INTRODUCTION TO ADVANCED ELBOW ARTHROSCOPY
The evolution of elbow arthroscopy has transitioned the modality from a purely diagnostic tool to a highly efficacious therapeutic intervention for a myriad of complex intraarticular pathologies. The constrained osseous anatomy of the ulnohumeral and radiocapitellar joints, combined with the intimate proximity of major neurovascular structures, demands a rigorous understanding of portal anatomy, fluid dynamics, and spatial orientation.
This comprehensive guide details the surgical techniques, biomechanical considerations, and postoperative protocols for arthroscopic synovectomy, arthroscopic tennis elbow and contracture release, the management of recalcitrant olecranon bursitis, and arthroscopic-assisted intraarticular fracture care.
ARTHROSCOPIC SYNOVECTOMY
Arthroscopic synovectomy is a highly effective joint-preserving procedure indicated for patients suffering from rheumatoid arthritis, primary synovial chondromatosis, pigmented villonodular synovitis (PVNS), hemophilic arthropathy, and other inflammatory arthritides. When medical management and disease-modifying antirheumatic drugs (DMARDs) fail to control localized synovial hypertrophy, surgical intervention is warranted to prevent progressive articular cartilage destruction and secondary osteoarthritis.
Pathoanatomy and Indications
In inflammatory conditions, the hypertrophic synovium acts as a locally destructive tissue, releasing proteolytic enzymes and cytokines that degrade the chondral surface. The elbow is particularly susceptible to stiffness secondary to capsular fibrosis induced by chronic inflammation. Arthroscopic synovectomy allows for near-total removal of the diseased synovium while minimizing the surgical trauma and subsequent arthrofibrosis associated with open arthrotomy.
Surgical Technique
Arthroscopic synovectomy is performed utilizing a systematic approach through all standard elbow portals (proximal anteromedial, anterolateral, posterolateral, and direct posterior) to ensure complete compartmental clearance.
- Anterior Compartment Clearance: The arthroscope is initially introduced through the proximal anteromedial portal. An aggressive full-radius shaver is introduced via the anterolateral portal to resect the hypertrophic synovium overlying the radiocapitellar joint and the anterior capsule.
- Posterior Compartment Clearance: The scope is then transitioned to the posterolateral portal, allowing visualization of the olecranon fossa, posterior radiocapitellar articulation, and the medial/lateral gutters.
- Loose Body Retrieval: In cases of synovial chondromatosis or advanced osteoarthritis, loose bodies are frequently encountered and must be systematically extracted.
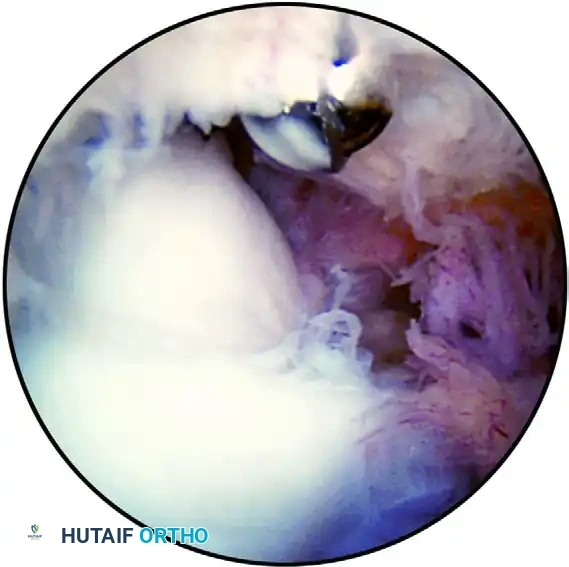
FIGURE 52-71 Extensive synovitis of the anterior compartment in a retired Major League pitcher presenting with persistent pain, popping, and swelling of the elbow. A partial synovectomy and removal of loose bodies were successfully performed.
Surgical Pearl: Fluid Management
Maintain arthroscopic pump pressures at the lowest possible setting (typically 30-40 mm Hg) to minimize fluid extravasation into the surrounding soft tissues, which can rapidly lead to compartment syndrome of the forearm.
ARTHROSCOPIC TENNIS ELBOW RELEASE AND CONTRACTURE MANAGEMENT
Posttraumatic arthrofibrosis and degenerative contractures of the elbow present significant functional limitations. The arthroscopic release technique described by Baker and Cummings provides a minimally invasive solution to restore the arc of motion by addressing both soft tissue contractures and osseous impingement.
Patient Positioning and Setup
- Anesthesia and Positioning: Following endotracheal intubation and the administration of a regional block (if not contraindicated by the need for immediate postoperative neurologic assessment), the patient is placed in the prone position on the operating table.
- Arm Support: Place two rolled towels longitudinally under the arm to provide a stable platform, allowing the elbow to flex and extend freely over the edge of the bolster. The prone position is highly advantageous as it allows gravity to assist in maintaining the arm position and provides excellent, unobstructed access to the posterior compartment.
Surgical Technique (Baker and Cummings)
The procedure requires a meticulous, step-wise approach to release fibrotic tissue while strictly avoiding iatrogenic neurovascular injury.
- Olecranon Fossa Preparation: Begin by resecting the dense scar tissue from the olecranon fossa to improve baseline visibility. This is critical, as the posterior compartment is often obliterated by fibrotic tissue in the stiff elbow.
- Portal Transition: Change the arthroscope to the posterolateral portal. Place the resector or arthroscopic burr through the direct posterior portal to complete the posterior debridement.
- Contracture Release: Carefully release the posterior capsular contracture utilizing a full-radius resector. Employ blunt mobilization techniques (using the shaver sheath without suction/blades active) to safely release the posterolateral and posteromedial gutters.
- Osseous Decompression: Use an arthroscopic osteotome to resect any osteophyte formation or impingement of the olecranon tip within the olecranon fossa. Complete the precise resection and contouring with an arthroscopic burr. To relieve bony hypertrophy creating impingement, systematically enlarge the olecranon fossa with the burr to accommodate the olecranon tip during terminal extension.
🚨 SURGICAL WARNING: ULNAR NERVE PROXIMITY
Do NOT use the mechanical shaver or thermal ablation devices in the deep posteromedial gutter without direct visualization of the capsular boundary. The ulnar nerve lies in extremely close proximity medially. Iatrogenic transection or thermal injury to the ulnar nerve is a catastrophic complication.
Medial Exposure and Ulnar Nerve Protection
If extensive posteromedial work is required, or if the surgeon wishes to expose the ulnar nerve to ensure its absolute protection:
- Create a posterior retractor portal approximately 2 cm proximal to the direct posterior portal.
- Introduce a small retractor-elevator through this accessory portal.
- This instrument can be used to gently retract the medial capsule and soft tissues away from the joint space, increasing visualization and providing a physical barrier to prevent any injury to the ulnar nerve during burring or shaving. Alternatively, a small open medial incision can be utilized to formally decompress and protect the nerve.
Closure and Splinting
- Upon completion of the release, place a surgical drain in the direct posterior portal to prevent postoperative hematoma formation, which can act as a scaffold for recurrent fibrosis.
- Close the portals with non-absorbable nylon sutures.
- While the patient is still under anesthesia, gently manipulate the elbow to confirm the newly gained maximal arc of motion.
- Splint the elbow in maximal extension, as extension is typically the most difficult motion to regain and maintain postoperatively.
POSTOPERATIVE REHABILITATION PROTOCOL
The success of an arthroscopic contracture release is heavily dependent on a rigorous, well-structured postoperative rehabilitation program. Without immediate and sustained physical therapy, the elbow will rapidly restiffen.
Phase I: Immediate Postoperative (0-24 Hours)
- The initial maximal extension splint is left in place for the first 24 hours to maintain the intraoperative gains and control initial hemorrhage.
- The surgical drain is typically removed on postoperative day 1.
Phase II: Early Motion and Bracing (Days 1-21)
- Range of Motion (ROM): Gentle active and active-assisted range-of-motion exercises of the elbow are initiated immediately after splint removal.
- Splinting: A custom-molded, removable extension splint is worn at all times between exercise periods and during sleep.
- Continuous Passive Motion (CPM): In patients with extensive posttraumatic arthrofibrosis and severe preoperative loss of flexion and extension, the use of an elbow CPM machine is highly recommended. The CPM should be utilized to maintain the arc of motion during the critical first 3 weeks after surgery.
- Static Progressive Bracing: At 1 week postoperatively, a static progressive brace, such as the Joint Active System (Joint Active Systems, Effingham, IL), is introduced. The patient utilizes the brace for 30 minutes, three times a day, alternating between maximal tolerated extension and flexion.
- Home Exercise Program: Active and passive ROM exercises are performed by the patient for 20 minutes, four to five times a day at home.
- Supervised Therapy: Formal, supervised physical therapy is continued three times a week to ensure compliance and perform joint mobilizations.
Pharmacologic Prophylaxis
An aggressive anti-inflammatory regimen is critical. A nonsteroidal anti-inflammatory drug (NSAID), such as Indomethacin or Celecoxib, is prescribed for the first 3 weeks. This serves a dual purpose: decreasing acute postoperative inflammation and mitigating the risk of heterotopic ossification (myositis ossificans), which is a known complication following extensive elbow capsular release.
MANAGEMENT OF OLECRANON BURSITIS
Olecranon bursitis is characterized by inflammation and fluid accumulation within the bursa overlying the olecranon process. While the majority of cases resolve with conservative management (compression, NSAIDs, aspiration, and corticosteroid injection), chronic recalcitrant cases require surgical intervention.
Open vs. Arthroscopic Bursectomy
Historically, chronic recalcitrant olecranon bursitis has been treated effectively with a small open excision. The open technique allows for complete en bloc resection of the thickened bursal sac.
In an attempt to circumvent the wound healing problems occasionally associated with open posterior elbow incisions, some surgeons have advocated for arthroscopic bursectomy. However, the literature presents significant concerns regarding this minimally invasive approach:
- Kerr's Study: Reported a 6-month follow-up of five patients undergoing arthroscopic bursectomy. Notably, a severe postoperative infection developed in one immunosuppressed patient.
- Savoie's Study: Reported on arthroscopic bursectomy in six patients, one of whom developed a chronic, draining portal fistula—a notoriously difficult complication to manage over the extensor surface of the elbow.
Clinical Consensus
Given the small number of studies supporting the arthroscopic technique, combined with complication rates (infection, fistulization) that are similar to or potentially worse than those reported for open techniques, the relative value of arthroscopic bursal resection remains highly questionable. At present, open excision remains the gold standard for recalcitrant olecranon bursitis, allowing for meticulous hemostasis and layered closure to eliminate dead space.
ARTHROSCOPIC-ASSISTED INTRAARTICULAR FRACTURE CARE
The application of arthroscopy in acute elbow trauma is an evolving frontier. While open reduction and internal fixation (ORIF) remains the standard of care for displaced intraarticular fractures, there are specific scenarios where arthroscopic-assisted evaluation and treatment offer distinct advantages.
Indications and Techniques
Arthroscopy is most beneficial in the management of localized, minimally displaced fractures or the retrieval of intraarticular fragments.
- Fragment Excision: Arthroscopy excels in the identification and removal of small, unfixable capitellar or radial head shear fragments that act as mechanical blocks to motion.
- Radial Head Resection: In cases of highly comminuted radial head fractures where arthroplasty is not indicated, arthroscopic radial head resection can be accomplished.
- Limited Internal Fixation: For larger, simple fracture patterns (e.g., Mason Type II radial head fractures or isolated capitellar fractures), arthroscopic visualization can assist in achieving anatomic reduction. Limited internal fixation can then be accomplished percutaneously using headless cannulated screws.
🚨 SURGICAL PITFALL: FLUID EXTRAVASATION IN TRAUMA
Arthroscopic radial head resection or fracture management should ONLY be attempted if a significant medial capsular injury has not occurred. A disrupted medial capsule provides a direct pathway for massive fluid extravasation into the forearm compartments.
Contraindications and Abort Criteria
In more extensive fractures involving significant soft tissue injuries, capsular tearing, or ligamentous disruption, the benefits of arthroscopy are vastly outweighed by the associated risks. The pressurized fluid required for arthroscopy can rapidly lead to acute compartment syndrome in the traumatized limb.
When contemplating arthroscopic fracture care, the surgeon must maintain a low threshold to convert to an open procedure. The arthroscopic approach must be immediately aborted if:
1. Visualization is poor due to persistent hemarthrosis.
2. Anatomic reduction cannot be definitively confirmed.
3. There is any clinical evidence of significant fluid extravasation into the forearm or upper arm.
