DEFINITION
Anacute paronychiais an infection of the soft tissue fold around the fingernail. It is the most common soft tissue infection of the hand.The most common infecting organism isStaphylococcus aureus, although these infections are commonly mixed infections.Achronic paronychiais characterized by repeated infection and inflammation of the eponychium.The eponychium becomes thickened and rounded.This problem often occurs in the setting of repeated and prolonged exposure to water.The most commonly isolated organisms areCandida albicans, gram-positive cocci, gram-negative rods, andMycobacteriumspp.Herpetic whitlow is caused by an outbreak of herpes simplex virus in the skin of the finger and can be confused with acute paronychia or felon.Herpetic whitlow is common in children and medical personnel who come into contact with oral secretions.Afelonis a tense abscess of the distal pulp of the finger or thumb that involves multiple septal compartments (FIG 1).
ANATOMY


FIG 1 • Felon in coronal and sagittal section.
PATHOGENESIS
Acute paronychia results from the introduction of bacteria into the space between the nail fold and the nail plate, either proximally or laterally.This commonly occurs as a result of a hangnail, nail biting, artificial nails, or an overzealous manicure.Chronic paronychia results from colonization and infection by organisms that enter the space between the nail plate and the cuticle, eponychium, and nail fold.Infection may result from repeated exposure to moisture.This chronic infection and inflammation lead to fibrosis of the eponychium, which, in turn, leads to decreased vascularity of the dorsal nail fold.This decreased vascularity predisposes to repeated bacterial insults, resulting in the characteristic clinical exacerbations.Felons often result from penetrating trauma or from bacterial inoculation through the exocrine sweat glands contained within the pulp.Cellulitis and local inflammation lead to local ischemia, which, in the setting of the closed spaces defined by septa, leads to increased pressure.Fat necrosis and abscess formation result from the increased pressure, which, in turn, causes a further increase in pressure and, in effect, a compartment syndrome.
NATURAL HISTORY
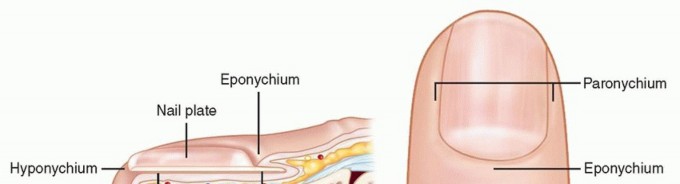
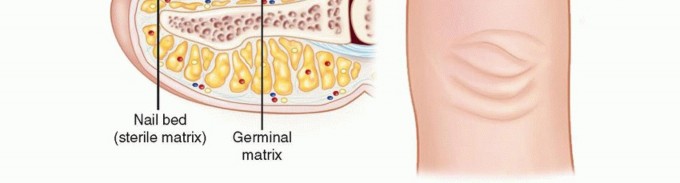
FIG 2 • Anatomy of the nail complex. Subsequent incision and drainage may lead to secondary bacterial infection.Chronic paronychia are characterized by induration of the eponychium punctuated by episodes of swelling and drainage.A felon, if left untreated, may lead to osteomyelitis or septic flexor tenosynovitis.
PATIENT HISTORY AND PHYSICAL FINDINGS
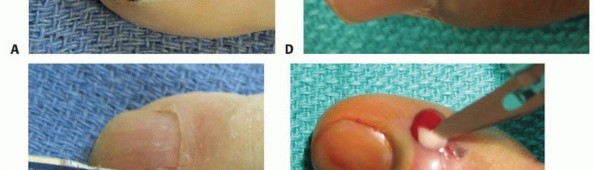
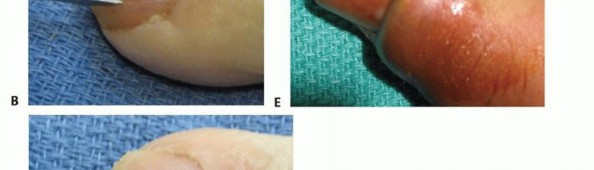
In acute paronychia, the patient will complain of swelling and pain immediately adjacent to the nail.If an abscess has formed, there may be erythema and purulent drainage.In chronic paronychia, the patient will present with a chronically indurated and rounded eponychium characterized by repeated episodes of inflammation and drainage.Herpetic whitlow is characterized by pain and swelling followed by the appearance of multiple vesicular lesions.The pain typically is out of proportion to the physical findings, and the fingertip is not tense (in contrast to a felon).A patient with a felon will present with severe throbbing pain, swelling, and a tense fingertip pad.A felon will not extend proximal to the distal interphalangeal (DIP) joint flexion crease unless it is associated with septic flexor tenosynovitis.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Radiographs are indicated to rule out osteomyelitis or if a foreign body is suspected.The diagnosis of herpetic whitlow is confirmed by Tzanck smear, which will show multinucleated giant cells.Patients suspected of having a systemic illness should have the appropriate laboratory workup.
DIFFERENTIAL DIAGNOSIS
Acute paronychia Chronic paronychia Herpetic whitlow Felon OsteomyelitisSeptic arthritis of the DIP joint
NONOPERATIVE MANAGEMENT
Acute paronychia may be treated with warm soaks and oral antibiotics if infection is caught early and if no significant abscess is present.Herpetic whitlow is managed by keeping the hands clean to prevent bacterial superinfections; these lesions will resolve on their own.Some recommend treatment with oral acyclovir, but multiple clinical trials have failed to show any definite benefit.Nonoperative treatment has no role in the treatment of chronic paronychia unless there is a concomitant fungal infection that may benefit from medical therapy.Given the rapid clinical progression of a felon, nonoperative treatment with antibiotics rarely will be successful, except in very early cases.
SURGICAL MANAGEMENT
If the abscess is superficial, drainage may sometimes be performed without anesthesia.If the infection is more extensive or involves both sides of the nail, incision and drainage should be performed under digital nerve block.Use lidocaine or a mixture of lidocaine and bupivacaine without epinephrine.Instillation of the medication at the level of the distal metacarpal from dorsal to volar is the safest and best tolerated technique.Chronic paronychia usually are treated with eponychial marsupialization.Chronic paronychia associated with underlying fungal infections may be amenable to more standard surgical treatments as performed for acute paronychia after the fungal infection has been successfully treated medically.Herpetic whitlow is treated with incision and drainageonlyif a bacterial superinfection has occurred.
POSITIONING
The patient is placed in the supine position with a standard hand table and either digital or forearm tourniquet.P.1161
APPROACH
The surgical approach is dictated by the location of the infection. Infection under the nail plate will require elevation of part of the nail.Infection under the eponychial fold will require elevation of the eponychium. Infection into the pulp will require incision deep into the pulp space.
TECHNIQUE
Incision and Drainage of an Acute Paronychia
Incision and Drainage of an Acute Paronychia
SINGLE INCISION


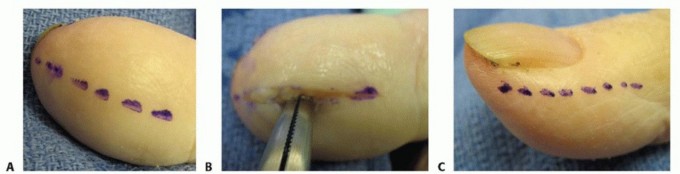
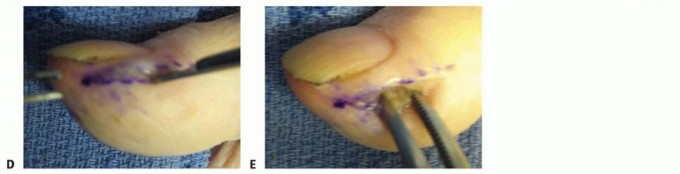
TECH FIG 1 • A. Incision to drain the paronychia. B,C. Incision and removal of a portion of the nail plate. D,E. Alternative incision to drain the paronychia. If the abscess extends to the eponychium, the incision may be carried as far proximally as necessary; a portion of nail may then be removed if necessary.Avoid making an incision across the eponychium, as this may result in a late nail fold deformity.
PARALLEL INCISIONS



TECH FIG 2 • Incision (A) and elevation of the eponychial fold (B,C) with removal of the proximal nail to decompress a proximal abscess. D. The wound is packed with gauze to prevent premature closure.
Eponychial Marsupialization for a Chronic Paronychia


TECH FIG 3 • A,B. Incision for marsupialization of chronic paronychia. C. Tissue removed with the underlying germinal matrix exposed.
TECH FIG 4 • A. Midvolar approach for drainage of a felon. B. Spread deeply with a hemostat to disrupt all septa. C,D. Lateral incision for drainage of a felon. E. Spread deeply with a hemostat to disrupt all septa. Carry the incision deep enough to disrupt all involved septa or spread with a hemostat (TECH FIG 4D,E).Avoid proximal probing to avoid the spread of infection to the flexor sheath.Irrigate the wound with normal saline.Place a strip of gauze into the open wound to allow for drainage, and dress appropriately.PEARLS AND PITFALLS
|Misdiagnosis ▪ Avoid misdiagnosis of herpetic whitlow as an acute paronychia with concomitant overtreatment of this problem resulting in a secondary bacterial infection and no improvement in the herpetic whitlow.1. Recognize underlying osteomyelitis in long-standing cases.2. Recognize any systemic illness that may hinder resolution of the infection.3. Chronic paronychia: Avoid missing a cyst, tumor, or associated fungal infection.||Technique ▪Acute paronychia:Determine whether purulence is present under the nail plateor extending into the pulp. Avoid incising into the sterile matrix by keeping the blade turned away from the nail bed.1.Chronic paronychia: Excise tissue superficial to the germinal matrix; avoid damaging the germinal matrix.2.Felon: Base the incision on the location of maximal tenderness. With a lateral incision, avoid damaging the digital nerve branches by remaining within 3 mm of the lateral edge of the nail. With a volar incision, do not cross the DIP joint flexion crease and avoid incising the flexor tendon sheath. Such incisions may lead to septic tenosynovitis.Postoperative ▪Acute paronychia and felons:Treat with 10 days of oral antibiotics. Use of a care removable splint over the distal digit is valuable early in recovery for patientcomfort. Encourage early digital range-of-motion exercises during daily soaks.3.Chronic paronychia: Failure to modify environmental factors and treat systemic disease may lead to recurrence.|------P.1164
POSTOPERATIVE CARE
Acute paronychia and felonsOral antibiotics should be started postoperatively.Soaks in a dilute solution of either chlorhexidine or povidone-iodine may be started on postoperative day 2 and continued until wound healing is completed. The packing is removed when the soaks begin.Begin early range-of-motion exercises to avoid stiffness.Chronic paronychiaOral antibiotics usually are not necessary.Soaks in a dilute solution of either chlorhexidine or povidone-iodine may be started on postoperative day 2 and continued until wound healing is completed.Correction of environmental factors or systemic illness is critical.Begin early range-of-motion exercises to avoid stiffness.
COMPLICATIONS
Recurrent infection (systemic spread of the infection) Incisional tenderness (pulp)Digital nerve injury Decreased sensation NeuromaOsteomyelitisNail plate deformity
SUGGESTED READINGS
- Bednar MS, Lane LB. Eponychial marsupialization and nail removal for surgical treatment of chronic paronychia. J Hand Surg Am 1991;16:314-317.
- Canales FL, Newmeyer WL III, Kilgore ES Jr. The treatment of felons and paronychias. Hand Clin 1989;5:515-523.
- Franko OI, Abrams RA. Hand infections. Orthop Clin North Am 2013;44(4):625-634.
- Gill MJ, Arlette J, Buchan K. Herpes simplex virus infection of the hand. A profile of 79 cases. Am J Med 1988;84:89-93.
- Hausman MR, Lisser SP. Hand infections. Orthop Clin North Am 1992;23:171-185.
- Jebson PJ. Infections of the fingertip. Paronychias and felons. Hand Clin 1998;14:547-555.
- Kesson AM. Use of acyclovir in herpes simplex virus infections. J Paediatr Child Health 1998;34:9-13.
