1.
General principles:
1
The main concern
in any spinal injury is less with the spine itself than with the closely related neurological elements (the spinal cord, issuing nerve roots and cauda equina).
2
If there is no neurological complication
the chances of later neurological involvement must be assessed; if there is some risk of this,
precautions must be taken to see that this is avoided at all stages
.
3
If there is an incomplete paraplegia
or other major neurological problem complicating the injury
great care must be taken to see that no deterioration is allowed to occur
.
4
If paraplegia is present and complete
, the prognosis regarding potential recovery must be firmly established as early as possible. Only if this is pronounced
total and permanent
can vigilance in the handling of the spinal injury be relaxed.
In summary, the key to the management of spinal injuries is a thorough understanding of the nature of any damage to the bony elements, the supportive ligamentous structures, and the related neurological structures.
2
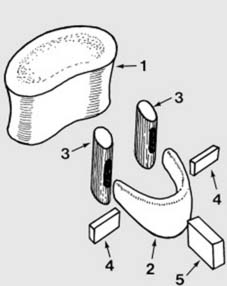
Anatomical features (after Kapandji 1) (a):
The components of a typical vertebra have a complex relationship, and can be illustrated with an exploded diagram. The elements comprise the vertebral body (1) composed of cancellous bone covered with an outer shell of cortical bone, the horseshoe-shaped neural arch (2), two articular masses or processes which take part in the facet (interarticular) joints (3) and the transverse (4) and spinous (5) processes.
3
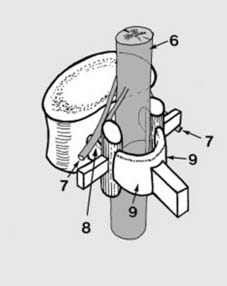
Anatomical features (b):
When these components are brought together they form a protective bony covering for the cord (6) and the issuing nerve roots (7). The neural arch (2) is divided by the articular processes (3) into pedicles (8) and laminate (9).
4
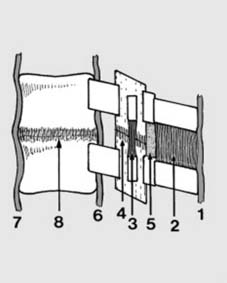
Anatomical features (c):
The vertebrae are bound together by the following structures: The supraspinous (1), interspinous (2), intertransverse (3) and capsular ligaments (4), and the ligamentum flavum (5): together these form the so-called posterior ligament complex. Playing a less powerful but nevertheless important role are the posterior (6) and anterior (7) longitudinal ligaments and the annular ligaments (8). Trauma may result in damage to any of the bony or ligamentous structures of the spine, in isolation or in combination.
5.
Assessment of spinal injuries (a):
In managing any case of spinal injury it is important to determine which structures have been involved and the extent of the damage they have suffered; with this information an assessment may be made of the risks of complication. Note: 1. The history may direct you to the type of injury to suspect; 2. The clinical examination may be a valuable guide to the extent of bony and ligamentous injury (and any neurological complication); 3. Investigation by X-ray and CT scan is likely to provide the most information; and MRI scans if available may help clarify the extent of any associated soft tissue damage, especially the intervertebral discs and the posterior ligament complex.
It is important to make an early assessment of the stability of the spine, i.e. to assess whether it is able to withstand stress without progressive deformity or further neurological damage.
Instability may be purely mechanical
(e.g. in some compression fractures where further kyphotic deformity may occur).
Instability may be neurological
(e.g. where shifting or further extrusion of bone fragments within the spinal canal may lead to neurological deterioration).
Combined mechanical and neurological instability
may be present.
In assessing instability it may be helpful to regard the spine as having three main elements or columns
.
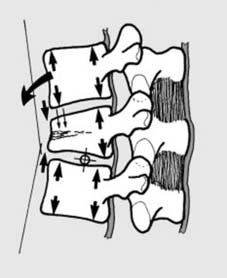
6
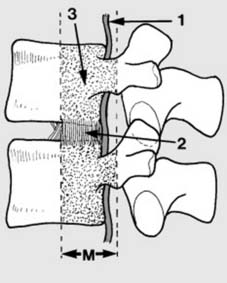
Assessment of spinal injuries (b):
The
middle column
(M) consists of the posterior longitudinal ligament (1), the posterior part of the annular ligament (2), and the posterior wall of the vertebral column (3). Unstable injuries occur when damage to the middle column is
combined
with damage to either the anterior column or damage to the posterior column.
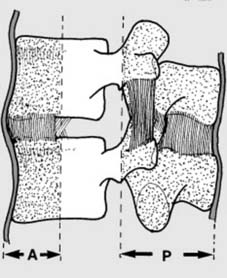
7
Assessment of spinal injuries (c):
The
posterior column
(P), vital for stability, comprises the neural arch, the pedicles, the spinous process, and the post. ligt. complex. The
anterior column
(A) is formed by the anterior longitudinal ligament, and the anterior parts of the annular ligament and vertebral body. Note that failure of these columns in their role as supports can be due to bony or ligament involvement. Four categories are recognised in the Denis Classification of spinal injury:
8
Compression fractures (a):
Simple compression fractures are common stable injuries involving the anterior column only. Hyperflexion of the spine round an axis passing through the disc space leads to mechanical failure of bone with either
anterior
(Illus.) or
lateral
wedging. The height of the posterior part of the vertebral body is maintained. (Note that
severe
wedging – e.g. more than 15–20° – often indicates damage to the other columns and a burst fracture or fracture dislocation.)
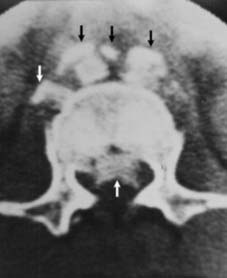
9
Burst fractures (b):
Axial loading of the spine may cause failure of the anterior and middle columns. One or both end plates may be involved, and bone fragments may be extruded into the spinal canal, compromising the neurological structures and more controversially causing neurological instability. Radiographs may show the vertebral body fracture, loss of vertebral height, and in the AP, laminar fractures and separation of the pedicles. (Illus: CT scan showing displacement of bony fragments both anteriorly and posteriorly.)
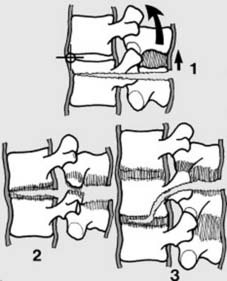
10
Seat belt type injuries (c):
Rapid deceleration causes the spine to jack-knife round an axis brought forward by the lap strap part of a seatbelt, and
tension
forces lead to failure of the posterior and middle columns. The spine is unstable in flexion. Failure may occur entirely through bone (Chance fracture) (1), or ligaments (2), or a combination (3), involving either one (1 & 2) or two (3) levels of the spine. Injuries of this pattern may be seen in situations outside road traffic accidents, but the essential element is tension failure.
11
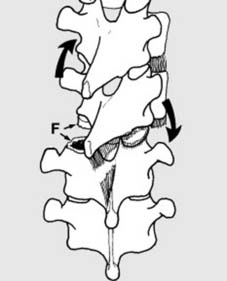
Fracture–dislocations (d):
All 3 columns fail in these unstable injuries. Suspect if: 1. There are multiple rib or transverse process fractures (as from D1 to D8 the ribs and sternum give additional support to the spine); 2. There is a slight increase in the height of a disc or a fracture of an articular process.
Types:
(a)
Flexion–rotation fracture–dislocation
. There is often a fracture of an articular process on one side (F), or a slicing fracture through a vertebral body, leading to rotation and subluxation of the spine.
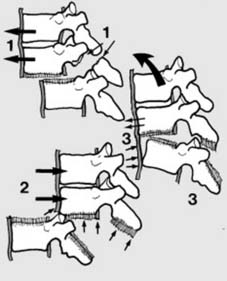
12
Fracture–dislocations (d)
ctd:
Shear types of fracture–dislocation: In the
posteroanterior type
(1) the upper segment shears forwards, often with fracture of the posterior arch at 1 or 2 levels. In the
anteroposterior type
(2) there is complete ligamentous disruption, but often no fracture. In the
flexion–distraction type
(3) there is an anterior annular tear with stripping of the anterior long. ligt. allowing anterior subluxation: this is a tension type of injury as in the seatbelt lesion.
13.
Neurological examination: basic principles:
Where there is evidence of a deficit, a thorough neurological examination is required on admission; this must include as a minimum:
1 Testing for evidence of muscle activity and power in all muscle groups below the level of injury.
2 Testing sensation of pin prick and light touch over the entire area affected.
3 Testing proprioception.
4 Testing the reflexes – the tendon reflexes, the plantar responses; the anal reflex (stimulation of the perineum leading to contraction of the external anal sphincter) and the glansbulbar reflex (compression of the glans leading to perineal muscle contraction).
Note also the following points:
1 Where the spinal cord is involved, the neurological level should be determined.
2 The neurological level and the level of any bony injury should be correlated. Absence of any obvious bony injury at the neurological level should lead to further local investigation (e.g. by MRI scan).
3 The severity of any deficit should be assessed.
4 If the findings indicate a
complete
spinal lesion, the examination should be repeated after 6 hours, 12 hours and 24 hours.
14
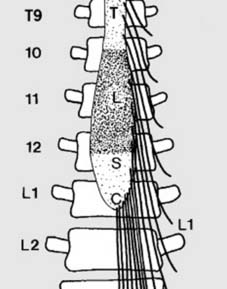
Anatomical features (a):
Note:
1. The spinal cord ends at L1; any injury distal to this can involve the cauda but not the cord. 2. All the lumbar and sacral segments of the cord lie between T10 and L1 only. 3. Injuries at the thoracolumbar junction produce a great variety of neurological disturbances as:
NEXT
Anatomical features (b): Cervical cord
The Spine: Master Injury Assessment & Ensure Stability
Updated: Feb 2026
53 Views
Key Medical Takeaway
Looking for accurate information on The Spine: Master Injury Assessment & Ensure Stability? Managing spine the spine injuries involves thoroughly understanding damage to bony, ligamentous, and neurological structures. Early assessment determines the extent of injury and spinal stability, crucial for preventing progressive deformity or neurological deterioration. Imaging (X-rays, CT, MRI) clarifies damage, and the three-column concept helps categorize instability to guide appropriate management and treatment strategies.
Table of Contents

Keywords