INTRODUCTION TO PATELLAR FRACTURE FIXATION
The patella is the largest sesamoid bone in the human body, serving a critical biomechanical role in the extensor mechanism of the knee. It increases the moment arm of the quadriceps tendon, thereby enhancing the mechanical advantage of knee extension by up to 30%. Fractures of the patella disrupt this vital mechanism, leading to profound functional impairment if not meticulously addressed.
The Arbeitsgemeinschaft für Osteosynthesefragen (AO) group has long advocated for the tension band wiring principle as the gold standard for the fixation of displaced transverse patellar fractures. When executed correctly, this technique neutralizes the distracting forces of the extensor mechanism and converts them into dynamic compressive forces across the articular surface during knee flexion. This biomechanical conversion is paramount, as it facilitates earlier union, allows for immediate postoperative motion, and mitigates the stiffness traditionally associated with prolonged immobilization.
Clinical Pearl: The success of tension band wiring relies entirely on the integrity of the opposite cortex (the articular surface). If the articular surface is severely comminuted and cannot provide a stable buttress, the tension band principle will fail, leading to fracture displacement and hardware failure.
BIOMECHANICAL PRINCIPLES OF THE TENSION BAND
To master the tension band wiring technique, the surgeon must first understand the forces acting upon the patella. The patella is subjected to massive tensile forces anteriorly, generated by the pull of the quadriceps muscle against the resistance of the patellar tendon.
When a transverse fracture occurs, these forces distract the anterior cortex. By placing a stout wire loop (the tension band) on the anterior surface of the patella, the surgeon creates a mechanical restraint. As the knee flexes, the tension band resists anterior gapping. Because the anterior cortex cannot distract, the force is redirected through the fulcrum of the bone, resulting in compression at the articular surface.
For the tension band principle to function optimally:
* The tension band must be applied to the tension surface (anteriorly).
* The bone must be able to withstand compression on the opposite surface (articular cartilage).
* The fixation must be secure enough to withstand the physiological loads of early active mobilization.
INDICATIONS AND PREOPERATIVE PLANNING
Indications for Operative Intervention
Not all patellar fractures require surgery. However, operative fixation via tension band wiring is strictly indicated in the presence of:
* Displacement of the fracture fragments greater than 3 mm.
* Articular step-off or incongruity greater than 2 mm.
* Disruption of the extensor mechanism (inability to perform a straight leg raise).
* Open fractures requiring immediate debridement and stabilization.
Preoperative Assessment
Standard anteroposterior (AP), lateral, and axial (skyline) radiographs are mandatory. The lateral view is particularly critical for assessing the degree of displacement and comminution. In cases of high-energy trauma or suspected osteochondral shearing, a CT scan may be warranted to fully delineate the fracture pattern and plan for supplemental screw fixation.
SURGICAL ANATOMY AND POSITIONING
Patient Positioning
The patient is placed in the supine position on a radiolucent operating table. A tourniquet is applied to the proximal thigh to ensure a bloodless surgical field, which is critical for identifying small articular fragments and assessing retinacular tears. A small bump may be placed under the ipsilateral hip to correct natural external rotation, ensuring the patella faces directly anteriorly. The limb is prepped and draped free to allow full, unrestricted flexion and extension of the knee during the procedure.
Surgical Approach
A midline longitudinal incision is universally preferred over transverse incisions. The longitudinal approach is extensile, respects the vascular supply to the skin flaps, and can be easily incorporated into a standard midline arthrotomy should the patient require total knee arthroplasty in the future.
The incision extends from the superior pole of the patella to the tibial tubercle. Full-thickness fasciocutaneous flaps are elevated medially and laterally to expose the entire anterior surface of the patella and the medial and lateral extensor retinacula.
SURGICAL TECHNIQUE 54-21: STANDARD TENSION BAND WIRING
The following represents the definitive, step-by-step execution of the AO tension band wiring technique using Kirschner wires (K-wires).
1. Joint Preparation and Debridement
Approach the patellar fracture in the usual fashion. Carefully clean the fracture surfaces of all organized blood clots, fibrin, and interposed soft tissue. Small, devitalized, non-articular fragments that impede reduction should be excised. Explore the full extent of the medial and lateral retinacular tears. Inspect the trochlear groove of the femur for any concomitant osteochondral damage. Thoroughly lavage the joint with sterile saline to remove intra-articular hematoma and debris.
2. Fracture Reduction
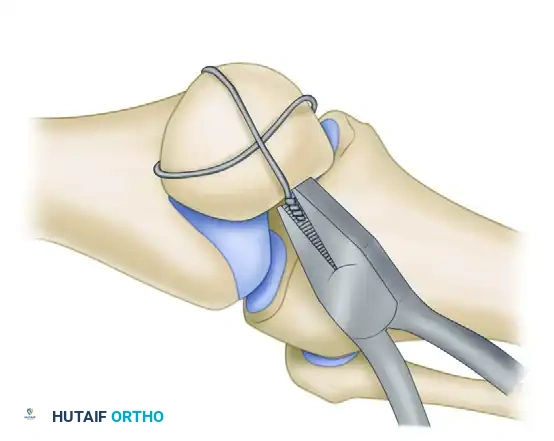
If the major proximal and distal fragments are large, reduce them accurately. Special attention must be directed toward restoring a perfectly smooth articular surface. Reduction is typically achieved using large, pointed reduction forceps (Weber clamps) applied to the superior and inferior poles.
Surgical Warning: Do not rely solely on the anterior cortical reduction. The anterior surface of the patella is naturally irregular. Anatomical reduction must be confirmed by palpating the articular surface through the retinacular tears.
3. Kirschner Wire Insertion
With the fracture anatomically reduced and held firmly with clamps, drill two 2.0-mm K-wires from inferior to superior through each fragment.
* Place these wires approximately 5 mm deep to the anterior surface of the patella.
* Position them along lines dividing the patella into medial, central, and lateral thirds.
* It is imperative to insert the wires as parallel as possible to facilitate uniform compression and prevent binding.
Alternative Retrograde Technique: In cases of difficult reduction, it is often easier to insert the K-wires through the fracture site into the proximal fragment in a retrograde manner before reduction. This is made easier by tilting the proximal fracture fragment anteriorly about 90 degrees. Once the wires pierce the superior pole, they are withdrawn until flush with the fracture site. The fracture is then reduced, clamped, and the wires are driven antegrade into the distal fragment.
Leave the ends of the K-wires long, protruding beyond the patella and the quadriceps/patellar tendon attachments.
4. Application of the Tension Band Wire
Pass a strand of 18-gauge stainless steel wire transversely through the quadriceps tendon attachment, as close to the superior bone pole as possible, passing deep to the protruding K-wires.
Route the wire over the anterior surface of the reduced patella. Pass it transversely through the patellar tendon attachment on the inferior fragment, again keeping it deep to the protruding K-wires and as close to the bone as possible. Bring the wire back over the anterior patellar surface to meet the upper end.
While a simple loop can be used, placing the wire in a figure-of-eight fashion is biomechanically superior, as it provides better rotational stability and more uniform compression across the fracture site.
5. Tensioning and Verification
Tighten the 18-gauge wire symmetrically. The wire should be tightened until the fracture is slightly overcorrected (opened microscopically on the anterior surface), ensuring maximum compression at the articular surface.
Check the reduction by palpating the undersurface of the patella with the knee fully extended. If the retinacular tears are insufficient to allow a finger into the joint, make a small, deliberate longitudinal incision in the retinaculum to permit digital palpation of the articular step-off.
6. Securing the Hardware
Once compression is confirmed, the K-wires must be secured to prevent postoperative migration—a common complication.
* Bend the upper ends of the two K-wires acutely anteriorly (approximately 180 degrees).
* Cut the bent ends short.
* Using a heavy impactor and mallet, embed the bent ends deep into the superior margin of the patella, ensuring they sit posterior to the wire loops. This locks the tension band in place.
* Cut the protruding ends of the K-wires short inferiorly, leaving just enough length to prevent the wire loop from slipping off, but short enough to avoid irritating the patellar tendon.
7. Retinacular Repair
The operation is not complete until the extensor mechanism is fully restored. Repair the medial and lateral retinacular tears meticulously using multiple interrupted heavy non-absorbable or slowly absorbable sutures (e.g., #1 or #2 Vicryl).
ADVANCED MODIFICATIONS FOR COMPLEX FRACTURES
The Schauwecker Technique for Comminuted Fractures
Standard tension band wiring is designed for simple transverse fractures. When comminution is present, the tension band alone may cause the fracture to collapse or telescope, leading to articular incongruity.
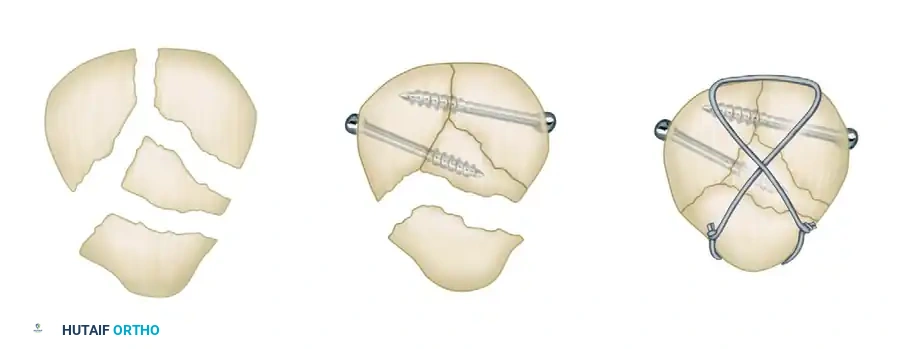
Schauwecker described a highly effective method of compression wiring using supplemental lag screws for comminuted fractures. The principle is to convert a multi-fragmentary fracture into a stable, bifragmental fracture before applying the tension band.
- Fragment Assembly: The comminuted fragments (usually at the inferior or superior pole) are anatomically reduced.
- Lag Screw Fixation: Mini-fragment lag screws (2.0 mm or 2.7 mm) are placed horizontally or obliquely to compress the comminuted fragments together. This effectively transforms the comminuted fracture into a simple transverse pattern.
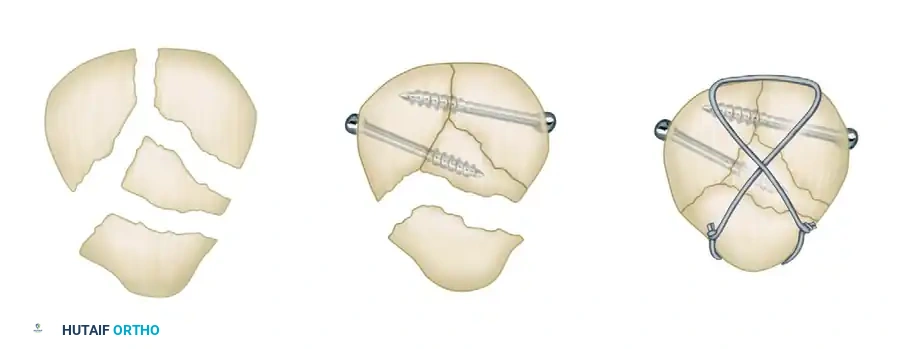
- Tension Band Application: Once the fracture is bifragmental, a standard figure-of-eight tension band wire is applied over the anterior surface of the patella to neutralize the extensor forces.
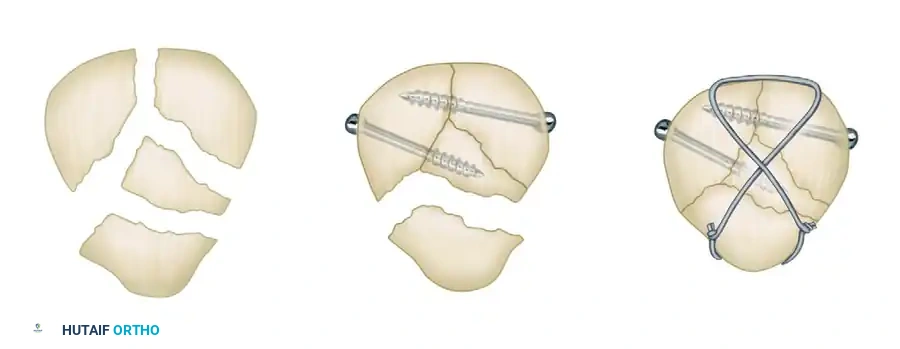
If the anterior cortex is split from the articular surface in the coronal plane, the fragment usually can be secured with the anterior tension band wire. If this is unsuccessful and the fragment is small and non-articular, it can be excised.
Cannulated Screw Tension Band Construct
A modern, highly favored alternative to K-wires involves the use of 4.0-mm partially threaded cannulated screws. This technique offers superior biomechanical strength and significantly reduces the incidence of symptomatic hardware prominence.
Instead of driving K-wires, two 4.0-mm cannulated screws are placed longitudinally from inferior to superior across the reduced fracture. These screws provide independent interfragmentary compression. The 18-gauge tension band wire is then passed directly through the hollow cannulae of the screws, rather than around protruding K-wire ends.


This construct creates a highly stable, low-profile fixation. The screws compress the articular surface, while the wire through the screws acts as the anterior tension band, neutralizing the distracting forces of the quadriceps.
POSTOPERATIVE CARE AND REHABILITATION
The success of patellar fracture fixation is heavily dependent on a structured, phased postoperative rehabilitation protocol. The tension band principle relies on early active flexion to produce compressive forces; however, the surgeon must balance this against the risk of fixation failure.
Phase I: Immediate Postoperative Period (Days 1-14)
- Immobilization: The limb is placed in full extension in a posterior plaster splint or a hinged, removable knee brace locked in extension.
- Weight-Bearing: The patient is allowed to ambulate while bearing weight as tolerated (WBAT) on the first postoperative day, provided the knee is locked in extension.
- Exercises: Isometric quadriceps sets and straight-leg raises (stiff-leg exercises) are encouraged immediately, beginning on postoperative day one. This prevents quadriceps atrophy and prevents adhesions in the suprapatellar pouch.
- Motion: The extent of active motion permitted in the immediate postoperative period is determined intraoperatively based on the stability of the fracture repair. If fixation is rock-solid, passive motion from 0 to 30 degrees may be initiated.
Phase II: Early Motion (Weeks 2-6)
- Active and active-assisted range-of-motion (ROM) exercises can be formally initiated when the surgical wound has healed, typically at 2 to 3 weeks.
- A controlled motion knee brace is highly recommended. The brace allows full extension and limits flexion to the degree permitted by the fixation (often starting at 0-45 degrees and advancing 15 degrees weekly).
- Caveat: In patients with less stable fixation, severe comminution, or extensive retinacular tears, active motion should be delayed until early fracture healing is evident radiographically. Initiating ROM exercises by the sixth postoperative week is desirable to prevent arthrofibrosis, but it is not always possible if stability is questionable.
Phase III: Strengthening and Return to Function (Weeks 6-24)
- Weeks 6-8: If clinical and radiographic healing is evident, the hinged knee brace can be discontinued. Progressive resistance exercises (closed kinetic chain) are initiated.
- Weeks 18-24: Unrestricted activity, including sports and heavy manual labor, can be resumed only when full, symmetric quadriceps strength has returned and the fracture is fully consolidated.
COMPLICATIONS AND REVISION SURGERY
Despite meticulous technique, complications can arise following tension band wiring of the patella.
Hardware Prominence and Irritation
The most common complication is symptomatic hardware, occurring in up to 40% of patients treated with traditional K-wires. The proximal K-wire ends or the wire knot can irritate the overlying skin and quadriceps tendon. Hardware can be safely removed after complete radiographic healing of the fracture (typically after 6 to 12 months) if it causes persistent symptoms. The use of cannulated screws significantly reduces this complication.
Loss of Fixation
Loss of reduction is a severe complication that demands immediate reassessment. If the fixation is lost and the fragments separate by 3 to 4 mm, or if 2 to 3 mm of articular incongruity develops, revision surgery is frequently required.
Clinical Pearl: If postoperative displacement occurs, examine the patient with the knee in full extension. If the reduction improves and the articular step-off resolves in extension, the patient can be treated conservatively by 6 weeks of rigid splinting or casting in full extension.
If the reduction does not improve in extension, revision open reduction and internal fixation (ORIF) is mandatory. In cases of catastrophic failure where the bone is too osteoporotic or comminuted to hold new hardware, a partial or total patellectomy must be considered as a salvage procedure, though this will result in a permanent extensor lag and decreased quadriceps power.
Infection and Nonunion
Superficial infections are managed with oral antibiotics, while deep infections require prompt surgical irrigation and debridement. Nonunion is rare (less than 2%) due to the excellent vascular supply of the patella, but when it occurs, it is usually the result of inadequate fixation or premature aggressive rehabilitation. Treatment requires revision ORIF with bone grafting.
📚 Medical References
- Tension band wiring–bone grafting for spondylolysis and spondylolisthesis: a clinical and biomechanical study, Spine 14:455, 1989.
- Haraldsson S, Willner S: A comparative study of spondylolisthesis in operations on adolescents and adults, Arch Orthop Trauma Surg 101:101, 1983.
- Harms J, Jeszenszky D, Stoltze D, et al: True spondylolisthesis reduction and monosegmental fusion in spondylolisthesis. In Bridwell KH, DeWald RL, eds: The textbook of spinal surgery, 2nd ed, Philadelphia, 1997, Lippincott-Raven. Harrington PR, Dickson JH: Spinal instrumentation in the treatment of severe progressive spondylolisthesis, Clin Orthop 117:157, 1976.
- Harrington PR, Tullos HS: Spondylolisthesis in children: observations and surgical treatment, Clin Orthop Relat Res 79:75, 1971.
- Harris IE, Weinstein SL: Long-term follow-up of patients with grade III and IV spondylolisthesis: treatment with and without fusion, J Bone Joint Surg 69A:960, 1987.
- Helenius I, Lamberg T, Osterman K, et al: Scoliosis Research Society outcome instrument in evaluation of long-term surgical results in spondylolysis and low-grade isthmic spondylolisthesis in young patients, Spine 30:336, 2005.
- Hensinger RN: Spondylolysis and spondylolisthesis in children, Instr Course Lect 32:132, 1983.
- Hensinger RN: Spondylolysis and spondylolisthesis in children and adolescents, J Bone Joint Surg 71A:1098, 1989.
- Hensinger RN, Lang JR, MacEwen GD: Surgical management of the spondylolisthesis in children and adolescents, Spine 1:207, 1976.
- Herbiniaux G: Traite sur divers accouchemens laborieux et sur les polypes de la matrice, Braxelles, 1782, JL DeBoubers. Huizenga BA: Reduction of spondyloptosis with two-stage vertebrectomy, Orthop Trans 7:21, 1983.
- Hu SS, Bradford DS, Transfeldt EE, Cohen M: Reduction of high-grade spondylolisthesis using Edwards instrumentation, Spine 21:367, 1996.
- Ivanic GM, Pink TP, Achatz W, et al: Direct stabilization of lumbar spondylolysis with a hook screw: mean 11-year followup period for 113 patients, Spine 28:255, 2003.
- Jackson DW, Wiltse LL, Cirincione RJ: Spondylolysis in the female gymnast, Clin Orthop Relat Res 117:68, 1976.
- Johnson JR, Kirwan EOG: The long-term results of fusion in situ for severe spondylolisthesis, J Bone Joint Surg 65B:43, 1983.
- Johnson LP, Nasca RJ, Dunham WK, et al: Surgical management of isthmic spondylolisthesis, Spine 13:93, 1988.
- Kaneda K, Satoh S, Nohara Y, et al: Distraction rod instrumentation with posterolateral fusion in isthmic spondylolisthesis: 53 cases followed for 18 to 89 months, Spine 10:383, 1985.
- Kilian HF: Schilderungen neuer Eckenformen und ihres Verhaltens in Leven, Mannheim, 1854, Verlag von Bassermann & Mathy. Kiviluoto O, Santavirta S, Salenius P, et al: Posterolateral spine fusion: a 1to 4-year follow-up of 80 consecutive patients, Acta Orthop Scand 56:152, 1985.
- Klinghoffer L, Murdock MG: Spondylolysis following trauma: a case report and review of the literature, Clin Orthop Relat Res 166:72, 1982.
- Lenke LG, Bridwell KH: Evaluation and surgical treatment of high-grade isthmic dysplastic spondylolisthesis, Instr Course Lect 52:525, 2003.
- Lenke LG, Bridwell KH, Bullis D, et al: Results of in situ fusion for isthmic spondylolisthesis, J Spinal Disord 5:433, 1992.
- Letts M, Smallmon T, Afanasiev R, et al: Fracture of the pars interarticularis in adolescent athletes: a clinical biomechanical analysis, J Pediatr Orthop 6:40, 1986.
- Lindholm TS, Ragni P, Ylikoski M, et al: Lumbar isthmic spondylolisthesis in children and adolescents: radiologic evaluation and results of operative treatment, Spine 15:1350, 1990.
- Lowe RW, Hayes TD, Kaye J, et al: Standing roentgenograms in spondylolisthesis, Clin Orthop Relat Res 117:80, 1976.
- Marchetti PG, Bartolozzi P: Classifi cation of spondylolisthesis as a guideline for treatment. In Bridwell KH, DeWald RL, eds: The textbook of spinal surgery, 2nd ed, Philadelphia, 1997, Lippincott-Raven. Matthiass HH, Heine J: The surgical reduction of spondylolisthesis, Clin Orthop Relat Res 203:34, 1986.
- Maurice HD, Morley TR: Cauda equina lesions following fusion in situ and decompressive laminectomy for severe spondylolisthesis: four case reports, Spine 14:214, 1989.
- McCarroll JR, Miller JM, Ritter MA: Lumbar spondylolysis and spondylolisthesis in college football players: a prospective study, Am J Sports Med 14:404, 1986.
- McPhee IB, O’Brien JP: Scoliosis in symptomatic spondylolisthesis, J Bone Joint Surg 62B:155, 1980.
- Meyerding HW: Spondylolisthesis, Surg Gynecol Obstet 54:371, 1932.
- Micheli LJ: Low back pain in the adolescent: differential diagnosis, Am J Sports Med 7:361, 1979.
- Miller SF, Congeni J, Swanson K: Long-term functional and anatomical followup of early detected spondylolysis in young athletes, Am J Sports Med 32:928, 2004.
- Mimatsu K: New laminoplasty after thoracic and lumbar laminectomy, J Spinal Disord 10:20, 1997.
- Molinari RW, Bridwell KH, Lenke LG, et al: Anterior column support in surgery for high-grade, isthmic spondylolisthesis, Clin Orthop Relat Res 394:109, 2002.
- Murray PM, Weinstein SL, Spratt KF: The natural history and long-term follow-up of Scheurermann kyphosis, J Bone Joint Surg 75A:236, 1993.
- Nachemson A: Repair of the spondylolisthetic defect and intertransverse fusion for young patients, Clin Orthop Relat Res 117:101, 1976.
- Neugebauer FL: A new contribution to the history and etiology of spondylolisthesis, New Sydenham Society Selected Monographs 121:1, 1988.
- Newman PH: A clinical syndrome associated with severe lumbosacral subluxation, J Bone Joint Surg 47B:472, 1965.
- Newman PH: Stenosis of the lumbar spine in spondylolisthesis, Clin Orthop Relat Res 115:116, 1976.
- Nicol RO, Scott JHS: Lytic spondylolysis: repair by wiring, Spine 11:1027, 1986.
- Nozawa S, Simizu K, Miyamoto K, et al: Repair of pars interarticularis defect by segmental wire fi xation in young athletes with spondylolysis, Am J Sports Med 31:359, 2003.
- Ohki I, Inoue S, Murata T, et al: Reduction and fusion of severe spondylolisthesis using halo-pelvic traction with a wire reduction device, Int Orthop 4:107, 1980.
- Osterman K, Snellman O, Poussa M, et al: Treatment of lumbar lytic spondylolisthesis using osteoperiosteal transplants in young patients, J Pediatr Orthop 1:289, 1981.
- Pedersen AK, Hagen R: Spondylolysis and spondylolisthesis: treatment by internal fi xation and bone grafting of the defect, J Bone Joint Surg 70A:15, 1988.
- Pizzutillo PD, Hummer CD III: Nonoperative treatment for painful adolescent spondylolysis or spondylolisthesis, J Pediatr Orthop 9:538, 1989.
- Pizzutillo PD, Mirenda W, MacEwen GD: Posterolateral fusion for spondylolisthesis in adolescence, J Pediatr Orthop 6:311, 1986.
- Poussa M, Remes V, Lambert T, et al: Treatment of severe spondylolisthesis in adolescence with reduction or fusion in situ: long-term clinical, radiologic, and functional outcome, Spine 31:583, 2006.
- Poussa M, Schlenzka S, Seitsalo M, et al: Surgical treatment of severe isthmic spondylolisthesis in adolescents: reduction of fusion in situ, Spine 18:894, 1993.
- Rabushka SE, Apfelbach H, Love L: Spontaneous healing of spondylolysis of the fi fth lumbar vertebra: a case report, Clin Orthop Relat Res 93:259, 1973.
- Riley P, Gillespie R: Severe spondylolisthesis: results of posterolateral fusion, Orthop Trans 9:119, 1985.
- Roca J, Iborra M, Cavanilles-Walker JM, et al: Direct repair of spondylolysis using a new pedicle screw hook fi xation: clinical and CT-assessed study: an analysis of 19 patients, J Spinal Disord Tech 18(suppl):S82, 2005.
- Roca J, Moretta D, Fuster S, et al: Direct repair of spondylolysis, Clin Orthop Relat Res 246:86, 1989.
- Rombold C: Treatment of spondylolisthesis by posterolateral fusion, resection of the pars interarticularis, and prompt mobilization of the patient: an end-result study of seventy-three patients, J Bone Joint Surg 48A:1282, 1966.
- Rosenberg NJ, Bargar WL, Friedman B: The incidence of spondylolysis and spondylolisthesis in nonambulatory patients, Spine 6:35, 1981.
- Rosomoff HL: Lumbar spondylolisthesis: etiology of radiculopathy and role of the neurosurgeon, Clin Neurosurg 27:577, 1980.
- Salib RM, Pettine KA: Modifi ed repair of a defect in spondylolysis or minimal spondylolisthesis by pedicle screw, segmental wire fi xation, and bone grafting, Spine 18:440, 1993.
- Saraste H: Long-term clinical and radiological follow-up of spondylolysis and spondylolisthesis, J Pediatr Orthop 7:631, 1987.
- Scaglietti O, Frontino G, Bartolozzi P: Technique of anatomical reduction of lumbar spondylolisthesis and its surgical stabilization, Clin Orthop Relat Res 117:164, 1976.
- Schlegel K, Pon MA: The biomechanics of posterior lumbar interbody fusion (PLIF) in spondylolisthesis, Clin Orthop Relat Res 193:115, 1985.
- Schoenecker PL: Developmental spondylolisthesis without lysis. In Bridwell KH, DeWald RL, eds: The textbook of spinal surgery, 2nd ed, Philadelphia, 1997, Lippincott-Raven. Schoenecker PL, Cole HO, Herring JA, et al: Cauda equina syndrome after in situ arthrodesis for severe spondylolisthesis at the lumbosacral junction, J Bone Joint Surg 72A:369, 1990.
- Seitsalo S: Operative and conservative treatment of moderate spondylolisthesis in young patients, J Bone Joint Surg 72B:908, 1990.
- Seitsalo S, Osterman K, Hyvarinen H, et al: Severe spondylolisthesis in children and adolescents: a long-term review of fusion in situ , J Bone Joint Surg 72B:259, 1990.
- Seitsalo S, Osterman K, Hyvarinen H, et al: Progression of spondylolisthesis in children and adolescents: a long-term follow-up of 272 patients, Spine 16:417, 1991.
- Seitsalo S, Osterman K, Poussa M: Scoliosis associated with lumbar spondylolisthesis: a clinical survey of 190 young patients, Spine 13:899, 1988.
- Seitsalo S, Osterman K, Poussa M, et al: Spondylolisthesis in children under 12 years of age: long-term results of 56 patients treated conservatively or operatively, J Pediatr Orthop 8:516, 1988.
- Sevastikoglou JA, Spangfort E, Aaro S: Operative treatment of spondylolisthesis in children and adolescents with tight hamstrings syndrome, Clin Orthop Relat Res 147:192, 1980.
- Sherman FC, Rosenthal RK, Hall JE: Spine fusion for spondylolysis and spondylolisthesis in children, Spine 4:59, 1979.
- Shuffl ebarger HL, Geck MJ: High-grade isthmic dysplastic spondylolisthesis: monosegmental surgical treatment, Spine 30:S42, 2005.
- Sijbrandij S: A new technique for the reduction and stabilisation of severe spondylolisthesis: a report of two cases, J Bone Joint Surg 63B:266, 1981.
- Sijbrandij S: Reduction and stabilisation of severe spondylolisthesis: a report of three cases, J Bone Joint Surg 65B:40, 1983.
- Stanton RP, Meehan P, Lovell WW: Surgical fusion in childhood spondylolisthesis, J Pediatr Orthop 5:411, 1985.
- Steffee AD, Sitkowski DJ: Reduction and stabilization of grade IV spondylolisthesis, Clin Orthop Relat Res 227:82, 1988.
- Szappanos L, Szepesi K, Thomazy V: Spondylolysis in osteopetrosis, J Bone Joint Surg 70B:428, 1988.
- Taddonio RF: Isthmic spondylolisthesis. In Bridwell KH, DeWald RL, eds: The textbook of spinal surgery, Philadelphia, 1991, JB Lippincott. Takeda M: A newly devised “three-one” method for the surgical treatment of spondylolysis and spondylolisthesis, Clin Orthop Relat Res 147:228, 1980.
- Tower SS, Prat WB: Spondylolysis and associated spondylolisthesis in Eskimo and Athabascan populations, Clin Orthop Relat Res 250:171, 1990.
- Transfelt EE, Dendrinos GK, Bradford DS: Paresis of proximal lumbar roots after reduction of L5-S1 spondylolisthesis, Spine 14:884, 1988.
- Turner RH, Bianco AJ Jr: Spondylolysis and spondylolisthesis in children and teen-agers, J Bone Joint Surg 53A:1298, 1971.
- van Dam DE: Nonoperative treatment and surgical repair of lumbar spondylolysis. In Bridwell KH, DeWald RL, eds: The textbook of spinal surgery, 2nd ed, Philadelphia, 1997, Lippincott-Raven. van den Oever M, Merrick MV, Scott JHS: Bone scintigraphy in symptomatic spondylolysis, J Bone Joint Surg 69B:453, 1987.
- Velikas EP, Blackburne JS: Surgical treatment of spondylolisthesis in children and adolescents, J Bone Joint Surg 63B:67, 1981.
- Vidal J, Fassio B, Buscauret C, et al: Surgical reduction of spondylolisthesis using a posterior approach, Clin Orthop Relat Res 154:156, 1981.
- Warner WC: Kyphosis. In Morrissy RT, Weinstein SL, eds: Lovell and Winter’s pediatric orthopaedics, 6th ed, Philadelphia, 2006, Lippincott Williams & Wilkins. Wertzberger KL, Peterson HA: Acquired spondylolysis and spondylolisthesis in the young child, Spine 5:437, 1980.
- Wiltse LL, Bateman JG, Hutchinson RH, et al: The paraspinal sacrospinalis-splitting approach to the lumbar spine, J Bone Joint Surg 50A:919, 1968.
- Wiltse LL, Jackson DW: Treatment of spondylolisthesis and spondylolysis in children, Clin Orthop Relat Res 117:92, 1976.
- Wiltse LL, Newman PH, Macnab I: Classifi cation of spondylolysis and spondylolisthesis, Clin Orthop Relat Res 117:23, 1976.
- Wimberly RL, Lauerman WC: Spondylolisthesis in the athlete, Clin Sports Med 21:133, 2002.
- Kyphoscoliosis in
