Surgical Management of Chronic Ankle Instability: Lateral and Medial Reconstruction
Key Takeaway
Chronic ankle instability often requires surgical intervention when conservative measures fail. This comprehensive guide details the Eyring and Guthrie technique for lateral ligament reconstruction using a peroneus brevis autograft, alongside strategies for medial deltoid repair. It provides orthopedic surgeons with step-by-step surgical approaches, biomechanical principles, and evidence-based postoperative rehabilitation protocols to restore tibiotalar kinematics and prevent long-term arthrosis.
INTRODUCTION TO CHRONIC ANKLE INSTABILITY
Chronic ankle instability (CAI) represents a complex interplay of mechanical laxity and functional deficits following recurrent ankle sprains. When exhaustive conservative management—including peroneal strengthening, proprioceptive training, and bracing—fails to provide dynamic stability, surgical reconstruction becomes imperative to restore tibiotalar kinematics and prevent the insidious progression of post-traumatic arthrosis.
Surgical intervention is broadly categorized into anatomic repairs (e.g., Broström-Gould) and non-anatomic tenodesis reconstructions. The Eyring and Guthrie technique is a robust, non-anatomic lateral reconstruction utilizing a split peroneus brevis autograft. This procedure is particularly indicated in patients with generalized ligamentous laxity, severe attenuation of the native anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL), or those with a high body mass index and demanding physical requirements. Furthermore, the evaluation of chronic instability must extend beyond the lateral complex; concomitant peroneal tendon pathology and medial (deltoid) incompetence are critical variables that dictate the ultimate success of the reconstruction.
PREOPERATIVE EVALUATION AND BIOMECHANICS
Biomechanical Considerations
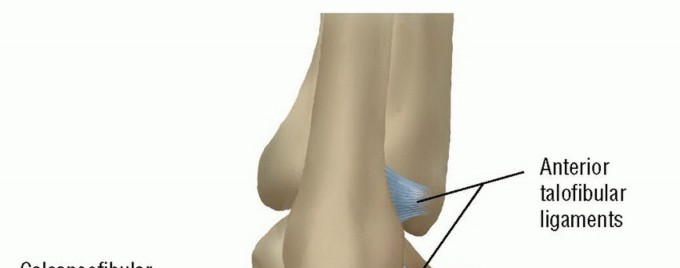
The lateral ligamentous complex primarily resists inversion and anterior translation of the talus within the mortise. The ATFL is the primary restraint to anterior talar translation in plantarflexion, while the CFL restrains inversion in dorsiflexion. Chronic attenuation of these structures alters the center of rotation of the ankle joint, leading to eccentric cartilage loading.
Conversely, the medial deltoid ligament complex is the primary stabilizer against valgus tilting and external rotation of the talus. Biomechanical cadaveric studies have demonstrated that sectioning of the deltoid ligament results in a 43% increase in tibiotalar contact area, while peak articular pressures increase by 30%. Isolated deltoid incompetence results in a valgus tilt of the talus, leading to chronic mechanical failure and rapid progression to tibiotalar arthrosis.
Clinical and Radiographic Assessment
Preoperative evaluation must include a meticulous assessment of hindfoot alignment. A varus hindfoot will place excessive stress on any lateral reconstruction and must be corrected (e.g., via a lateralizing calcaneal osteotomy) concurrently.
Clinical Pearl: Always assess for incompetence of the medial tendons of the ankle, especially the posterior tibial tendon (PTT). The combination of PTT insufficiency and deltoid incompetence is frequently seen in older populations and is categorized by Myerson as a Stage IV adult-acquired flatfoot. Failure to address the medial column will result in rapid failure of lateral reconstructions.
Standard weight-bearing radiographs, alongside anterior drawer and talar tilt stress views, are mandatory. Magnetic Resonance Imaging (MRI) is highly recommended to evaluate the integrity of the peroneal tendons, osteochondral lesions of the talus, and the degree of ligamentous attenuation.
LATERAL REPAIR OF CHRONIC INSTABILITY: THE EYRING AND GUTHRIE TECHNIQUE
The Eyring and Guthrie procedure is designed to reconstruct the lateral stabilizing forces of the ankle by creating a new ligamentous restraint from the anterior two-thirds of the peroneus brevis tendon.
Patient Positioning and Anesthesia
- Anesthesia: General or regional anesthesia (spinal/popliteal block) is utilized.
- Positioning: The patient is placed in the lateral decubitus position or supine with a large bump under the ipsilateral hip to internally rotate the leg, providing unhindered access to the posterolateral ankle.
- Tourniquet: A pneumatic thigh tourniquet is applied and inflated after exsanguination.
Surgical Approach and Exposure

- Incision: Make a curved posterolateral incision approximately 5 inches (12.5 cm) long, centered just posterior to the lateral malleolus. The incision should follow the course of the peroneal tendons, curving gently toward the base of the fifth metatarsal.
- Superficial Dissection: Reflect the skin and subcutaneous fat meticulously to expose the anterolateral aspect of the ankle. Take great care to identify and protect the sural nerve posteriorly and the intermediate dorsal cutaneous nerve anteriorly.
- Retinaculum Mobilization: Mobilize the lateral extensor retinaculum. This structure will be utilized later for tissue reinforcement and to prevent bowstringing of the reconstructed tendons.
- Sinus Tarsi Exposure: Open the sinus tarsi to expose the interosseous talocalcaneal ligament. Place a heavy, non-absorbable retention suture (e.g., #1 or #2 FiberWire) into this ligament for later fixation of the graft.
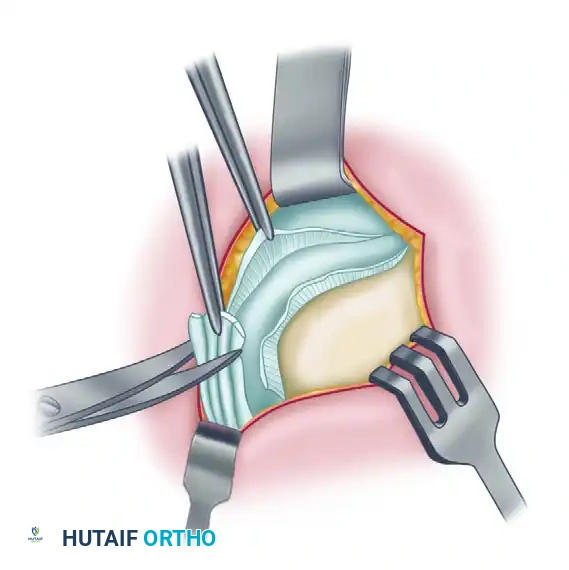
Capsular and Ligamentous Preparation
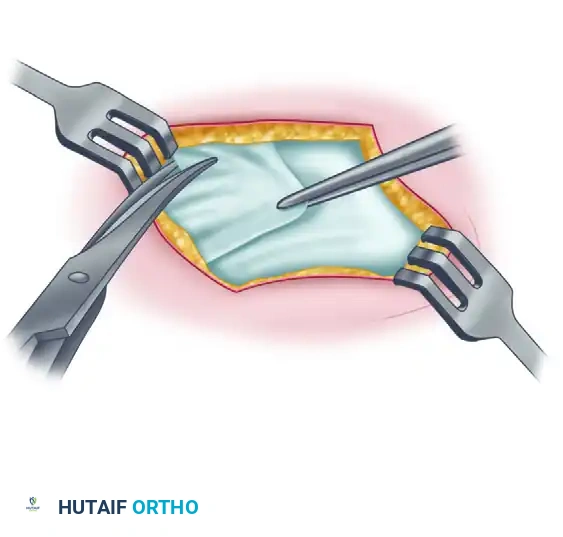
- Capsulotomy: Make a capsular incision, leaving a small cuff of tissue attached to the fibula for potential imbrication or repair.
- Debridement: Inspect the native ATFL and CFL. In chronic cases, these ligaments are often severely stretched, attenuated, or replaced by disorganized scar tissue. Trim the stretched calcaneofibular ligament and the thickened capsular remnants of the anterior talofibular ligament to prepare the bed for the tenodesis graft.
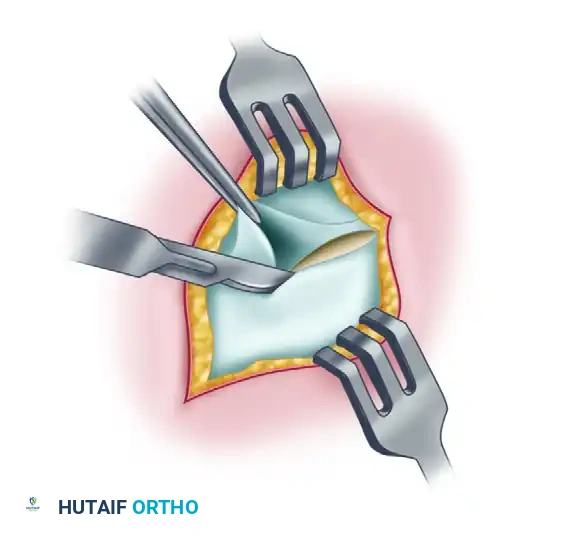
Tendon Harvest and Routing
- Peroneus Brevis Isolation: Expose the peroneus brevis tendon. Isolate its anterior two-thirds approximately 3 inches (7.5 cm) proximal to the tip of the lateral malleolus.
- Tendon Splitting: Longitudinally split the tendon, maintaining the distal insertion of the peroneus brevis on the base of the fifth metatarsal intact.
- Sheath Management: Open the tendon sheath distal to the retinaculum to allow free excursion of the harvested graft.
- Graft Mobilization: Place a hemostat behind the lateral malleolus and pull the free, proximal portion of the harvested tendon down to the level of the fifth metatarsal. This maneuver creates a separate, robust ligamentous graft.
- Routing: Pass the tendon graft behind the lateral retinaculum. Place a locking retention suture (e.g., Krackow stitch) in its free proximal end to facilitate passage through the osseous tunnel.
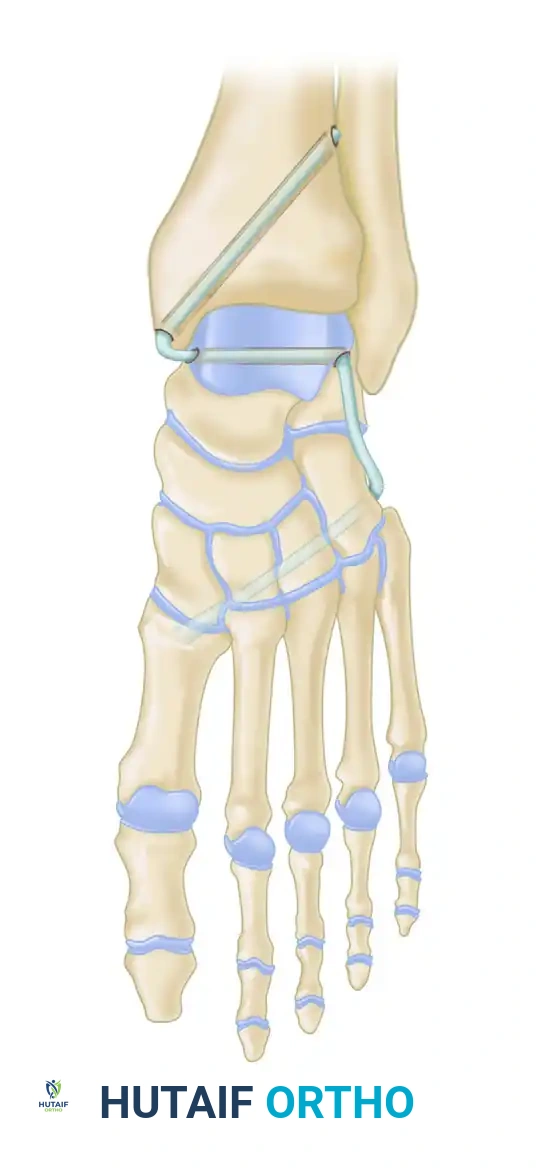
Fibular Tunnel Preparation and Graft Passage
- Drill Hole Placement: Drill an osseous tunnel through the distal fibula. The trajectory should mimic the anatomic origins of the ATFL and CFL.
Surgical Warning: In skeletally immature patients, meticulous fluoroscopic guidance is required to ensure the drill hole completely avoids the distal fibular physis to prevent premature growth arrest and subsequent angular deformity.
- Tunnel Preparation: Remove the periosteum and any obstructing soft tissue from the posterior opening of the drill hole in the fibula.
- Graft Passage: Pass the detached, sutured portion of the peroneus brevis tendon from posterior to anterior through the fibular drill hole.
Surgical Pearl: A bent Keith needle or a suture passing loop is highly effective for retrieving the retention suture within the tight confines of the posterior fibula and pulling the tendon graft smoothly through the osseous tunnel.
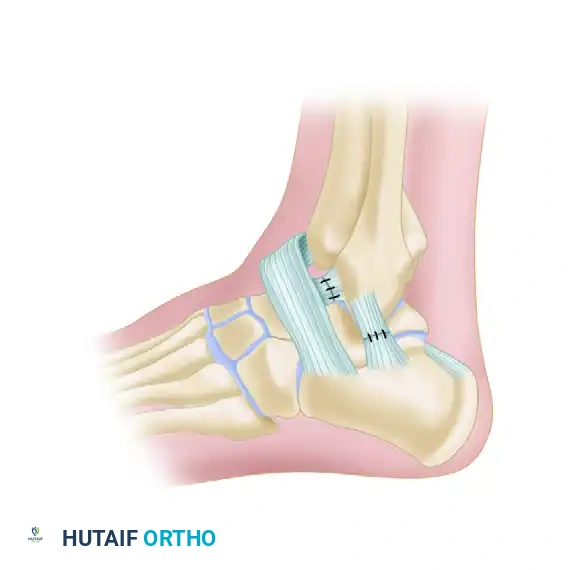
Fixation and Reconstruction Tensioning

- Tensioning: The assistant must hold the foot in neutral dorsiflexion and slight eversion. This is the most critical step of the procedure; over-tensioning will severely restrict subtalar and tibiotalar motion, while under-tensioning will result in recurrent instability.
- Primary Fixation: Secure the newly routed "ligament" to the anterior periosteum of the fibula with one or two heavy non-absorbable sutures.
- Secondary Fixation: Fix the remaining distal portion of the reconstruction to the previously placed retention suture in the interosseous talocalcaneal ligament within the sinus tarsi. This step effectively recreates the stabilizing vector of the cervical and interosseous ligaments.
- Capsular Imbrication: If viable native capsular tissue remains, shorten and reattach the attenuated ATFL and CFL over the reconstruction to provide an additional layer of anatomic reinforcement.
Closure and Analgesia
- Retinacular Repair: Suture the extensor retinaculum over the repair. This prevents bowstringing of the graft and provides a smooth gliding surface for the overlying subcutaneous tissues.
- Wound Closure: Close the peroneal tendon sheath, subcutaneous tissues, and skin in a layered fashion while maintaining the foot in neutral flexion.
- Postoperative Analgesia: Infiltrate the entire wound and intra-articular ankle space with approximately 10 mL of a local anesthetic mixture. A highly effective, evidence-based formulation is 4 parts 0.5% bupivacaine (Marcaine) mixed with 1 part 4 mg/mL dexamethasone (Decadron). The addition of the corticosteroid significantly prolongs the duration of the sensory block and reduces acute postoperative inflammation and pain.
MANAGEMENT OF CONCOMITANT PERONEAL PATHOLOGY
Chronic ankle instability is rarely an isolated ligamentous event. The altered kinematics place immense sheer and tensile stress on the peroneal tendons, frequently leading to longitudinal split tears.
Bonnin et al. conducted a pivotal study on patients with split lesions of the peroneus brevis tendon associated with chronic ankle instability.
- Clinical Presentation: The primary complaint is often retromalleolar pain, accompanied by a sensation of giving way.
- Diagnosis: While preoperative MRI and tenography are useful, these lesions are notoriously difficult to visualize on imaging. Diagnosis is often confirmed only via direct surgical exploration. The lesions are typically localized at the tip of the lateral malleolus and become visible only after the peroneal retinaculum is fully opened.
- Surgical Imperative: Bonnin et al. concluded that split lesions of the peroneus brevis are a direct mechanical result of chronic ankle laxity. The peroneal tendons must be meticulously inspected during every surgical procedure for ankle laxity.
- Treatment: Depending on the degree of tendon degeneration, treatment ranges from simple tubularization and tendinous repair to complex reconstructions (e.g., Chrisman-Snook) utilizing the remaining viable tendon. Neglected peroneus brevis split tears are a primary cause of residual lateral pain following otherwise successful ligamentous repairs.
MEDIAL REPAIR OF CHRONIC INSTABILITY
While lateral ankle instability is ubiquitous in orthopedic practice, chronic medial instability is less common, more challenging to treat, and historically associated with less predictable surgical outcomes.
Pathoanatomy and Indications
Patients with chronic medial ankle instability typically present with a history of a severe pronation-eversion injury, though many report a vague history of multiple sprains without a clear mechanism.
The deltoid ligament is a massive, multi-fascicular structure. Its incompetence leads to profound kinematic derangement. As previously noted, loss of the deltoid ligament increases tibiotalar contact area by 43% and peak pressures by 30%, rapidly accelerating joint degeneration.
Medial ankle ligament reconstruction is strictly indicated in patients with chronic, symptomatic mechanical instability who have failed exhaustive conservative treatment, provided that advanced tibiotalar arthrosis has not yet developed.
Surgical Reconstruction Principles
Because direct primary repair of a chronically attenuated deltoid ligament is rarely feasible due to poor tissue quality, reconstruction using autograft or allograft is usually required.
- Graft Selection: The peroneus longus autograft (or a robust allograft such as semitendinosus) is frequently utilized to reconstruct the medial complex.
- Technique Overview: The reconstruction aims to recreate the deep (tibiotalar) and superficial (tibiocalcaneal/tibionavicular) fibers of the deltoid.
- Osseous Tunnels: Tunnels are drilled into the medial malleolus, the medial aspect of the talus, and the sustentaculum tali of the calcaneus.
- Routing and Fixation: The graft is routed through these tunnels to recreate the V-shaped anatomic configuration of the deltoid ligament. Fixation is typically achieved with interference screws or suspensory cortical buttons. Tensioning must be performed with the ankle in neutral dorsiflexion and slight inversion to restore the medial restraint without over-constraining the joint.
POSTOPERATIVE CARE AND REHABILITATION PROTOCOL
The success of both lateral and medial ankle reconstructions relies heavily on strict adherence to a phased postoperative rehabilitation protocol. The goal is to protect the healing tenodesis while preventing debilitating joint stiffness.
Phase I: Maximum Protection (Weeks 0-4)
- Immobilization: Immediately postoperatively, a light compression dressing and a well-molded, short-leg cast are applied with the foot locked in a strictly neutral position.
- Weight-Bearing: The patient is strictly non-weight-bearing on the operative extremity.
- Wound Care: Sutures are removed at 2 weeks postoperatively. The patient is then placed back into a cast or a rigid boot locked in neutral for an additional 2 weeks.
Phase II: Controlled Mobilization (Weeks 4-7)
- Transition: At 4 weeks post-surgery, the cast is removed.
- Support: A controlled ankle motion (CAM) walking boot is utilized for ankle support for the next 3 weeks.
- Physical Therapy: An active exercise program is initiated. Therapy focuses on active range of motion (dorsiflexion and plantarflexion). Inversion and eversion are introduced gradually and cautiously to avoid stressing the graft.
- Weight-Bearing: Progressive weight-bearing as tolerated is permitted within the CAM boot.
Phase III: Strengthening and Proprioception (Weeks 7-12)
- Weaning: The patient is transitioned from the CAM boot to a functional lace-up ankle brace.
- Therapy Focus: Intensive physical therapy begins, focusing on peroneal strengthening, Achilles stretching, and advanced proprioceptive training (e.g., balance board, single-leg stance exercises).
Phase IV: Return to Activity (Months 3-6)
- Vigorous Activity: For 3 to 4 months postoperatively, additional rigid brace support is mandatory during any vigorous, high-impact, or pivoting activities.
- Clearance: Full return to competitive sports is typically permitted between 4 to 6 months, contingent upon the restoration of full dynamic stability, symmetric strength, and the absence of pain. Early mobilization, as advocated by modern literature, prevents arthrofibrosis, but must be carefully balanced against the mechanical limits of the healing graft.
📚 Medical References
- chronic ankle instability, Oper Tech Orthop 2:142, 1992.
- Hamilton WG, Thompson FM, Snow SW: The modifi ed Broström procedure for lateral ankle instability, Foot Ankle Int 14:1, 1993.
- Hangody L, Kish G, Karpati Z, et al: Treatment of osteochondritis dissecans of the talus: use of the mosaicplasty technique—a preliminary report, Foot Ankle Int 18:628, 1997.
- Harper MC: The deltoid ligament: an evaluation of need for surgical repair, Clin Orthop Relat Res 226:156, 1988.
- Harper MC: Stress radiographs in the diagnosis of lateral instability of the ankle and hindfoot, Foot Ankle 13:435, 1992.
- Harper MC: Modifi cation of the Gould modifi cation of the Broström ankle repair, Foot Ankle Int 19:788, 1998.
- Hauger O, Moinard M, Lasalarie JC, et al: Anterolateral compartment of the ankle in the lateral
You Might Also Like