
11
Palpation
The sharp edge of a fracture may be palpable. Note also the presence of localised oedema. This is a particularly useful sign over hair-line and stress fractures. The development of oedema may, however, take some hours to reach detectable proportions.

12
Other signs
If the fracture is mobile, moving the part may produce angulation or crepitus from the bone ends rubbing together. In addition, the patient will experience severe pain from such movement. These signs may be inadvertently observed during routine examination of the patient, but should not be sought unless the patient is unconscious and the diagnosis is in doubt.
13
Radiographic examination
In every case of suspected fracture, radiographic examination of the fracture is mandatory. Radiographs of the part will generally give a clear indication of the presence of a fracture and provide a sound basis for planning treatment. In the case where there is some clinical doubt, radiographs will reassure patient and surgeon and avert any later medicolegal criticism.
Radiographers in the United Kingdom receive thorough training in the techniques for the satisfactory visualisation of any suspect area, but it is essential that they in turn are given clear guidance as to the area under suspicion. The request form must be quite specific, otherwise mistakes may occur. At its simplest, the request must state
both the area to be visualised and the bone suspected of being fractured
. It is desirable to include the joints above and below the fracture. It need hardly be stressed that a thorough clinical examination should precede the completion of the radiographic request if repetition and the taking of unnecessary films are to be avoided.
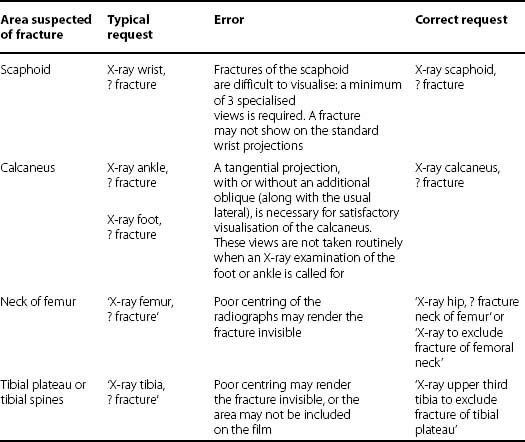
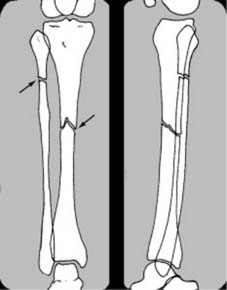
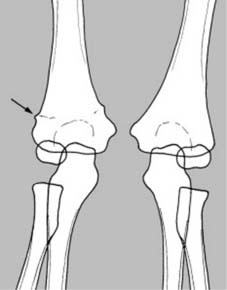
The following table lists some of the commonest errors made in the filling in of request forms

14
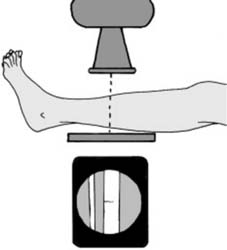
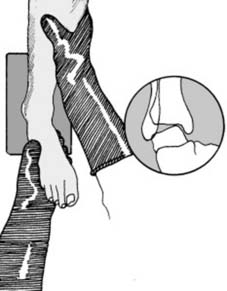
The standard projections:
These are an
anteroposterior (AP) and lateral
. Ideally the beam should be centred over the area of suspected fracture, with visualisation of the proximal
and
distal joints. This is especially important in the paired long bones where, for example, a fracture of the tibia at one level may be accompanied by a fibular fracture at another
15
Comparison films:
Where there is some difficulty in interpreting the radiographs (e.g. in the elbow region in children where the epiphyseal structures are continually changing, or where there is some unexplained shadow, or a congenital abnormality) films of the other side should be taken for direct comparison
16
Oblique projections
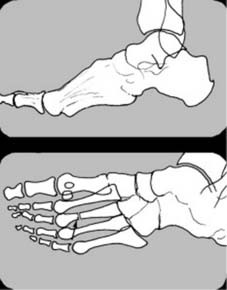
In the case of the hand and foot, an oblique projection may be helpful when the lateral gives rise to confusion due to the superimposition of many structures. Such oblique projections may have to be specifically requested when they are not part of an X-ray department’s routine
17
Localised views
Where there is marked local tenderness, but routine films are normal, coned-down localised views may give sufficient gain in detail to reveal for example a hair-line fracture: if such films are also negative, the radiographs should be repeated after an interval of 10–14 days if the symptoms are persisting (see also Hair-line Fractures in Ch. 1/
Frame 13
)
18
Stress films (a)
Stress films can be of value in certain situations: (i) When a complete tear of a major ligament is suspected, e.g., where the lateral ligament of the ankle is thought to be torn, radiographs of the joint taken with the foot in forced inversion may demonstrate instability of the talus in the ankle mortice. (Local or general anaesthesia may be required in fresh injuries.)
19
Stress films (b)
(ii) Stress films may also be used where there is some doubt as to stability of a uniting fracture. They may also be employed where the possibility of refracture arises.
Other visualisation techniques
1 CT (CT) scans
These can show tissue slices in any plane, but characteristically in median sagittal, parasagittal, coronal, and most importantly, transverse planes. The last projection cannot be readily obtained with plain X-rays, and can often provide useful additional information which is not otherwise available. In addition, in the CT scan there is a greater range of grey scale separation, allowing a greater differentiation of tissue types. It is of particular value in:
• Vertebral fractures, to show the relationship between bony fragments and the spinal canal
• Acetabular floor fractures, to clarify the degree of disturbance of the articular surface
• Pelvic fractures, to show the number of elements involved and their relationship. In some cases it may be possible to display and rotate informative 3-D reconstructions
• In calcaneal and other fractures involving joints, to visualise the position of the elements and the degree of joint disturbance.
2 AP and lateral tomography
In this X-ray technique the tube and film are rotated (or slid) in opposite directions during the exposure. Their position relative to one another and the part being examined determines the tissue slice being clearly visualised. The results are inferior to those obtained by CT scanning, but may be helpful if the latter is not available.
3 Technetium bone scans
Technetium tagged methylene diphosphate ( 99 Tc m -methylene diphosphate (MDP)) can be used 48 hours after an injury to demonstrate bone activity at a fracture site, and confirm the presence of a fracture when other methods of detection have failed.
4 MRI scans
These avoid any exposure to X-radiation and produce image cuts as in CT scans with a greater ability to distinguish between different soft-tissues. In the trauma field they are of particular value in assessing neurological structures within the skull and spinal canal, and meniscal and ligamentous structures about the knee and shoulder.
5 Bone scanning with SPECT (single-photon-emission computed tomography)
This allows physiological assessment of bone by identifying areas of increased osteoblastic activity. It is highly sensitive.
6 Ultrasound
Ultrasound imaging is of great sensitivity and of value in assessing the presence of fluid (e.g. blood) within the abdominal cavity in the patient with multiple injuries; it may also be helpful in elucidating injuries to the quadriceps tendon, the patellar ligament and the Achilles tendon.
Pitfalls
A number of fractures are missed with great regularity – sometimes with serious consequences. You should always be on the look-out for the following:
1 An elderly patient who is unable to weight bear after a fall must be examined most carefully. The commonest cause by far is a fracture of the femoral neck, and this must be eliminated in every case. If the femoral neck is intact, look for a fracture of the
pubic rami
. Note that, on the rare occasion, a patient with an impacted fracture of the femoral neck may be able to weight bear, albeit with pain.
2 If a car occupant suffers a fracture of the patella or femur from a dashboard impact, always eliminate the presence of a silent dislocation of the hip.
3 If a patient fractures the calcaneus in a fall, examine the other side most carefully. Bilateral fractures are extremely common, and the less painful side may be missed.
4 If a patient complains of a ‘sprained ankle’ always examine the foot as well as the ankle. Fractures of the base of the fifth metatarsal frequently result from inversion injuries, and are often overlooked. The mistake of not performing a good clinical examination in these circumstances is compounded by requesting radiographs of the ankle (which do not show the fifth metatarsal bone).
5 In the unconscious patient, injuries of the cervical spine are frequently overlooked. It pays to have routine screening films of the neck, chest and pelvis in the unconscious patient.
6 Impacted fractures of the neck of the humerus are often missed, especially when one view only is taken. Conversely, in children, the epiphyseal line is often wrongly mistaken for fracture.
7 Posterior dislocation of the shoulder may not be diagnosed when it should be at the initial attendance. This is because the humeral head comes to lie directly behind the glenoid, and is not detected if only a single AP projection is taken. If there is a strong suspicion of injury, and especially if there is deformity of the shoulder, a second projection is
essential
if no abnormality is noted on the AP film. (Two views should be taken routinely in all injuries, but in many departments the shoulder, for no good reason, is excluded from this rule.)
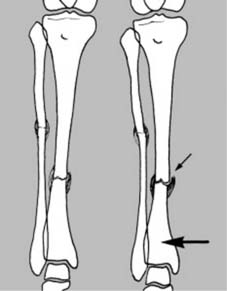
8 Apparently isolated fractures of either the radius or ulna should be diagnosed with caution. The Monteggia and Galeazzi fracture–dislocations are still frequently missed. In the same way, it is unwise to diagnose an isolated fracture of the tibia until the whole of the fibula has been visualised; fracture of the tibia close to the ankle is, for example, often accompanied by fracture of the fibular neck.
9 At the wrist, greenstick fractures of the radius in children are often overlooked due to lack of care in studying the radiographs.
10 In adults, fractures of the radial styloid or Bennett’s fracture may be missed or treated as suspected fractures of the scaphoid. Complete tears of ulnar collateral ligament of the MP joint of the thumb are frequently overlooked, sometimes with severe resultant functional disability.
Treatment of fractures
Primary aims
The primary aims of fracture treatment are:
1 The attainment of sound bony union without deformity
2 The restoration of function, so that the patient is able to resume his former occupation and pursue any athletic or social activity he wishes.
To this might be added ‘as quickly as possible’ and ‘without risk of any complications, whether early or late’. These aims cannot always be achieved, and in some situations are mutually exclusive. For example, internal fixation of some fractures may give rapid restoration of function, but at the expense of occasional infection. The great variations that exist in fracture treatment are largely due to differences in interpretation of these factors and their relevance in the case under consideration; they are in constant flux, with on the one hand the development of more sophisticated methods of fracture fixation and new antibiotics, and on the other the emergence of antibiotic resistant organisms.
Resuscitation
If a limb fracture is a patient’s sole injury, resuscitation is less frequently required, so that it is often possible to proceed with treatment without undue delay (although unfitness for anaesthesia may sometimes upset this ideal). If, however, a fracture is complicated by damage to other structures, or involvement of other systems, then treatment of the fracture usually takes second place. Immediate action must be taken to correct any life-endangering situation which may be present or anticipated.
Advanced trauma life support (ATLS)
It is recognised that a well-organised trauma team can give the best treatment to a severely injured patient. The core trauma team will normally consist of ten staff: a team leader, an anaesthetist and his assistant, a general surgeon, an orthopaedic surgeon, an emergency department physician, two nurses, a radiographer, and a note-taker (scribe). Each member has his own specific areas of responsibility. The team leader should not normally touch the patient, but orchestrate the team.
Additional staff will include porters, blood bank staff including a haematologist, and a biochemist. A neurosurgeon, thoracic surgeon, plastic surgeon, and radiologist should also be available at short notice.
To maintain such a team with its equipment makes heavy demands, and is only possible in a few hospitals which have the necessary workload and resources. In most situations, especially away from large centres, smaller teams are involved and assessment and management follow a more linear approach (as adopted below).
Initial management
Some general principles in the initial management of cases of multiple injuries are well established, and may be summarised with the mnemonic ABCDE(F)
A = Airway
1 Any blood, mucus or vomit must be removed from the upper respiratory passages by suction or swabbing. Dentures should be looked for and extracted. In the more minor situations, respiratory obstruction may be avoided by support of the jaw, a simple airway, and turning the patient on his side.
2 An endotracheal tube may have to be passed:
• in the unconscious patient with an absent gag reflex
• where inhalation of mucus or vomit has already taken place (or is suspected), for clearing of the respiratory passages under vision
• where there is bleeding from the upper airway
• for the more effective management of cases where there is respiratory difficulty or evidence of hypoxia, e.g. in cases of flail chest. Where there is need for intubation in a patient when a cervical spine injury is suspected, the procedure should be carried out with great care, avoiding excessive cervical spine extension; naso-tracheal intubation should be used. Confirm placement by auscultation (and/or by a radiograph).
B = Breathing
1 <a id="para0660" style="background: none 0px 0px repeat scroll transparent; border: 0px none; margin: 0px; outline: none 0p
