Introduction to Upper Extremity Limb Salvage
In contrast to the lower extremity, where modern prosthetics can closely mimic the biomechanics of the native limb, even the most advanced artificial limb fails to provide comparable function in the upper extremity. The lack of sensory feedback, fine motor control, and spatial proprioception makes upper extremity amputation a profoundly disabling procedure. Consequently, modern imaging and surgical techniques prioritize limb salvage in almost all oncologic circumstances.
Resections of the proximal humerus frequently require the sacrifice of the axillary nerve, and resections of the humeral shaft frequently necessitate the sacrifice of the radial nerve. Remarkably, even with the sacrifice of up to three major nerves, limb salvage usually provides superior functional outcomes compared to an artificial limb. If the median or ulnar nerve must be sacrificed, limb salvage may still be highly worthwhile provided that functioning muscles are available for tendon transfers to restore grip and pinch.
Surgical Warning: One absolute indication for amputation in the upper extremity is extensive, un-reconstructible neurovascular involvement that precludes a functional, sensate hand. A displaced pathological fracture with massive soft-tissue contamination may also serve as a relative indication for amputation, depending on the tumor grade and compartment breach.
Pediatric Considerations: Noninvasive Expandable Prostheses
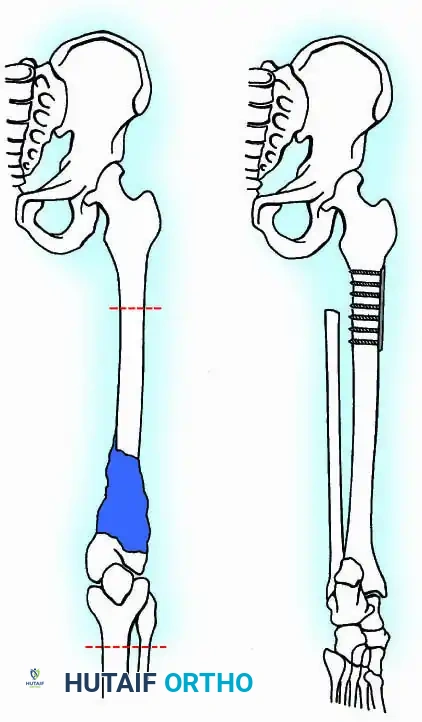
In skeletally immature patients requiring massive bone resection for osteosarcoma or Ewing sarcoma, limb length discrepancy is a major postoperative complication. The development of noninvasive expandable prostheses, such as the Repiphysis system, has revolutionized pediatric limb salvage.
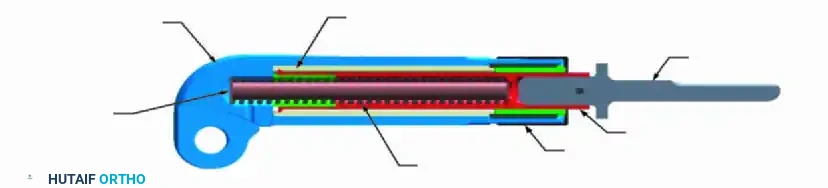
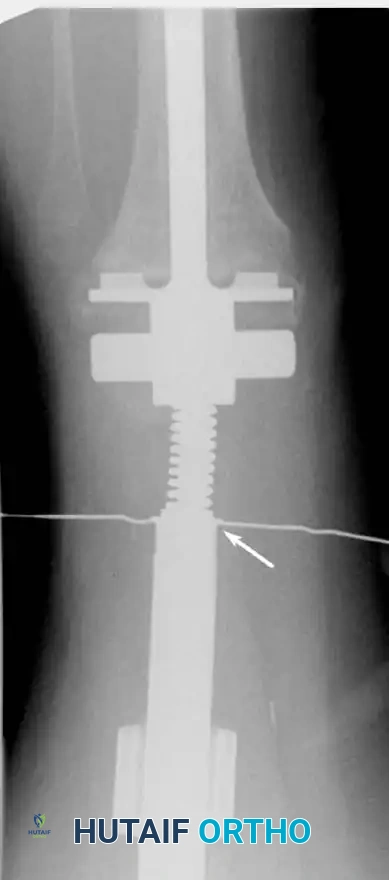
These devices utilize an electromagnetic field to release a locking mechanism within the prosthesis, allowing a compressed spring to expand the tubular housing. This permits incremental lengthening in the outpatient clinic without the need for repeated surgical interventions.



The Repiphysis Lengthening Procedure
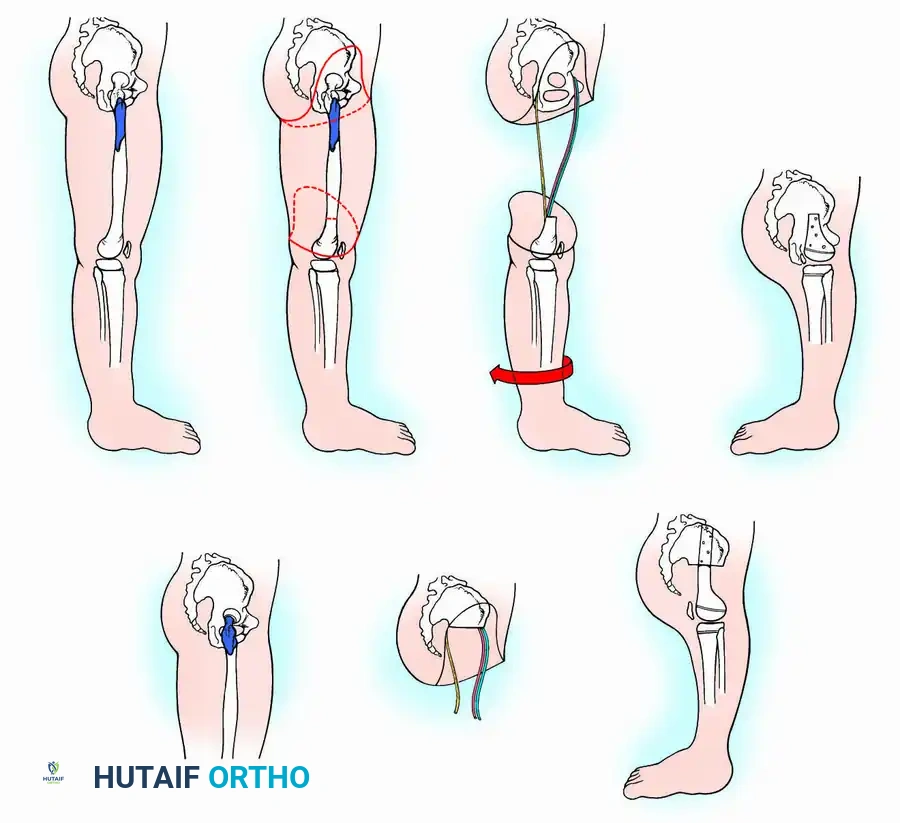
The lengthening process is meticulously controlled:
1. The locking mechanism is located via palpation or fluoroscopy.
2. The patient’s limb is marked at the exact site of the internal mechanism.
3. An electromagnetic coil is placed circumferentially around the limb at the marked level.
4. The device is activated, generating a field that releases the internal spring.
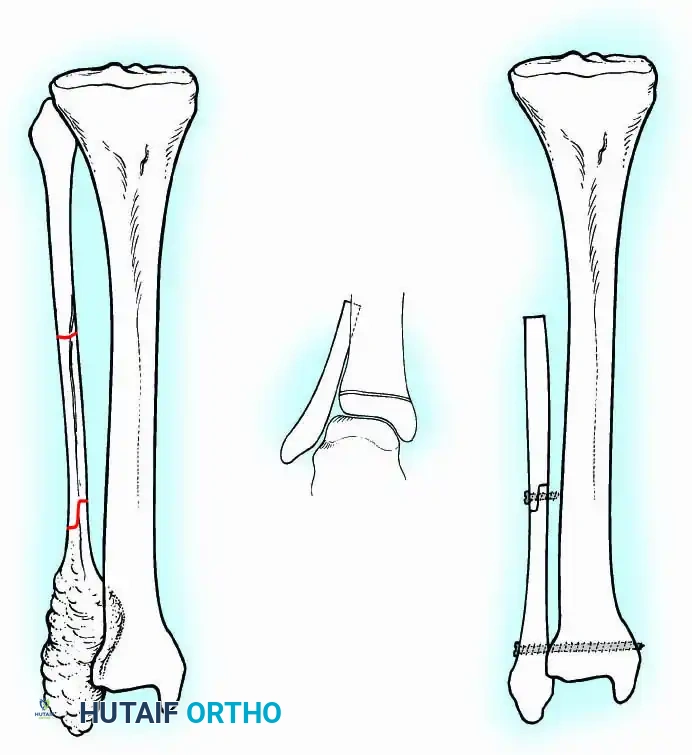
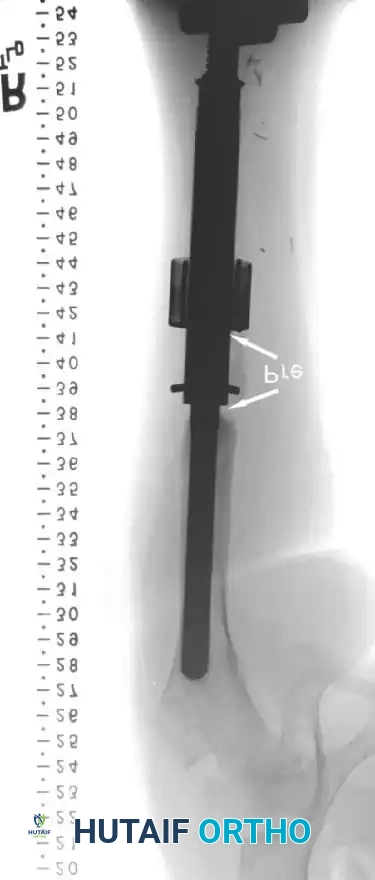
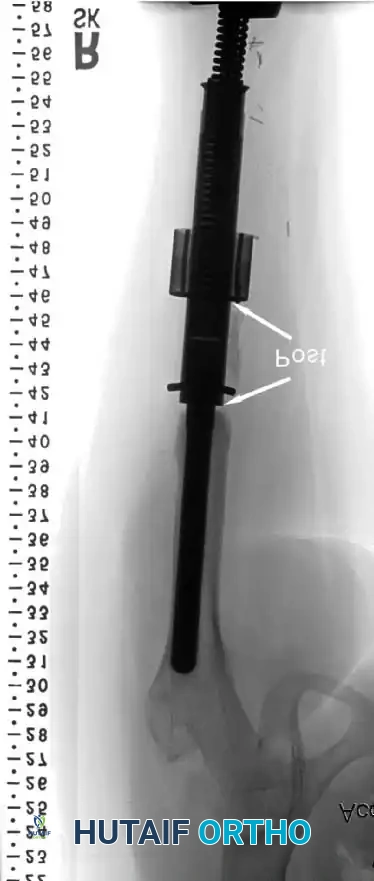
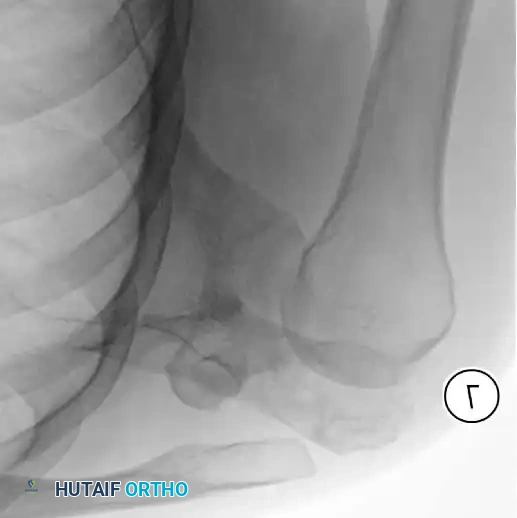
5. Pre-expansion and post-expansion radiographs are obtained to quantify the exact lengthening achieved.





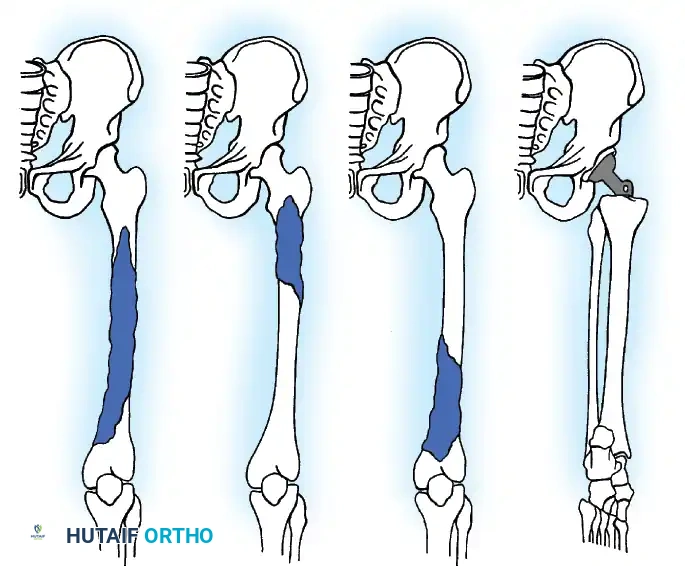
Classification of Shoulder Girdle Resections
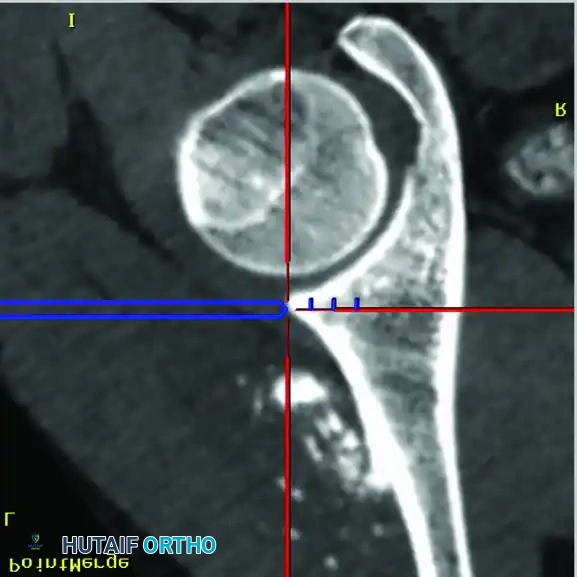
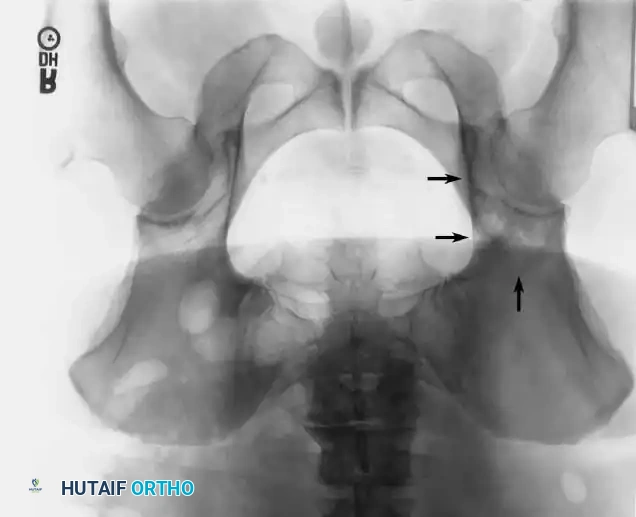
Tumors of the scapula are frequently complicated by extension into the glenohumeral joint, necessitating extra-articular resection of the humeral head en bloc with the scapula. Likewise, the long head of the biceps tendon provides a direct anatomical passageway for tumors of the proximal humerus to extend into the joint, often requiring an extra-articular partial scapulectomy.
To standardize terminology and allow for meaningful comparison of oncologic and functional results, Malawer et al. proposed a comprehensive classification system. This system is based strictly on the anatomical structures removed, reflecting the relationship to the glenohumeral joint and the status of the abductor mechanism.
The Malawer Classification System
- Type I: Intra-articular proximal humeral resection.
- Type II: Partial scapular resection.
- Type III: Intra-articular total scapulectomy.
- Type IV: Extra-articular total scapulectomy and humeral head resection.
- Type V: Extra-articular humeral head resection.
- Type VI: Extra-articular humeral and total scapular resection.
Each type is further subdivided based on the status of the abductor mechanism (deltoid and rotator cuff):
* A: Abductor mechanism intact.
* B: Partial or complete resection of the abductor mechanism.


Surgical Technique: Resection of the Shoulder Girdle (Tikhoff-Linberg Procedure)
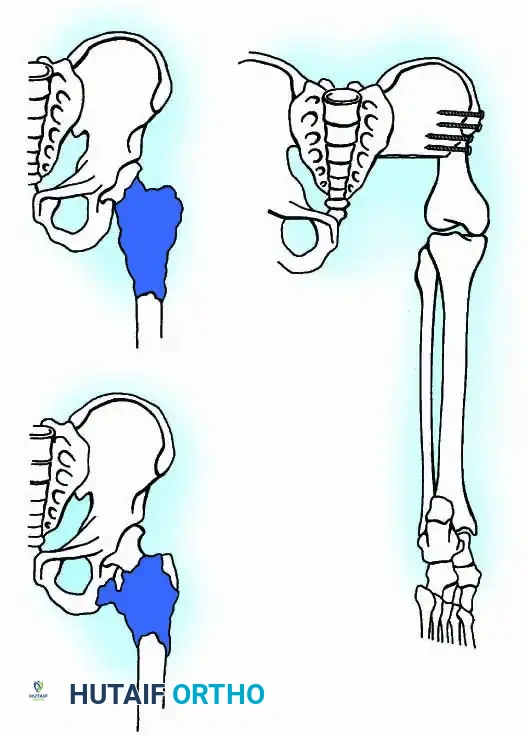
The Tikhoff-Linberg procedure is a massive resection of the shoulder girdle consisting of total scapulectomy, partial or complete excision of the clavicle, and excision of the proximal humerus. It is indicated for high-grade malignant tumors around the shoulder where a sufficient margin of normal tissue exists to clear the neurovascular bundle.
🔪 Surgical Technique 19-1: Marcove, Lewis, and Huvos Approach
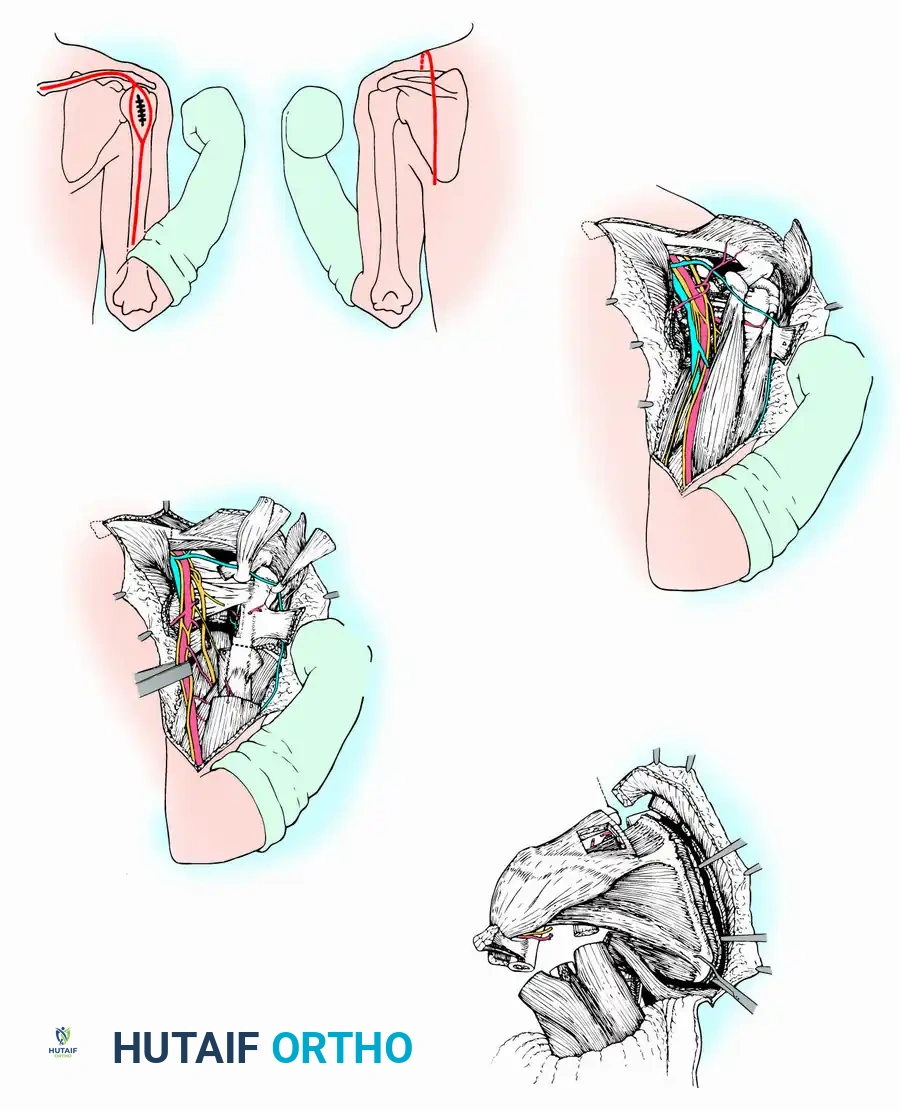
1. Incision and Exposure:
* Make an incision extending from the medial end of the clavicle along the medial two-thirds of the bone, curving inferiorly over the coracoid process, and continuing along the medial aspect of the arm.
* From the midpoint of this anterior incision, make a posterior longitudinal extension along the middle of the scapula down to its inferior angle.
* Incise the deltoid and pectoralis major and minor inferior to the clavicle and medial to the coracoid.
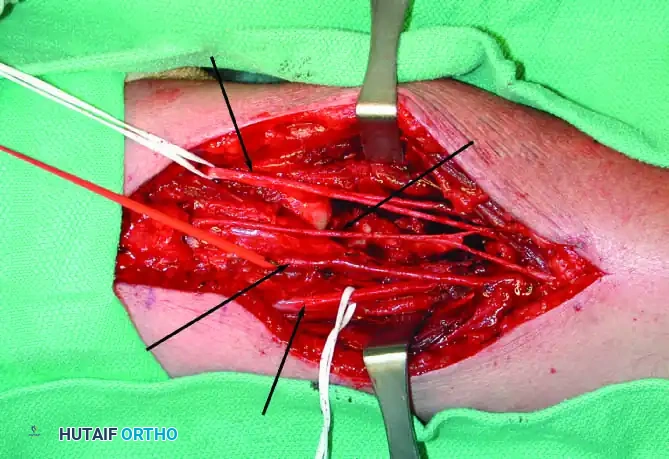
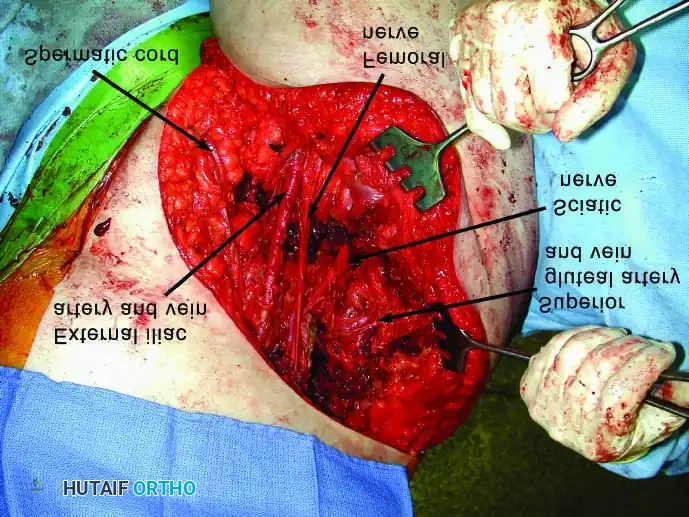
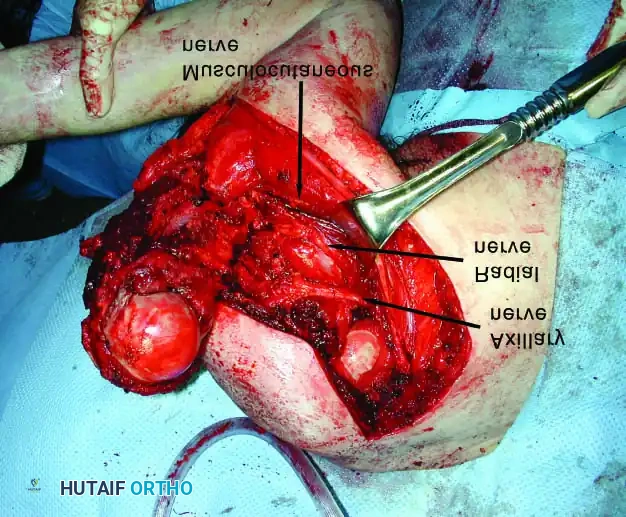
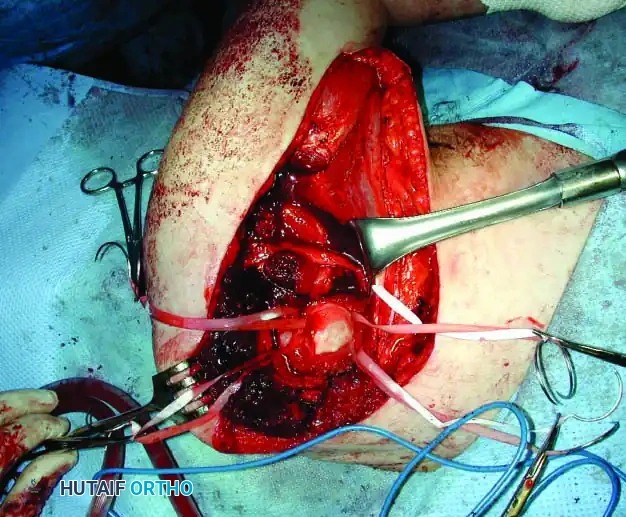
2. Neurovascular Dissection:
* Ligate the cephalic vein to expose the axillary vessels and the brachial plexus.
* Meticulously determine that the neurovascular bundle is not involved by the tumor.
* Ligate the anterior and posterior humeral circumflex vessels, and gently retract the axillary vessels medially. If oncologic margins dictate, sacrifice the radial and musculocutaneous nerves.
3. Muscular Division and Osteotomy:
* Divide the coracobrachialis, short head of the biceps, triceps, teres major, and latissimus dorsi muscles well away from the tumor pseudocapsule.
* Osteotomize the medial end of the clavicle using a Gigli saw or oscillating saw.
* Develop the posterior extension of the incision. Mobilize the inferior angle and vertebral border of the scapula by dividing the latissimus dorsi, trapezius, rhomboids, and levator scapulae muscles.
4. Scapular Mobilization and Resection:
* Maintain wide soft-tissue margins. If the lesion is isolated to the proximal humerus, a scapular osteotomy can be made at the level of the base of the coracoid, sparing the body of the scapula.
* Raise a lateral skin flap over the upper arm, leaving the deltoid muscle en bloc with the specimen.
* Complete the mobilization of the scapula by dividing the omohyoid and serratus anterior muscles. Divide and ligate the suprascapular, subscapular, and transverse cervical vessels.
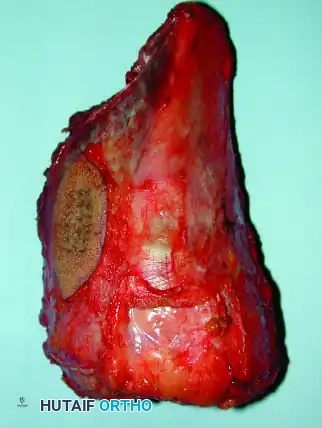
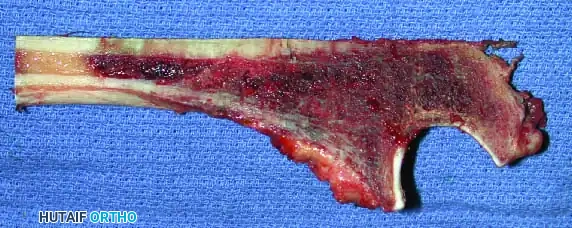
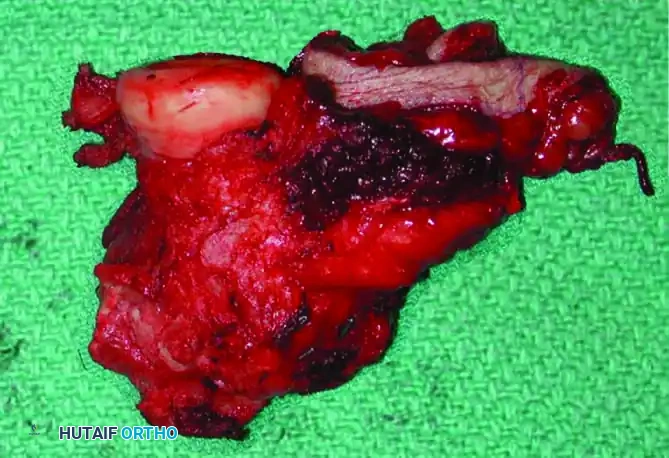
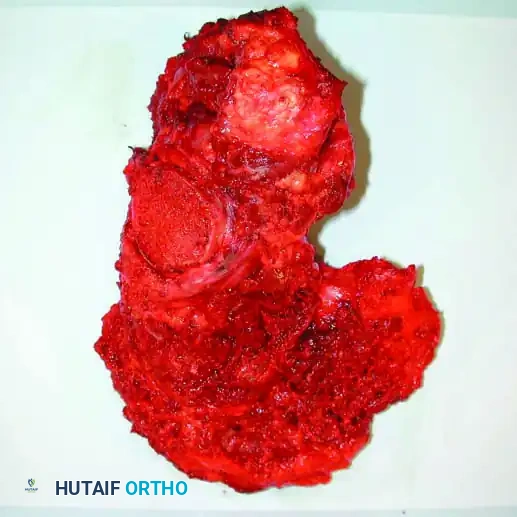
* Osteotomize the humerus at the preoperatively determined level and remove the specimen en bloc. Confirm adequate margins via frozen section analysis.

5. Reconstruction and Closure:
* Reattach the remaining biceps and triceps to the trapezius, pectoralis major, and latissimus dorsi to provide soft-tissue suspension.
* Insert a modular humeral megaprosthesis into the remaining humeral shaft. Suspend the proximal end of the prosthesis to the second rib or the remaining clavicular stump using heavy non-absorbable sutures or synthetic mesh.
* Close the wound in layers over closed-suction drains and apply a rigid shoulder immobilizer.
Surgical Technique: Resection of the Scapula (Scapulectomy)
Parts of the scapula, varying from a small segment to the entire body, can be resected for benign aggressive tumors, malignant sarcomas, or chronic recalcitrant infection. The subscapularis muscle often provides a robust anatomical barrier, protecting tumors of the scapula from direct chest wall invasion until late in the disease process.
After an isolated scapulectomy, the shoulder remains surprisingly stable and functional because the acromion, glenoid, and coracoid are undisturbed, allowing the humerus to remain in a nearly normal anatomical position.
🔪 Surgical Technique 19-2: Total or Partial Scapulectomy
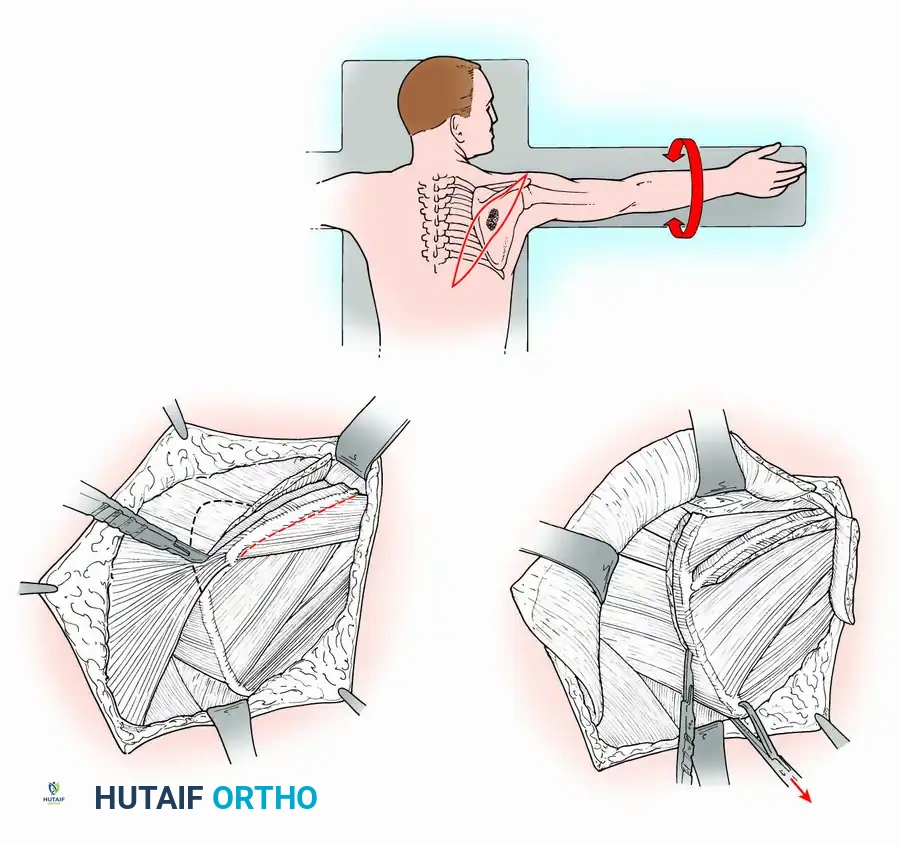
1. Positioning and Incision:
* Place the patient in the prone or lateral decubitus position with the arm resting in 90 degrees of abduction on a sterile arm board. Drape the arm free to allow dynamic manipulation during the procedure.
* Make an elliptical skin incision encompassing the biopsy tract and the tumor, extending from the tip of the acromion superolaterally to the paravertebral region inferomedially.


2. Muscular Dissection:
* Raise medial and lateral skin flaps full-thickness down to the investing fascia.
* Divide the attachment of the trapezius muscle to the scapular spine and retract the muscle superomedially to expose the supraspinatus.
* Divide the attachment of the deltoid muscle to the acromion.
* Divide the attachment of the latissimus dorsi to the inferior angle of the scapula and retract it inferiorly.
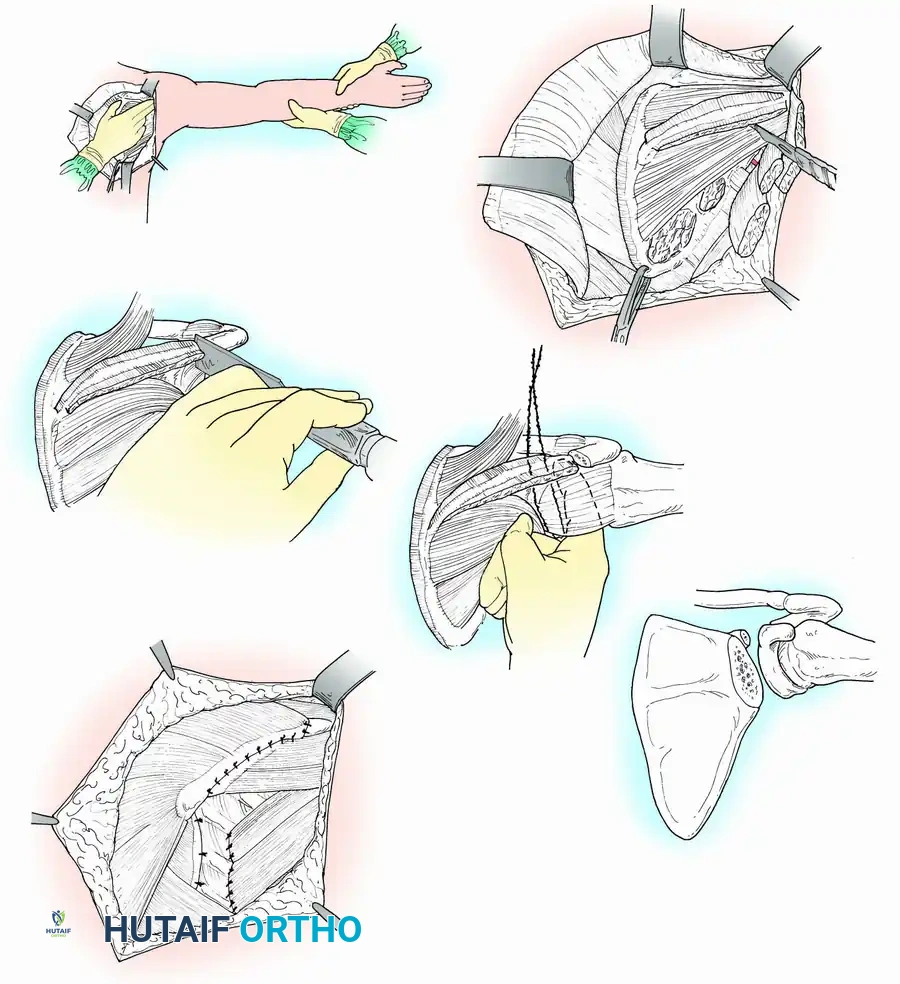
3. Scapular Mobilization:
* Apply traction to the inferior angle of the scapula with a heavy towel clip. Divide the muscles attached to the vertebral border (rhomboids) and the levator scapulae at the superior angle.
* Rotate the scapula and abduct the arm, permitting the axillary contents to fall away and be safely retracted out of the operative field.
* Divide the teres major, teres minor, and the long head of the triceps, followed by the supraspinatus and infraspinatus tendons, and finally the serratus anterior.



4. Osteotomy and Specimen Removal:
* Expose the shoulder joint and divide the scapular spine near the acromion using a sharp osteotome.
* Divide the subscapularis. Pass a Gigli saw around the neck of the scapula, taking extreme care to avoid breaching the glenohumeral joint capsule, and divide the scapular neck to remove the specimen en bloc.
5. Closure and Aftertreatment:
* Obtain meticulous hemostasis. Approximate the trapezius and deltoid muscles to recreate the shoulder contour and provide suspension.
* Suture the teres major and minor muscles to the chest wall fascia.
* Insert suction drains and close the wound. Apply a shoulder immobilizer.
* Postoperative Protocol: The immobilizer is removed after 48 hours, transitioning to a simple sling. Active and active-assisted exercises of the elbow, wrist, and hand are begun immediately. Shoulder mobilization begins as soft-tissue healing permits, usually at 3-4 weeks.
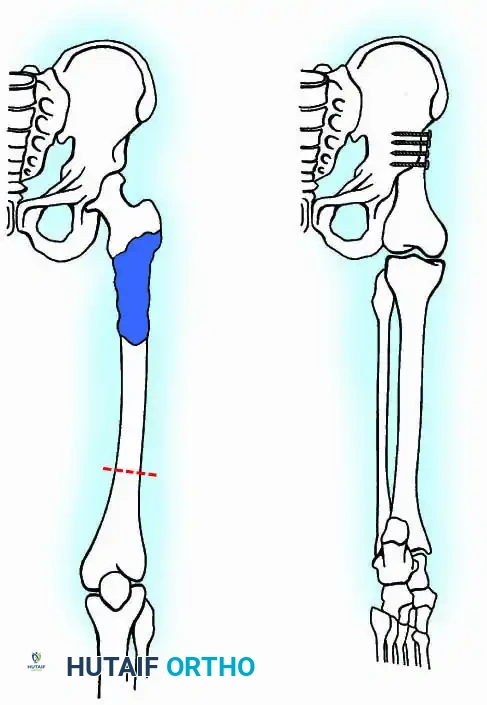
Surgical Technique: Resection of the Proximal Humerus
Biopsy of a proximal humeral lesion must be performed through the anterior third of the deltoid, taking absolute care not to contaminate the deltopectoral interval. Contamination of this interval allows tumor cells to spread along the neurovascular bundle, making a successful limb-sparing resection exponentially more difficult and increasing the risk of local recurrence.
Resection of the proximal humerus with its contiguous soft tissues usually achieves satisfactory oncologic margins for high-grade sarcomas, aggressive benign neoplasms (e.g., giant cell tumors), and metastatic carcinomas.
Reconstructive Alternatives
Following resection, reconstructive options include:
1. Flail Shoulder: Rarely indicated, reserved for patients with massive soft tissue loss where suspension is impossible.
2. Passive Spacer: Utilized in severe infections or as a temporary bridge.
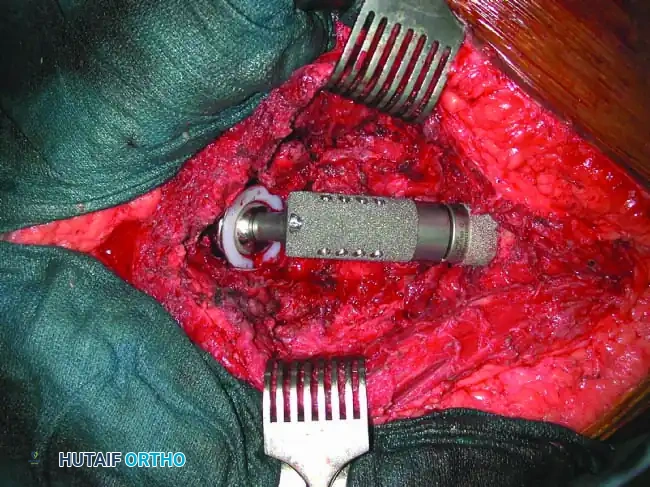
3. Endoprosthetic Arthroplasty: Modular megaprostheses offer immediate stability and rapid rehabilitation.
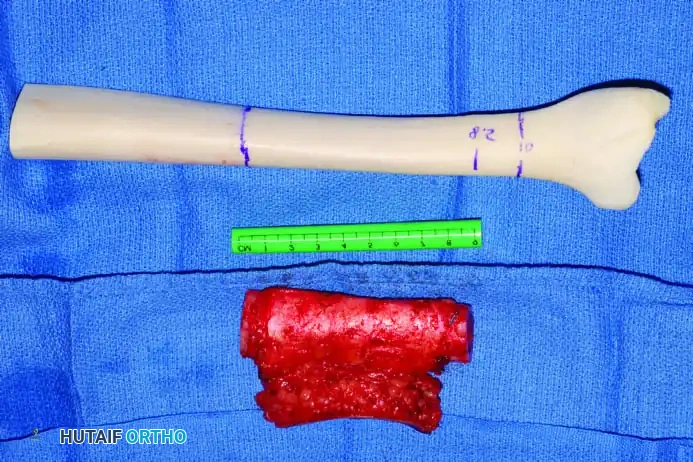
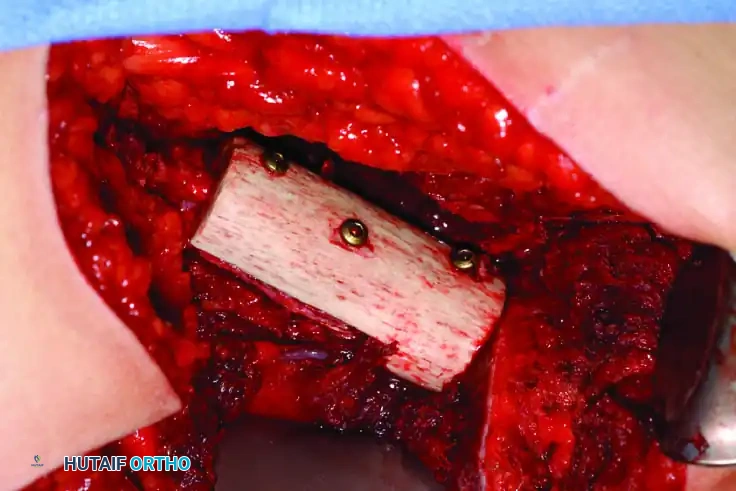
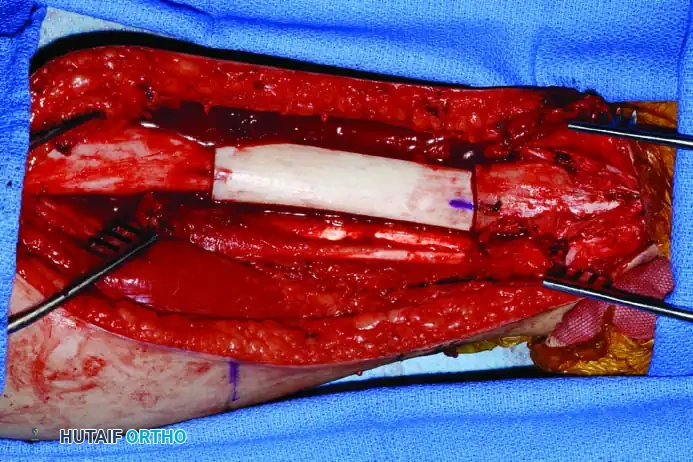
4. Allograft-Prosthetic Composite (APC): Combines the immediate fixation of a prosthesis with the biologic soft-tissue attachment potential of an allograft.
5. Arthrodesis: Provides a stable, powerful shoulder but sacrifices all glenohumeral motion.

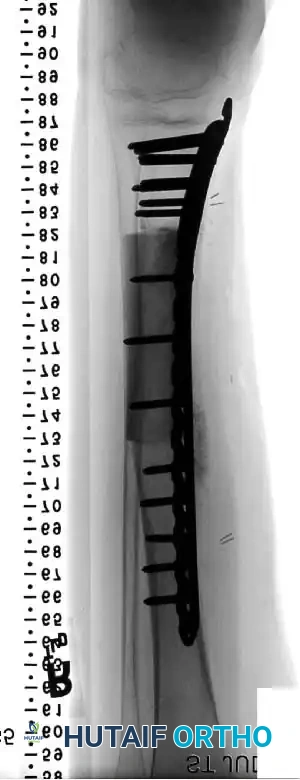
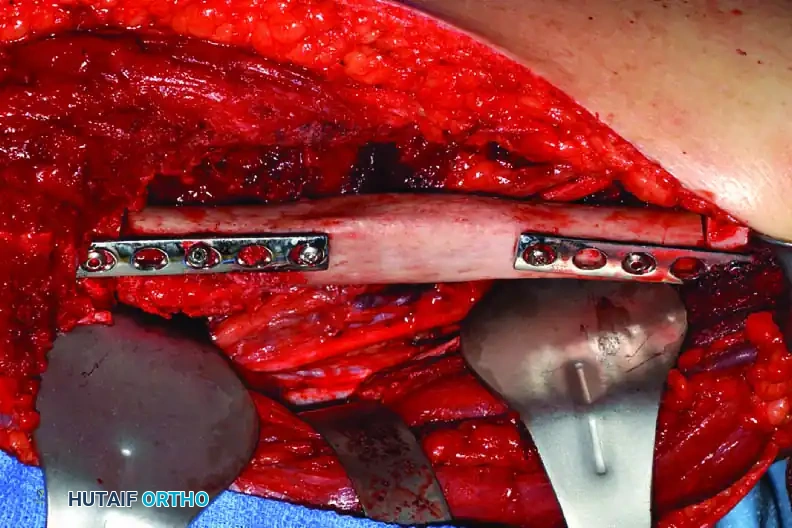
Clinical Pearl: When utilizing an Allograft-Prosthetic Composite (APC), step-cut osteotomies at the host-allograft junction combined with rigid plate fixation significantly increase rotational stability and union rates compared to transverse osteotomies.
Advanced Reconstructive Modalities and Distal Extensions
While proximal humeral resections dominate shoulder oncology, tumors extending into the humeral diaphysis or distal humerus require equally complex limb salvage strategies. Total humeral replacement or distal humeral megaprostheses are viable options when the radial nerve can be preserved or grafted.
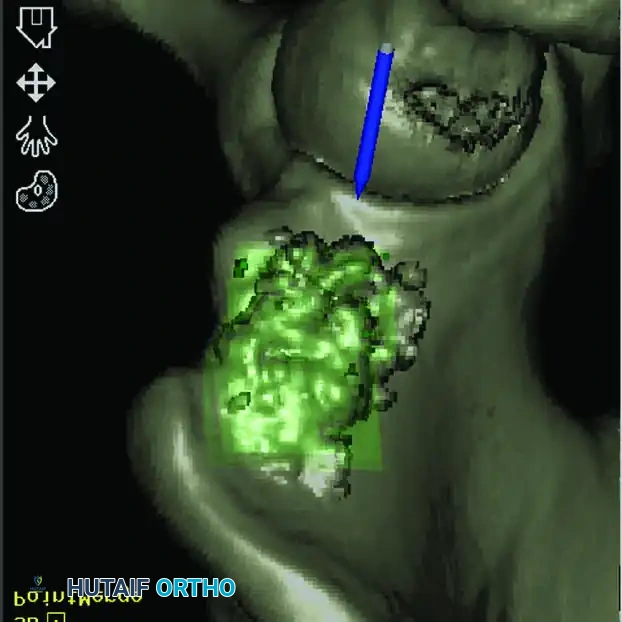
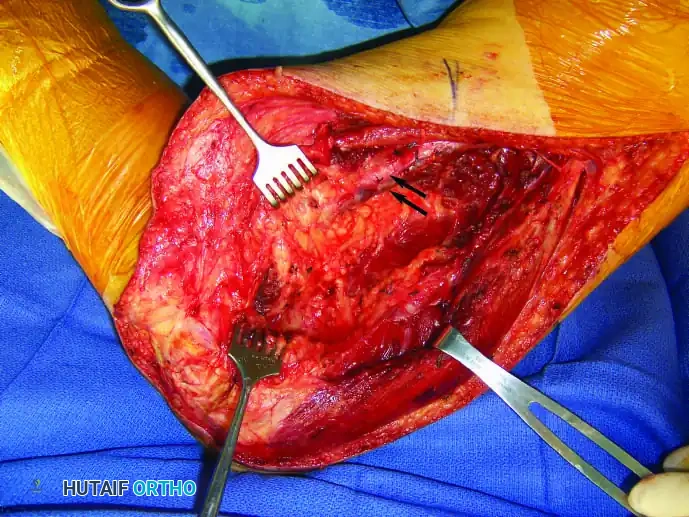
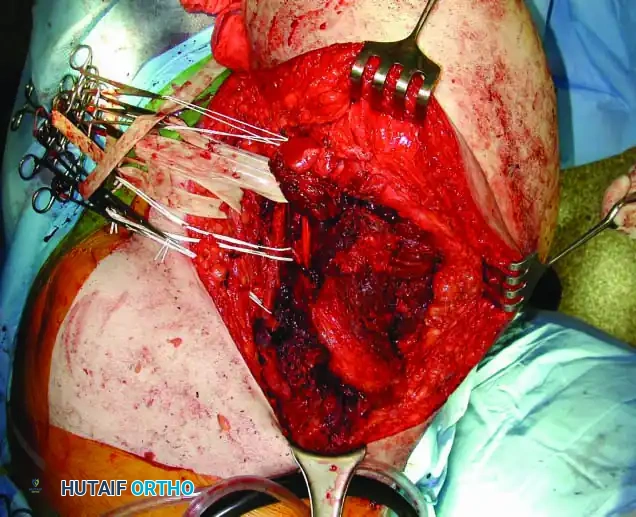
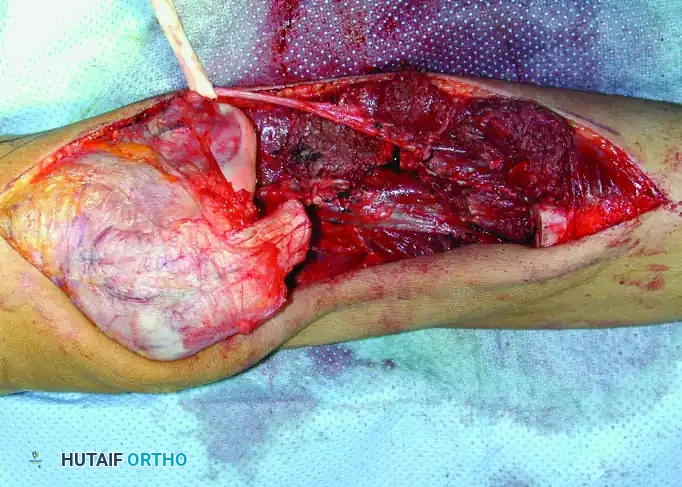
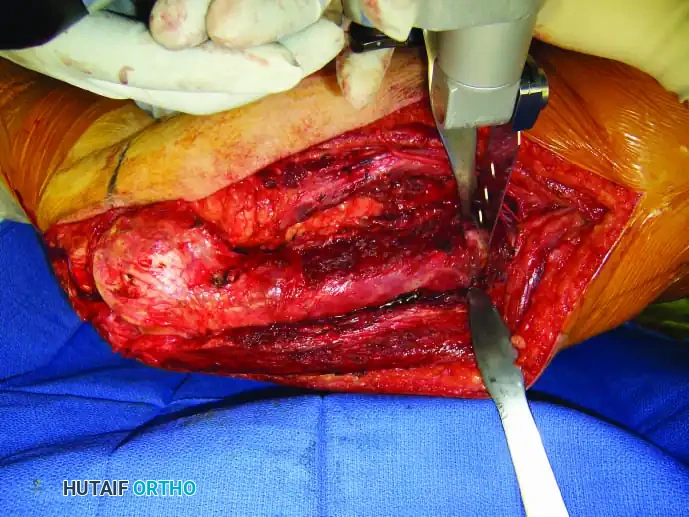
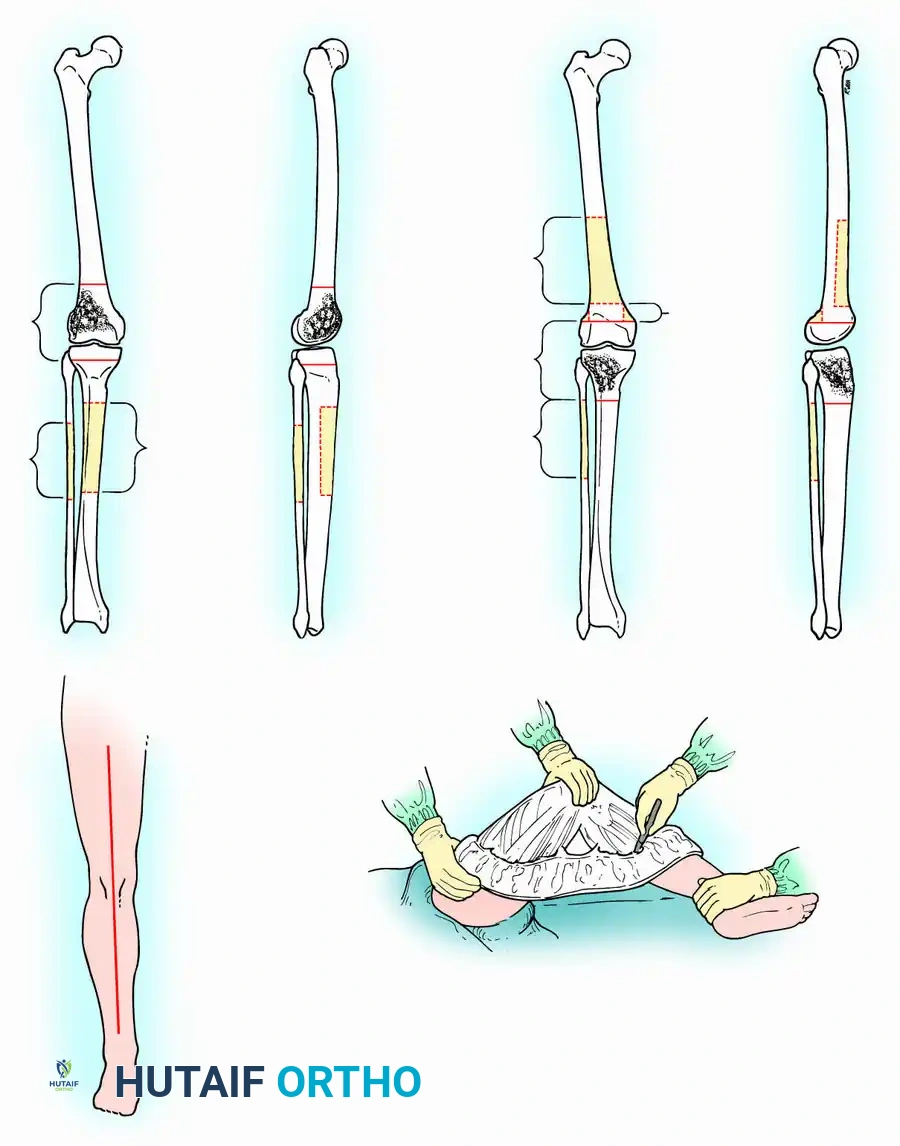
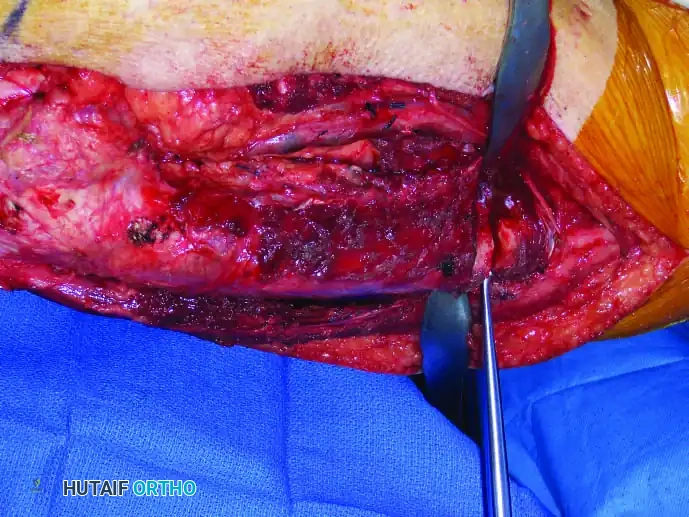
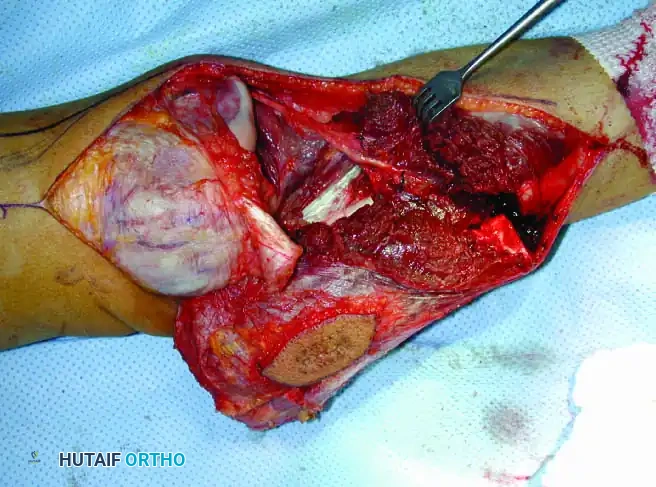
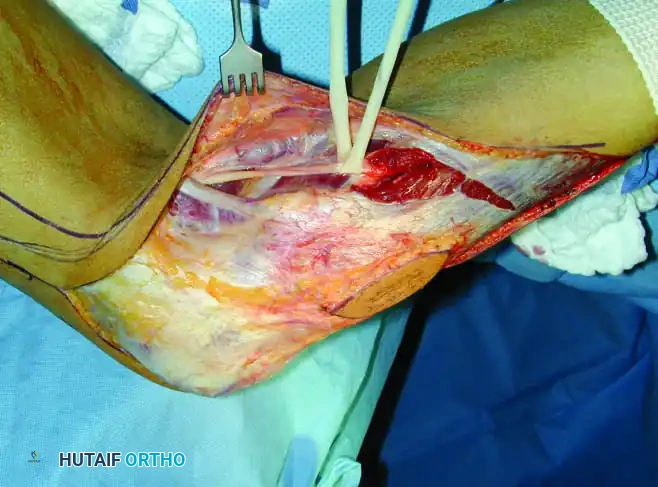
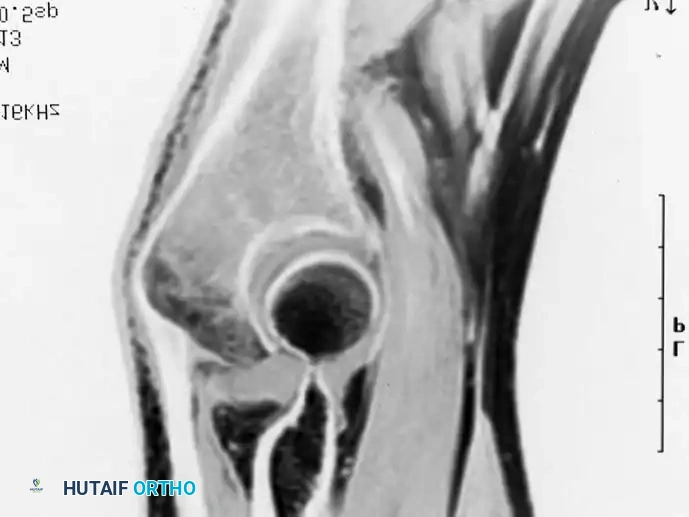
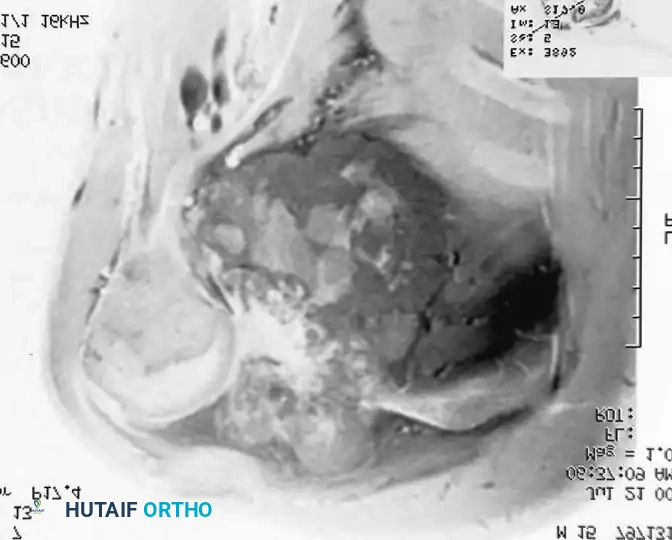
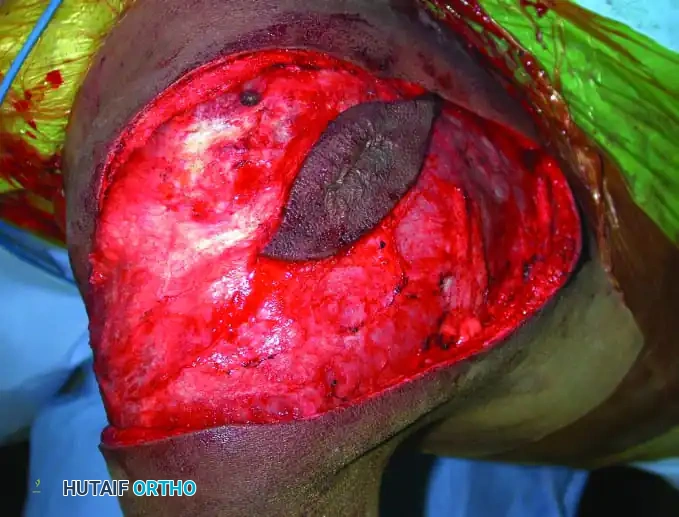
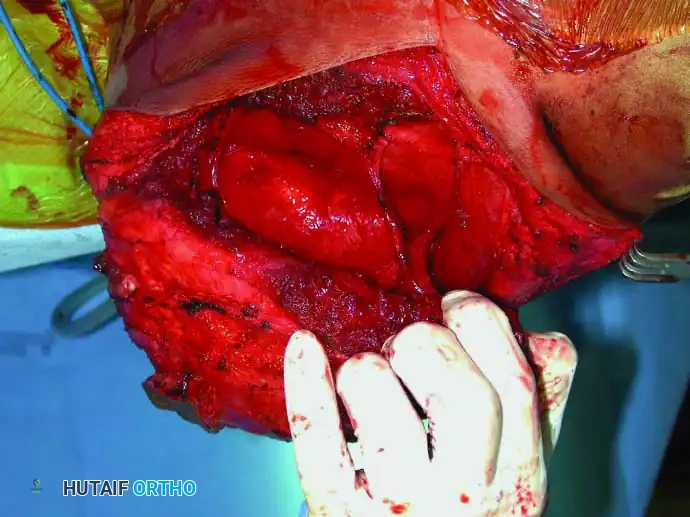
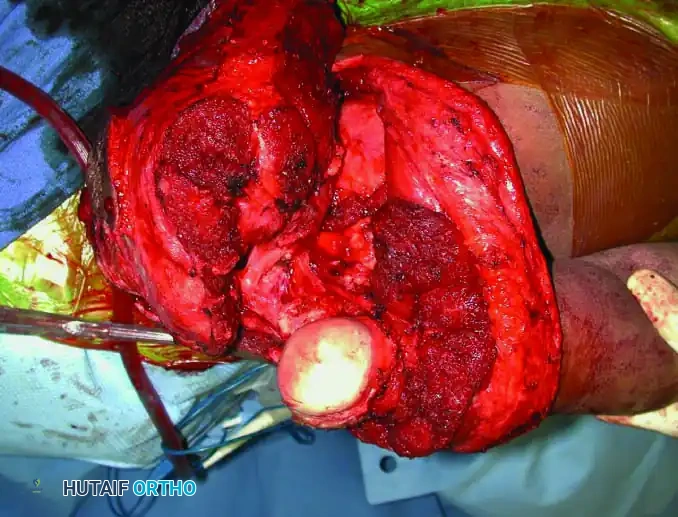
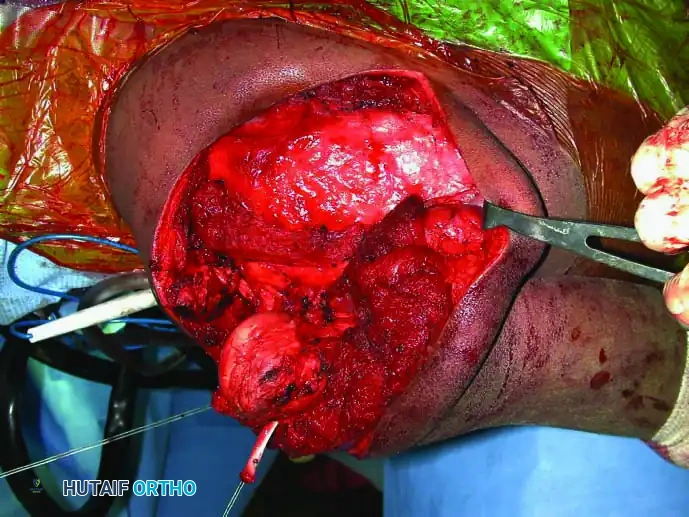
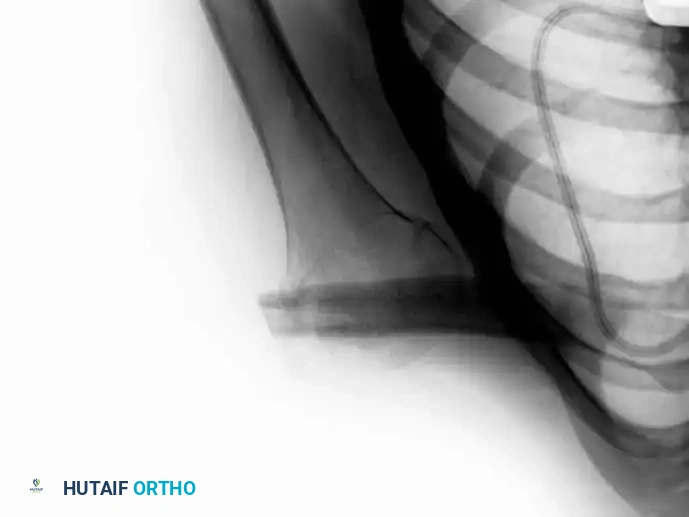
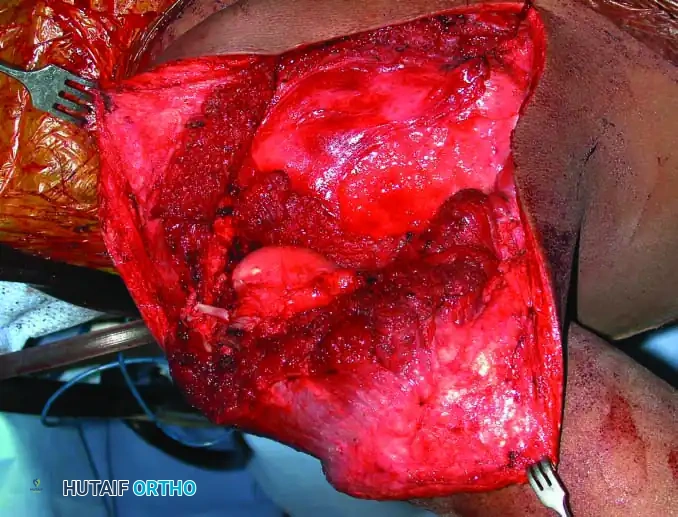
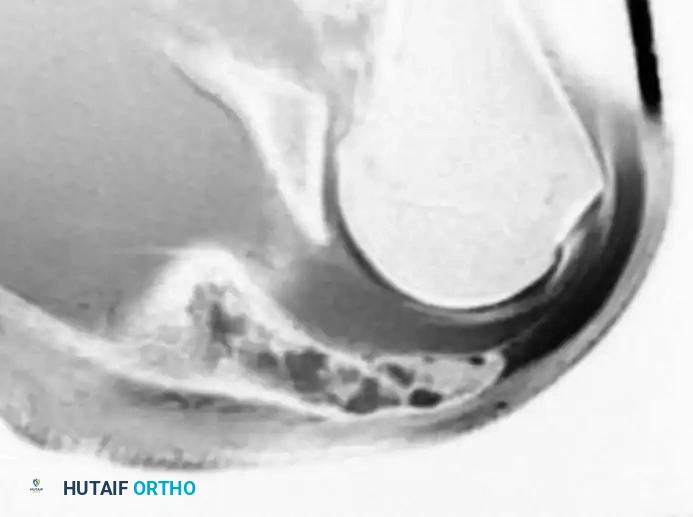
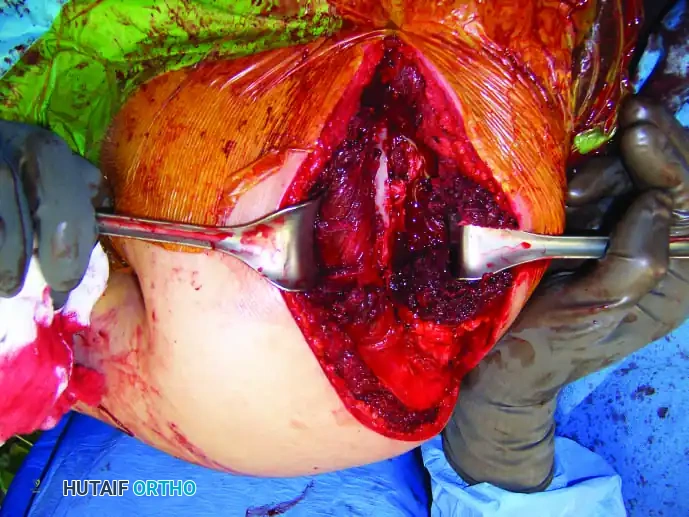
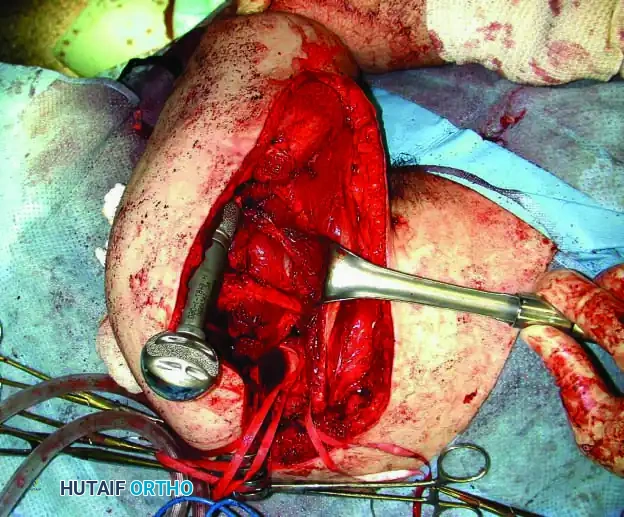
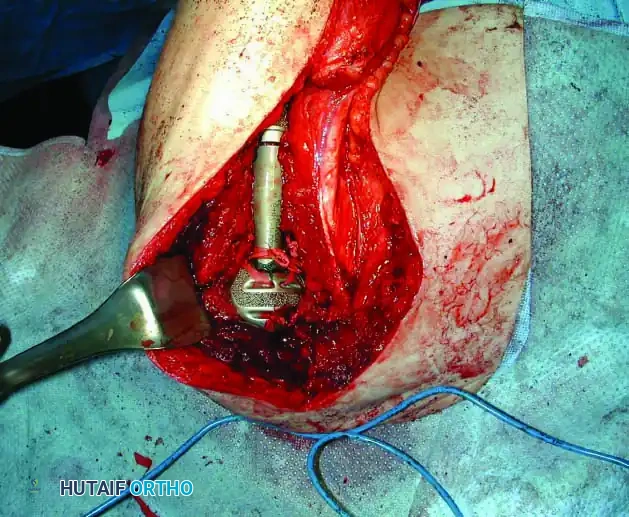
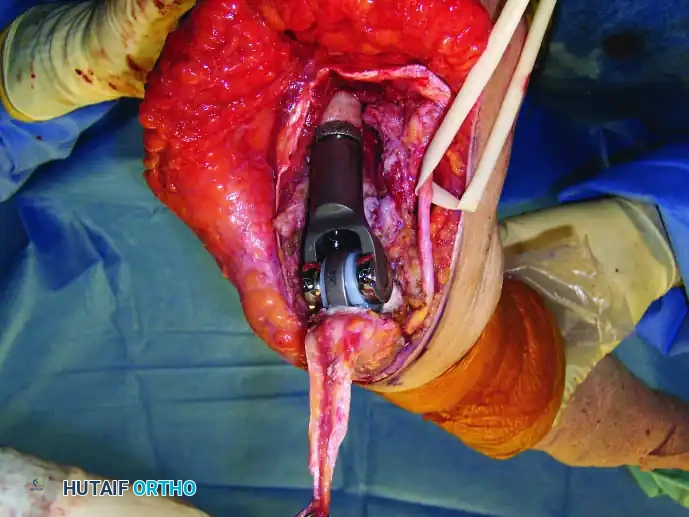
Intraoperative Imaging and Margin Assessment
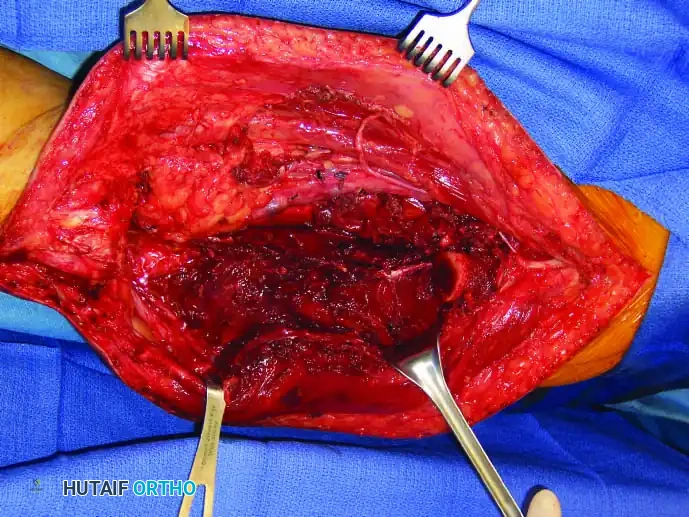
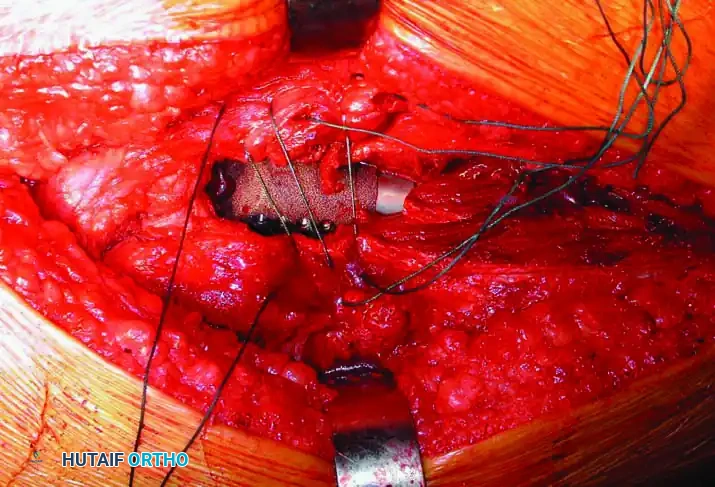
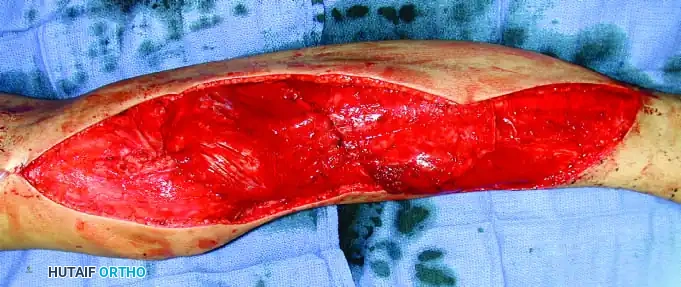
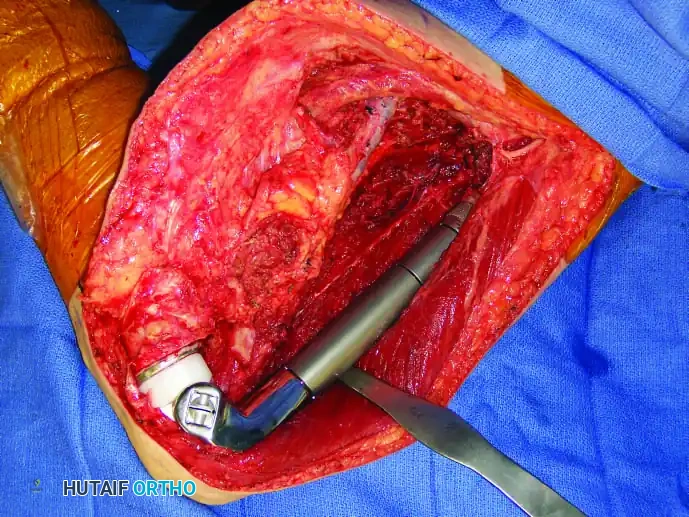
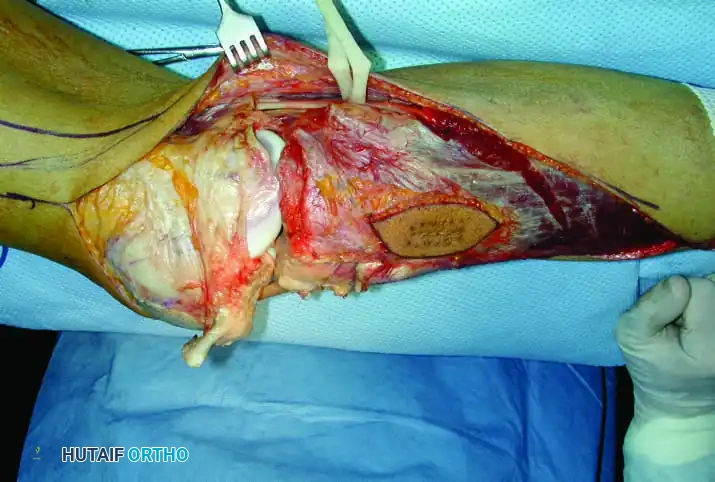
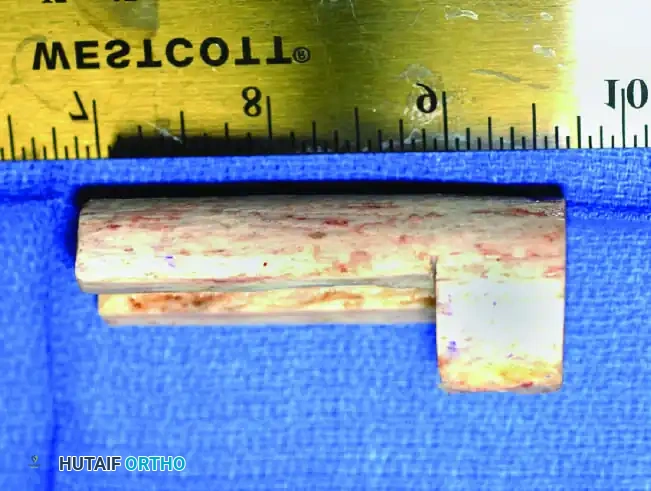
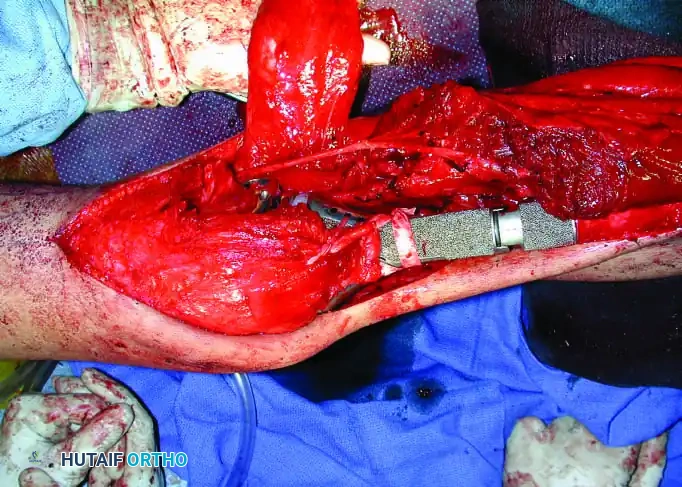
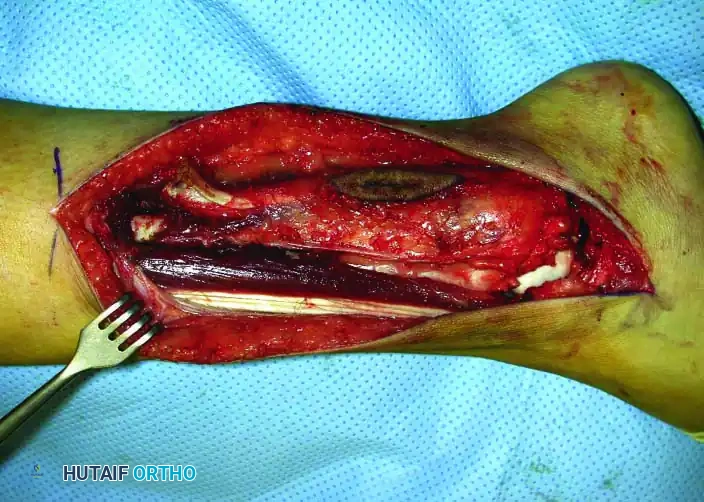
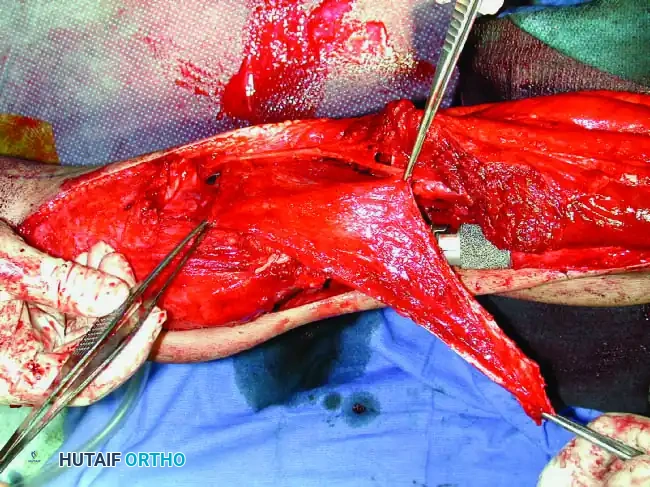
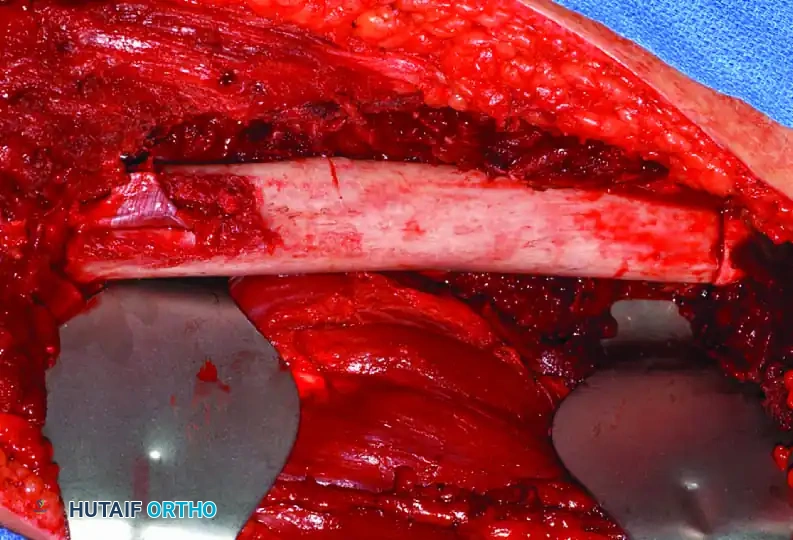
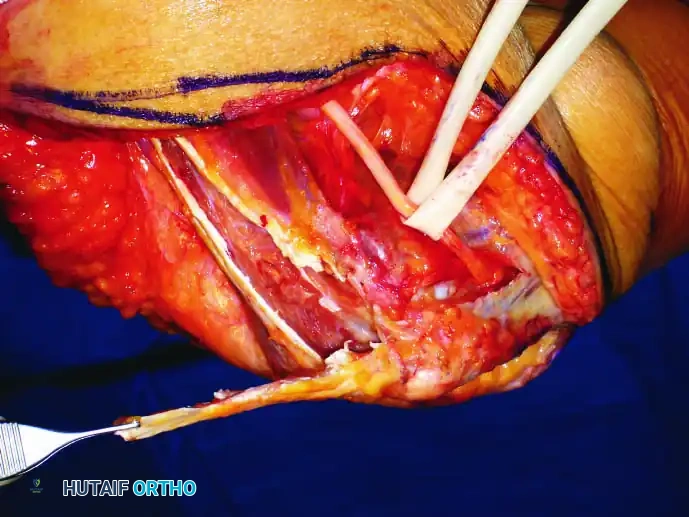
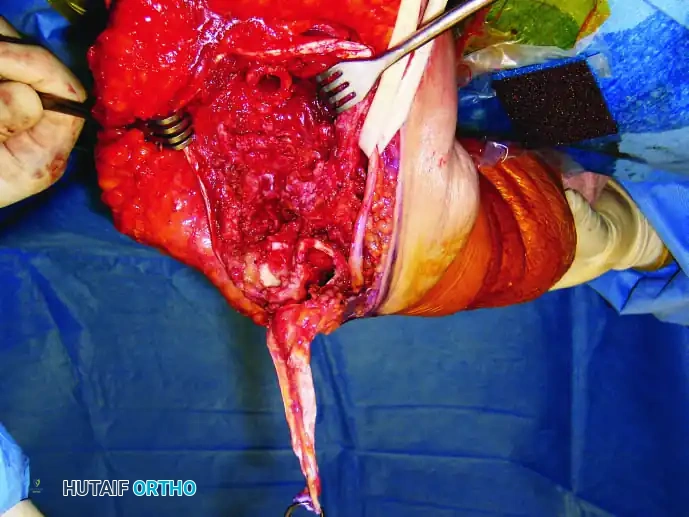
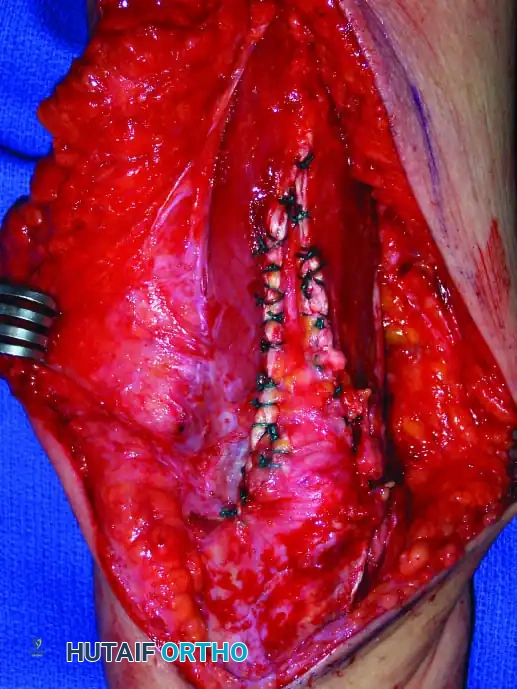
Continuous intraoperative assessment using fluoroscopy and frozen section pathology is mandatory. The following images demonstrate various stages of complex upper extremity resections, allograft preparations, and prosthetic implantations across the humerus and elbow joint.



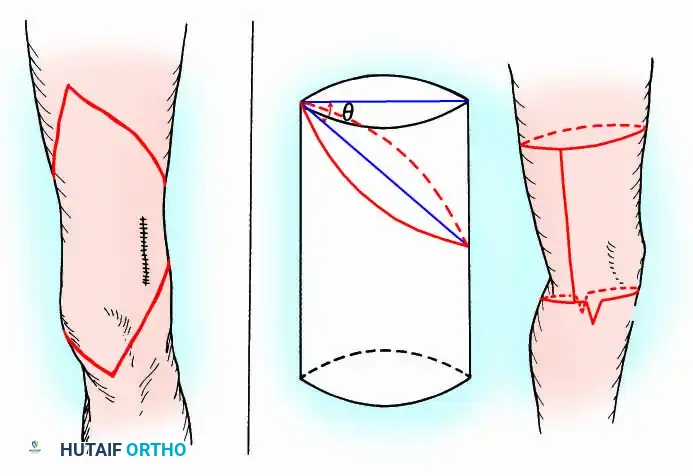
Soft Tissue Coverage and Biologic Integration
In massive resections, local muscle flaps (e.g., latissimus dorsi or pectoralis major rotational flaps) are often required to cover metallic implants and prevent deep infection. The use of synthetic meshes (e.g., Trevira tube) over the prosthesis allows for the ingrowth of fibrous tissue, providing a pseudo-capsule that enhances joint stability and prevents dislocation.

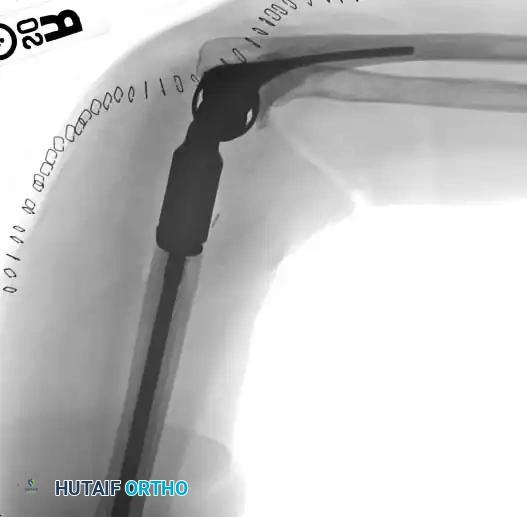

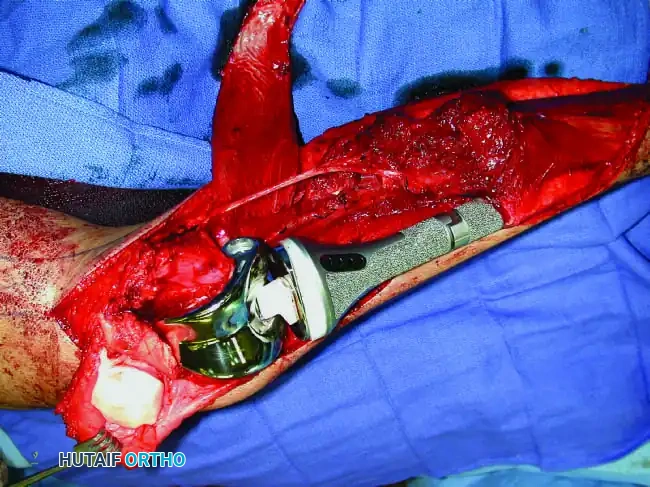
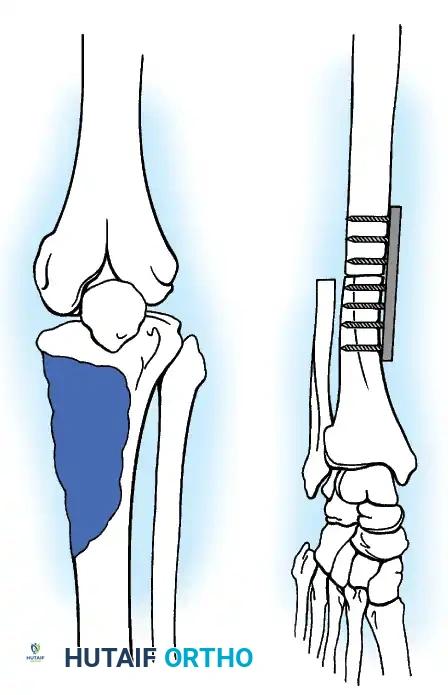
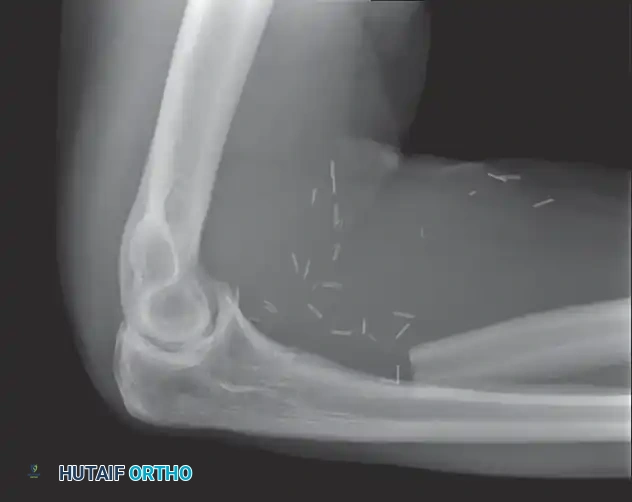
Distal Humerus and Elbow Reconstruction
When tumors involve the distal humerus, resection often requires sacrifice of the collateral ligaments and the articular surface of the elbow. Reconstruction is typically achieved using a linked, semi-constrained total elbow arthroplasty designed for oncologic defects.