoid should be scrutinised. (Special views are required if an associated scaphoid fracture is strongly suspected.)
15
Treatment: Does the fracture require manipulation? (a):
If the fracture is grossly displaced, it obviously should be reduced (1). If undisplaced, no manipulation is needed (2). Between these extremes, the following additional factors may be considered: if there is a readily appreciated naked eye deformity (3) manipulation should be carried out (but distinguish between
swelling
and
deformity
.)
16
Does the fracture require manipulation? (b):
If there is displacement of the ulnar styloid, this indicates
serious disruption of the inferior radio-ulnar joint
. (Acute ulnar angulation of the distal fragment is also evidence of this.) An attempt at correction should be made
irrespective of other appearances
17
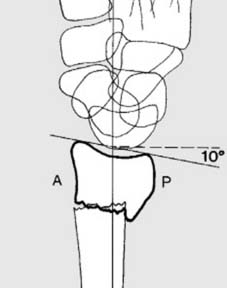
Does the fracture require manipulation? (c):
If the joint line in the lateral projection is tilted 10° or more posteriorly rather than anteriorly, the fracture should be manipulated: but in the very old, frail patient somewhat greater degrees of deformity may be accepted.
NEXT
Colles Fractures: Unraveling Hand the Wrist Injuries & Deformities
Updated: Feb 2026
59 Views
Key Medical Takeaway
For anyone wondering about Colles Fractures: Unraveling Hand the Wrist Injuries & Deformities, A Colles fracture is a common break in the radius bone, typically occurring within 2.5 cm of the wrist joint. It often results from a fall on the outstretched hand, leading to characteristic displacements like dorsal and radial displacement, and anterior angulation. This can create a ‘dinner fork deformity’ affecting the hand the wrist.
Table of Contents

Keywords