INTRODUCTION AND DEFINITION
Subtrochanteric femoral fractures represent a complex and highly challenging subset of proximal femur fractures. Anatomically defined as fractures occurring in the region between the lesser trochanter and the isthmus of the femoral canal, they are frequently described in the literature as fractures localized within the first 5 cm distal to the lesser trochanter.
Initially characterized by Boyd and Griffin as a variant of peritrochanteric femoral fractures associated with a notoriously high incidence of unsatisfactory results, the management of these injuries continues to demand meticulous surgical planning. The subtrochanteric region is subjected to the highest biomechanical stresses in the human skeleton, experiencing massive compressive forces along the medial cortex and profound tensile forces along the lateral cortex. Consequently, surgical intervention requires not only a robust implant but an intimate understanding of the deforming forces at play to prevent catastrophic malunion or implant failure.
SURGICAL ANATOMY AND BIOMECHANICS
Understanding the deforming forces acting upon the proximal femur is the most critical prerequisite for avoiding the typical malalignments (varus, procurvatum, and external rotation) associated with subtrochanteric femoral fractures.
The proximal and distal fracture fragments are subjected to intense, opposing muscular pulls:
- Proximal Fragment: Strongly influenced by the pull of the abductors (gluteus medius and minimus inserting on the greater trochanter), the short external rotators, and the iliopsoas (inserting on the lesser trochanter). The net result of these muscle insertions is profound abduction, external rotation, and flexion of the proximal segment.
- Distal Fragment: Strongly influenced by the pull of the adductor complex (inserting along the linea aspera). This results in severe medialization of the distal fragment.
- Global Deformity: The overall combined pull of the massive quadriceps and hamstring muscle groups results in significant axial shortening of the extremity.
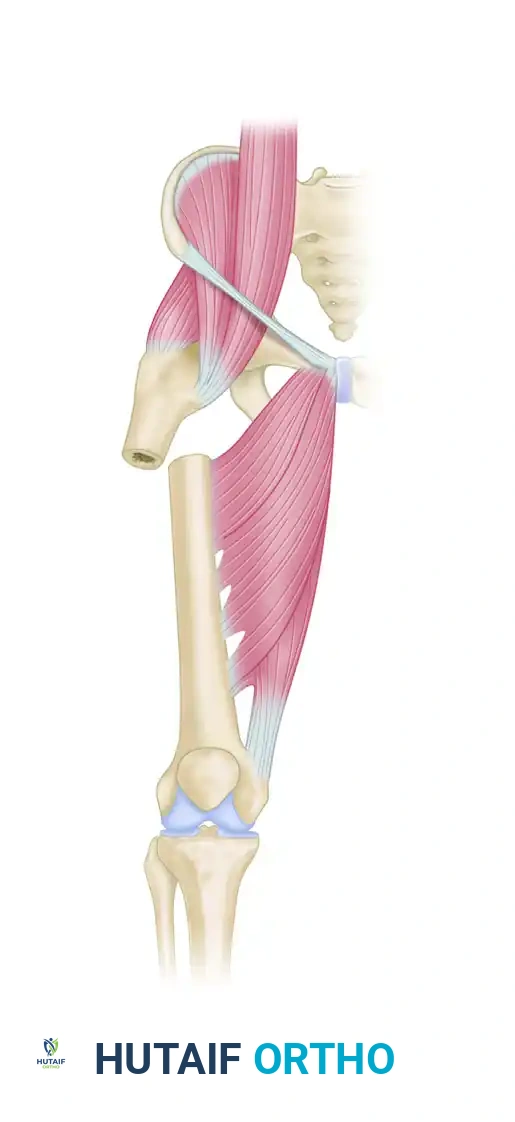
Anatomical illustration demonstrating the intact muscular forces acting across the proximal femur, highlighting the vectors of the iliopsoas, abductors, and adductors.
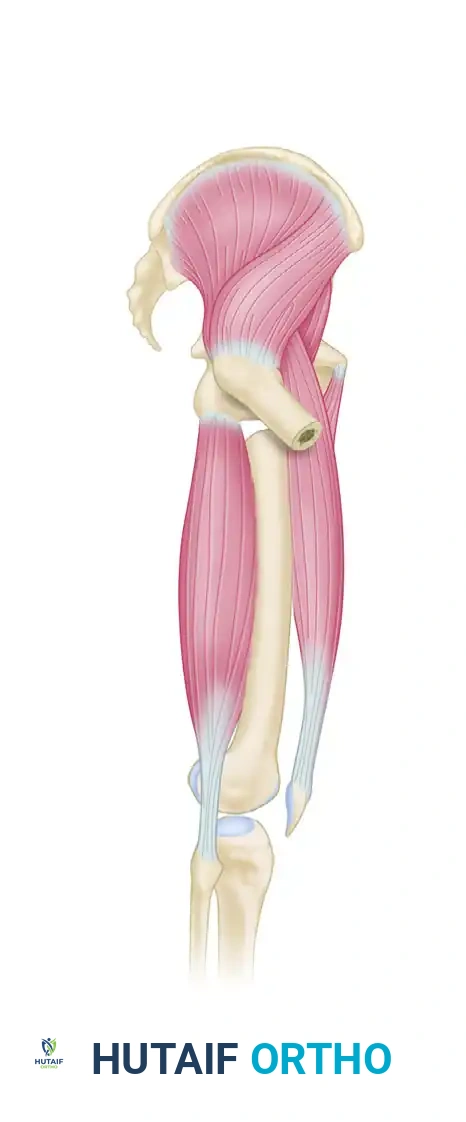
Deforming forces acting on a subtrochanteric femoral fracture. Note the classic flexion, abduction, and external rotation of the proximal fragment coupled with medialization and shortening of the distal fragment.
Clinical Pearl: More proximal subtrochanteric fractures are influenced to a much greater degree by these deforming forces than those occurring further distal to the lesser trochanter. Furthermore, the integrity of the lesser trochanter dictates the degree of flexion; fractures that compromise the lesser trochanter may defunctionalize the iliopsoas, resulting in less severe flexion and external rotation of the proximal fragment.
CLASSIFICATION SYSTEMS
Numerous classification systems have been proposed since Boyd and Griffin's initial work in 1949. However, the Russell-Taylor Classification remains the most clinically relevant framework. It guides surgical decision-making by evaluating two critical anatomical zones: the integrity of the lesser trochanter and the extension of fracture lines into the piriformis fossa.
The involvement of the piriformis fossa dictates the viability of a standard trochanteric entry portal, while the integrity of the lesser trochanter dictates the biomechanical stability of the medial calcar.
Type I: Fractures do not extend into the piriformis fossa.
-
Type IA: The lesser trochanter remains intact. These fractures possess inherent medial stability.


-
Type IB: The lesser trochanter is not intact, compromising medial cortical support and increasing the risk of varus collapse. Reverse obliquity fractures are often functionally categorized as Russell-Taylor IB due to their biomechanical behavior and inherent instability.

Type II: Fractures extend proximally into the piriformis fossa.
-
Type IIA: The lesser trochanter is intact, but the proximal extension complicates standard piriformis entry nailing.


-
Type IIB: The lesser trochanter is not intact, and the fracture extends into the piriformis fossa. This is a highly unstable, complex fracture pattern requiring advanced cephalomedullary reconstruction.

While advances in intramedullary nailing implants have somewhat reduced the strict dependency on this classification for implant selection, it remains an indispensable descriptive tool for preoperative planning and anticipating intraoperative reduction challenges.
INDICATIONS FOR SURGERY AND IMPLANT SELECTION
The absolute mainstay of treatment for subtrochanteric femoral fractures is intramedullary nailing (IMN). Extensive biomechanical and clinical evidence demonstrates that intramedullary implants are vastly superior to extramedullary implants (such as dynamic condylar screws or standard plates) in this high-stress region. IM nails act as load-sharing devices, positioned closer to the mechanical axis of the femur, thereby reducing the bending moment and minimizing the risk of implant fatigue failure.
While IMN is the gold standard, there are specific, complex circumstances—such as severe proximal articular extension, narrow medullary canals, or specific salvage procedures—where 95-degree fixed-angle blade plates or proximal femoral locking plates remain highly useful in the orthopedic surgeon's armamentarium.
Locking Configurations: Standard vs. Reconstruction Mode
Modern nailing systems allow for standard proximal interlocking (transverse or oblique screws into the lesser trochanteric region) as well as locking in reconstruction mode (utilizing two cephalomedullary screws directed into the femoral head).
- Russell-Taylor IB, IIA, and IIB fractures: Must be proximally locked in reconstruction mode to bypass the compromised proximal anatomy and secure fixation directly into the dense trabecular bone of the femoral head.
- Russell-Taylor IA fractures: Can theoretically be locked in standard or reconstruction mode. However, for IA fractures located very close to the lesser trochanter, reconstruction mode is strongly preferred.
Surgical Warning: Based on contemporary biomechanical data, many academic centers now advocate that all subtrochanteric femoral fractures should be locked in reconstruction mode to maximize construct rigidity and prevent varus collapse. For patients with osteoporotic bone or inadequate bone stock in the femoral head, a robust cephalomedullary device such as a Gamma nail or the TRIGEN InterTAN system is highly recommended.
PREOPERATIVE PLANNING AND PATIENT POSITIONING
The choice of patient positioning is heavily influenced by the patient's body habitus and the specific characteristics of the fracture pattern.
Supine Positioning on a Fracture Table
We prefer the supine position on a radiolucent fracture table for the vast majority of subtrochanteric fractures. This allows for excellent biplanar fluoroscopic visualization and utilizes a modified medial trochanteric portal. The unaffected leg is typically placed in a hemilithotomy position (scissored down and away) to allow unimpeded access for the C-arm.
Lateral Decubitus Positioning
We reserve the lateral decubitus position for morbidly obese patients or highly complex fracture patterns. In obese patients, the supine position often causes the abdominal pannus to push the surgeon's hand and instruments laterally, forcing a medialized, eccentric starting point that inevitably leads to varus malreduction. The lateral position allows gravity to pull the soft tissues anteriorly, providing a collinear trajectory for the guidewire and reamers.
A free-hand technique on a flat radiolucent table can also be highly effective, provided an adequate number of skilled surgical assistants are available to maintain manual traction and reduction.
OPERATIVE TECHNIQUE: INTRAMEDULLARY NAILING
The successful intramedullary nailing of a subtrochanteric fracture relies on two non-negotiable principles: achieving anatomic reduction prior to reaming, and maintaining absolute trajectory control during canal preparation.
1. Fracture Reduction
The intramedullary nail will not reduce the fracture; rather, it will permanently lock the femur in whatever alignment exists at the time of reaming. Due to the deforming forces, closed reduction is often insufficient.
* Percutaneous Techniques: Use a ball-spike pusher or a Schanz pin placed percutaneously into the proximal fragment to counteract flexion and external rotation.
* Mini-Open Techniques: Do not hesitate to make a small lateral incision to apply a collinear reduction clamp.
* Poller (Blocking) Screws: Placed strategically in the wide proximal metaphysis to narrow the canal and force the nail into the desired trajectory, preventing varus and procurvatum.
2. Trajectory Control and Portal Preparation
We strongly advocate for the concept of "Trajectory Control" in the treatment of these fractures. Trajectory control involves the precise establishment of the proximal nail portal under strict fluoroscopic guidance.
The starting point must be perfectly collinear with the medullary canal. Once the guidewire is placed, the surgeon must obtain anterior and lateral cortical support. We routinely utilize a specialized channel reamer (e.g., Channel Reamer, Smith & Nephew, Memphis, TN). Reaming through this protected channel prevents the reamer from migrating laterally into the softer cancellous bone of the greater trochanter. Retrospective institutional data confirms that implementing trajectory control and routinely using a channel reamer drastically reduces the incidence of eccentric reaming and subsequent varus malalignment.
3. Cephalomedullary Fixation (The InterTAN Technique)
When utilizing an integrated dual-screw cephalomedullary system like the InterTAN, precise stepwise execution is required to achieve optimal compression and rotational stability of the proximal fragment.
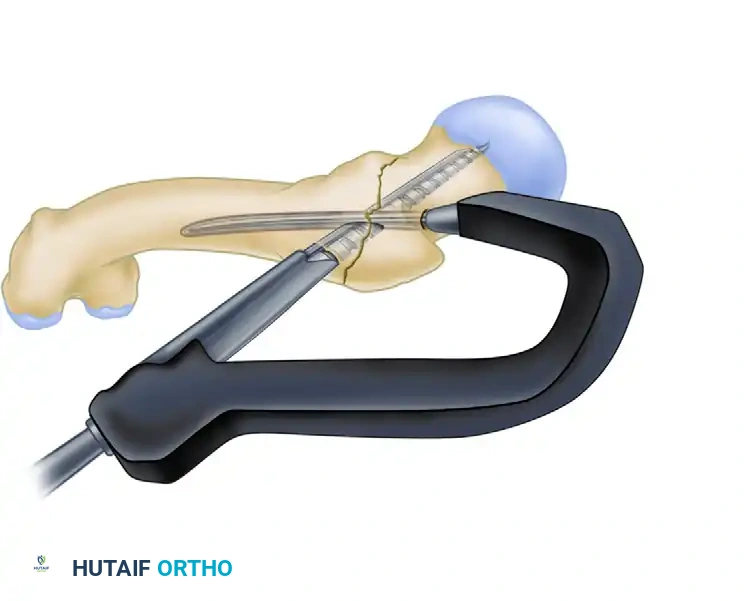
Step A: Guidewire Placement and Drilling
After the nail is seated at the correct depth, the guidewire for the inferior lag screw is placed centrally within the femoral head on both AP and lateral fluoroscopic views.

Drilling for the lag screw with the derotational bar in place. The derotational bar prevents the proximal fragment from spinning during the aggressive reaming process.
Step B: Lag Screw Insertion
The primary lag screw is inserted over the guidewire. This screw provides the foundational purchase within the femoral head.
Insertion of the primary lag screw into the femoral head.
Step C: Integrated Compression Screw Insertion
The secondary, integrated compression screw is then inserted through the same proximal portal of the nail. As this screw engages the primary lag screw, it creates active, controlled linear compression across the fracture site (if the fracture pattern allows) and provides exceptional rotational stability.

Insertion of the integrated compression screw, locking the construct and providing rotational control.
Step D: Final Construct Verification
Fluoroscopy is used to confirm the final seating of the cephalomedullary screws, ensuring no joint penetration and verifying the restoration of the neck-shaft angle.

Final integrated construct demonstrating the interlocking mechanism of the cephalomedullary screws.
4. Distal Interlocking
Distal interlocking is performed using a perfect circles technique under fluoroscopy. For subtrochanteric fractures, at least two distal locking screws are recommended to control rotation and maintain length, particularly in comminuted or length-unstable patterns.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol is heavily dictated by the fracture pattern, bone quality, and the stability of the surgical construct.
- Weight Bearing: Patients with subtrochanteric or intertrochanteric femoral fractures treated with a robust cephalomedullary device (such as an InterTAN) are generally allowed to bear weight as tolerated (WBAT) immediately postoperatively in most circumstances. The load-sharing nature of the IM nail and the rotational stability of the dual-screw proximal fixation typically support early mobilization.
- Modifications for Instability: In cases of highly unstable fracture patterns (e.g., severe medial comminution, reverse obliquity with distal extension) or profound osteoporosis, weight-bearing may need to be temporarily modified (e.g., toe-touch weight-bearing for 4-6 weeks) based on the surgeon's intraoperative assessment.
- Physical Therapy: Early focus is placed on hip and knee range of motion, abductor strengthening, and deep vein thrombosis (DVT) prophylaxis.
- Follow-up: Serial radiographs are obtained at 2, 6, and 12 weeks to monitor for maintenance of alignment, progression of callus formation, and to rule out hardware failure or varus collapse.
CONCLUSION
Subtrochanteric femoral fractures remain a formidable orthopedic challenge due to the intense deforming forces inherent to the proximal femur. Successful management requires a deep understanding of the Russell-Taylor classification, meticulous preoperative planning, and flawless intraoperative execution. By prioritizing anatomic reduction prior to reaming, utilizing trajectory control to prevent eccentric portals, and employing robust cephalomedullary intramedullary nailing, surgeons can reliably restore biomechanical stability, promote high rates of union, and facilitate early patient mobilization.
