Introduction and Historical Context
The anatomical anomaly of spondylolisthesis was first noted by Herbiniaux, a Belgian obstetrician, who observed a bony prominence anterior to the sacrum that obstructed the birth canal and complicated delivery. He is widely credited with the first clinical description of the condition. The formal medical terminology, however, was coined by Kilian in 1854. The term spondylolisthesis is derived from the Greek spondylos (meaning "vertebra") and olisthenein (meaning "to slip"). Clinically, spondylolisthesis is defined as the anterior or posterior translation of one segment of the spine over the adjacent lower segment.
While the condition can occur anywhere in the spine, it is overwhelmingly most common at the L5-S1 junction, followed by L4-L5. Understanding the intricate biomechanics, natural history, and precise surgical indications is paramount for the practicing orthopedic surgeon and neurosurgeon.
Anatomy and Biomechanics
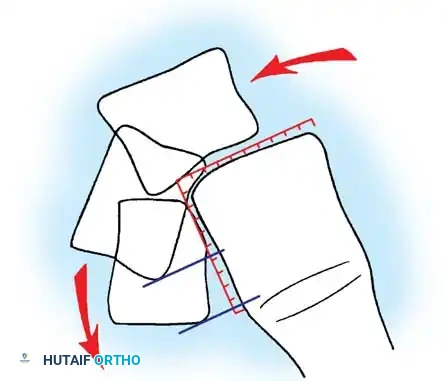
The stability of the lumbosacral junction relies heavily on the integrity of the posterior osseous and ligamentous complex. The critical anatomical structure preventing anterior translation of L5 over S1 is the "bony hook."
The bony hook is comprised of the pedicle, the pars interarticularis, the inferior articular facets of L5, and the superior articular facets of the sacrum. In a normal spine, this hook effectively resists the anterior shear forces generated by the lumbar lordosis and the sacral slope.
Biomechanics Pearl: The degree of lumbar lordosis and the position of the sagittal gravity line are critical predictors of slip progression. The further anterior the gravity line falls relative to the sacral promontory, the higher the shear forces acting on the pars interarticularis, increasing the likelihood of progressive spondylolisthesis.
Furthermore, the competency of the intervertebral disc at the affected level plays a vital role in resisting shear. Early disc degeneration or failure exacerbates instability. Magnetic Resonance Imaging (MRI) is often required to accurately assess disc hydration and structural integrity.
Etiology and Natural History
The prevalence of spondylolisthesis in the general population is approximately 5%, with an equal distribution between men and women. However, distinct genetic and biomechanical factors drive its development.
Genetic Predisposition and Biomechanical Stress
Developmental spondylolisthesis with lysis typically manifests as a stress fracture in children possessing a genetic predisposition. Notably, the defect is virtually never present at birth and is absent in chronically bedridden patients, strongly indicating an acquired mechanical etiology superimposed on genetic susceptibility.
Wiltse et al. postulated that the normal flexion contractures of the hip in early childhood accentuate lumbar lordosis, thereby concentrating weight-bearing and shear forces directly onto the pars interarticularis. Letts et al. further demonstrated that shear stresses on the pars are maximized during lumbar extension. Cyron and Hutton's biomechanical studies revealed that the pars interarticularis is structurally thinner, and the intervertebral disc less resistant to shear, in children and adolescents compared to adults.
Epidemiological data strongly supports a genetic link: up to 50% of Eskimos possess spondylolisthesis, compared to only 6% to 7% of Caucasian males and 1.1% of African American females. The condition is also disproportionately prevalent in adolescent athletes subjected to repetitive hyperextension, such as female gymnasts, interior linemen in American football, and fast bowlers in cricket.
Long-Term Natural History
The natural history of untreated spondylolysis and low-grade spondylolisthesis is overwhelmingly benign. Beutler et al. conducted a landmark 50-year prospective study (initiated by Dr. Daniel Baker) following 500 first-grade children. Initially, 4.4% exhibited a lytic pars defect, which increased to 6% by adulthood.
Key findings from the Beutler study include:
* Subjects with unilateral defects never experienced slippage.
* Progression of slippage slowed significantly with each advancing decade.
* There was no statistical correlation between slip progression and the incidence of low back pain.
* SF-36 health survey scores of the study cohort were indistinguishable from the general population.
Clinical Pearl: If slip progression is to occur, it almost exclusively happens during the adolescent growth spurt (ages 9 to 15) and is exceedingly rare after age 20. Therefore, there is no evidence-based justification for restricting asymptomatic children with spondylolysis or low-grade slips from competitive sports.
Similarly, Harris and Weinstein's long-term follow-up of untreated high-grade (Grade III and IV) slips revealed that 36% were entirely asymptomatic, 55% had only mild symptoms, and all led active lives without significant cosmetic or social dissatisfaction.
Classification Systems
Accurate classification is essential for determining prognosis and guiding surgical intervention.
Wiltse, Newman, and Macnab Classification
Historically the most widely utilized system, it categorizes the condition into five distinct types based on etiology:
- Type I (Dysplastic): Congenital abnormalities of the upper sacral facets or inferior L5 facets. No pars defect is present.
- Type II (Isthmic): Defect in the pars interarticularis. Subdivided into:
- Lytic: Stress fracture of the pars.
- Elongated: Intact but stretched pars.
- Acute Fracture: Traumatic fracture of the pars.
- Type III (Degenerative): Secondary to long-standing intersegmental instability and facet arthropathy (most common at L4-L5).
- Type IV (Traumatic): Fractures of the posterior arch other than the pars (e.g., pedicle, lamina).
- Type V (Pathological): Secondary to generalized bone disease (e.g., osteogenesis imperfecta, Paget's disease, malignancy).
Marchetti-Bartolozzi Classification
Marchetti and Bartolozzi criticized the Wiltse system for mixing etiological and topographical criteria, arguing it failed to accurately predict progression or surgical response. They proposed a system emphasizing the degree of dysplasia:
- Developmental:
- High Dysplastic: Severe dysplasia of the bony hook (with lysis or elongation). High risk of progression.
- Low Dysplastic: Mild dysplasia (with lysis or elongation).
- Acquired:
- Traumatic: Acute or stress fractures.
- Postsurgery: Direct or indirect destabilization.
- Pathological: Local or systemic.
- Degenerative: Primary or secondary.
Surgical Warning: When evaluating a patient, the surgeon must first differentiate developmental from acquired. If developmental, assessing the degree of dysplasia (high vs. low) via the integrity of the posterior bony hook is paramount. High dysplastic slips are inherently unstable and require more aggressive, heavily instrumented surgical stabilization.
Clinical Presentation
In pediatric populations, spondylolysis and low-grade spondylolisthesis are frequently asymptomatic. Presentation is often prompted by parental observation of a postural deformity or an abnormal gait.
When symptomatic, pain typically coincides with the adolescent growth spurt. The pain is predominantly mechanical axial backache, exacerbated by high-impact activity and relieved by rest. Radicular leg pain is less common but, when present, usually indicates L5 nerve root irritation (exiting root compression in the neuroforamen due to hypertrophic pseudarthrosis tissue at the pars defect).
Physical Examination
Physical findings correlate directly with the severity of the slip:
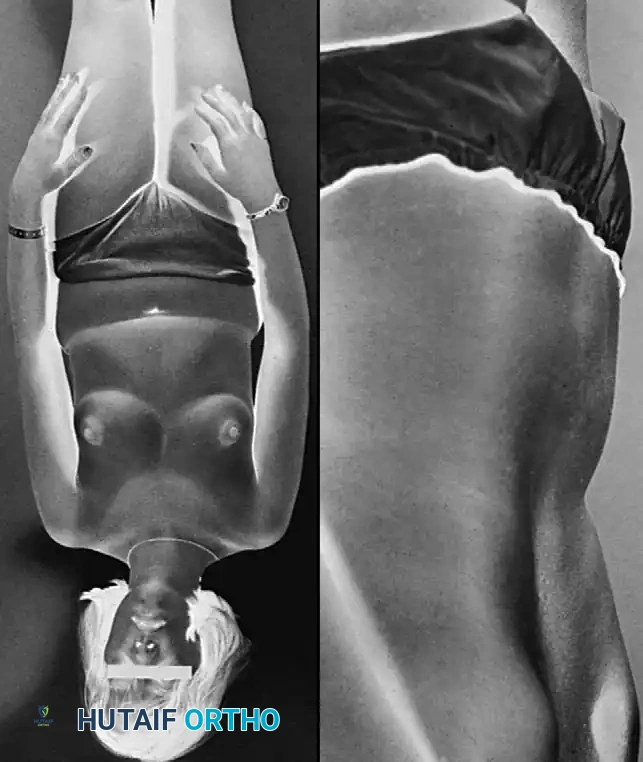
* Palpable Step-Off: A distinct shelf is palpable at the lumbosacral junction in higher-grade slips.
* Postural Compensation: As L5 translates anteriorly, the patient hyper-extends the lumbar spine above the slip to maintain sagittal balance. The sacrum becomes vertical, resulting in a "heart-shaped" appearance of the buttocks.
* Trunk Shortening: In severe slips (spondyloptosis), the trunk shortens, obliterating the waistline.
* Pelvic Waddle: Described by Newman, this peculiar spastic gait is secondary to severe hamstring tightness and lumbosacral kyphosis.
* Neurological Deficits: Unlike adults with degenerative slips, children rarely exhibit objective motor weakness, reflex changes, or sensory deficits. Hamstring tightness is often the sole positive neurological sign.
Associated Scoliosis
Scoliosis frequently coexists with pediatric spondylolisthesis and presents in three forms:
1. Sciatic Scoliosis: A non-structural, muscle-spasm-induced lumbar curve that resolves with recumbency or pain relief.
2. Olisthetic Scoliosis: A torsional lumbar curve blending into the pars defect, caused by asymmetrical slippage. It typically resolves following surgical stabilization of the slip.
3. Idiopathic Scoliosis: A concurrent but independent structural curve. Seitsalo et al. demonstrated that lumbosacral fusion for spondylolisthesis has no corrective effect on independent thoracic or thoracolumbar idiopathic curves. They must be treated as separate entities.
Radiographic Evaluation
Standard radiographic evaluation is the cornerstone of diagnosis and surgical planning.
Plain Radiography
- Standing Lateral View: Mandatory for assessing the true degree of slippage. Lowe et al. demonstrated a 26% increase in measured slip on standing films compared to supine films.
- Anteroposterior (AP) View: Evaluates for concurrent scoliosis and transverse process anatomy.
- Ferguson Coronal View: The X-ray beam is angled 30 degrees cephalad (parallel to the L5-S1 disc space). This provides a true en face view of the L5 pedicles, transverse processes, and sacral ala.
- Oblique Views: Historically used to visualize the "Scottie Dog" collar (pars defect), though largely superseded by advanced imaging for subtle lesions.
Advanced Imaging
- SPECT Bone Scan: Highly sensitive for detecting early stress reactions in the pars before a frank fracture line is visible on plain films.
- Computed Tomography (CT): The gold standard for defining osseous anatomy, confirming acute stress fractures versus chronic non-unions with sclerotic margins, and planning pedicle screw trajectories.
- Magnetic Resonance Imaging (MRI): Essential for evaluating disc hydration, central canal stenosis, and foraminal compromise affecting the L5 nerve root.



Radiographic Grading Systems
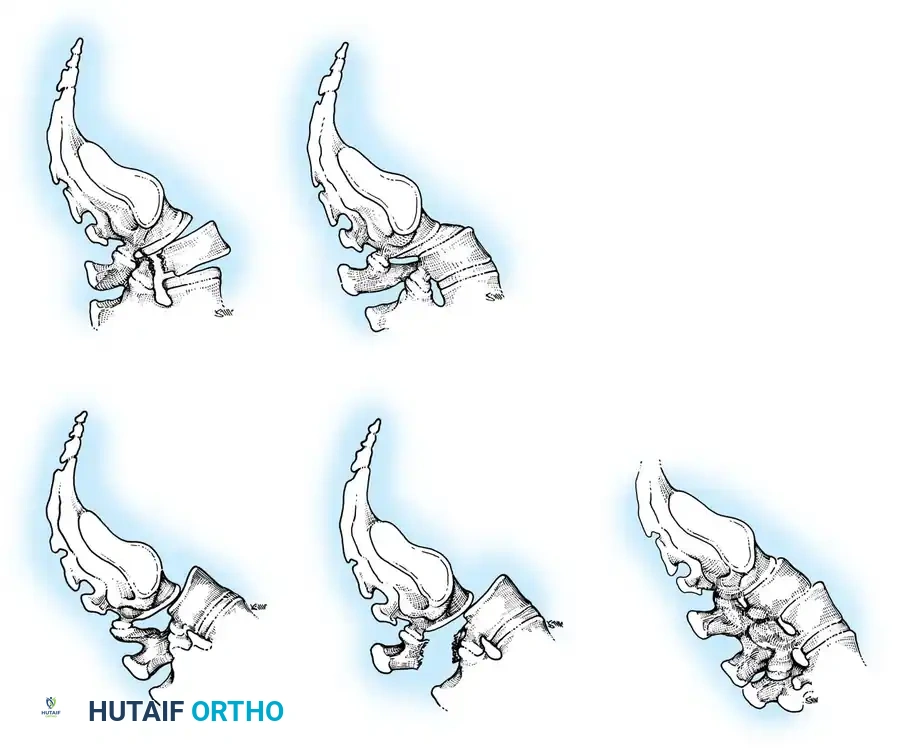
Meyerding Classification:
The most universally applied system. The superior endplate of S1 is divided into four equal quarters. The grade is determined by the position of the posterior-inferior corner of L5 relative to S1.
* Grade I: < 25% slip
* Grade II: 25% - 50% slip
* Grade III: 50% - 75% slip
* Grade IV: > 75% slip
* Grade V (Spondyloptosis): L5 is completely displaced anterior and inferior to the sacral promontory.
DeWald Modification:
DeWald modified Newman's system to better quantify the anterior "roll" or kyphosis of L5. The sacral dome and anterior sacral surface are divided into 10 equal parts, providing a highly precise two-number score mapping both translation and angular displacement.

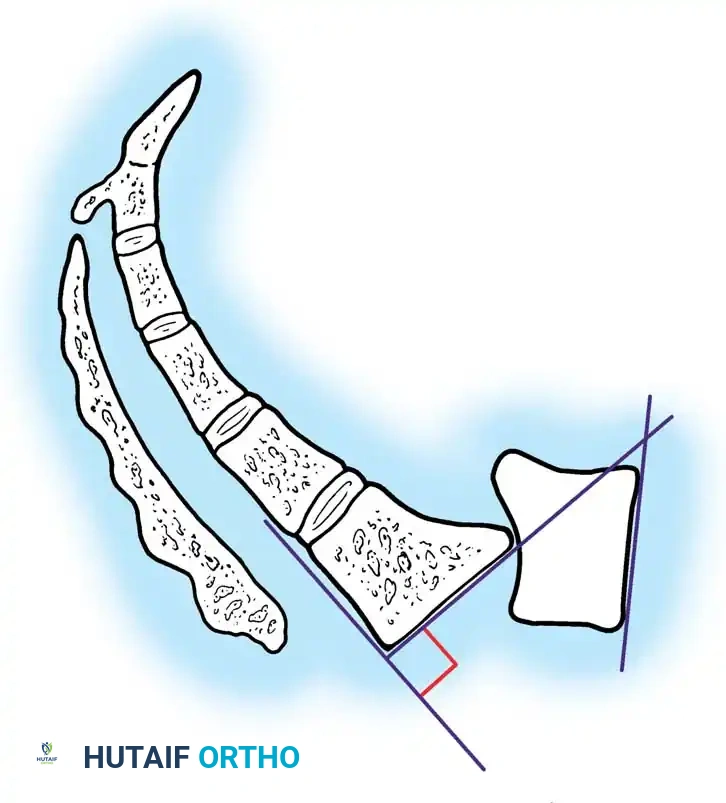
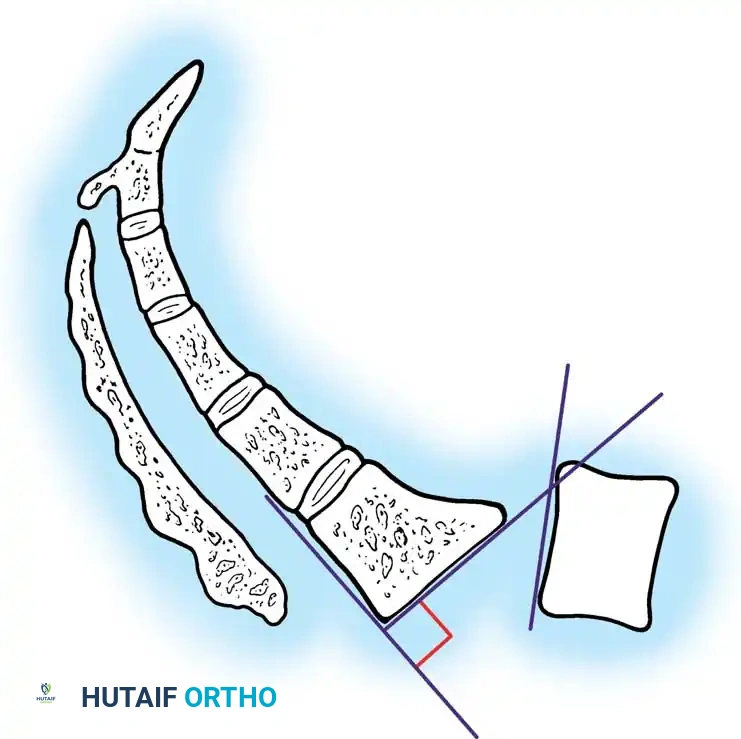
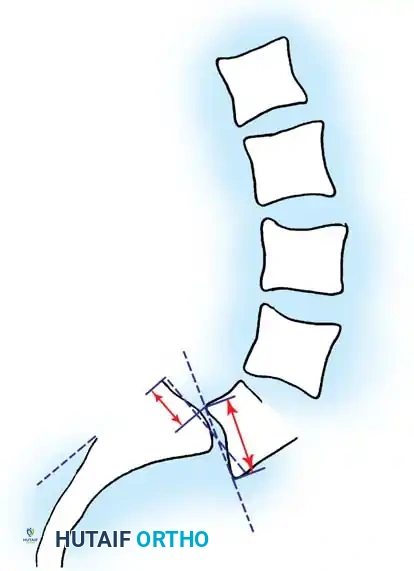
Boxall's Slip Angle:
Boxall et al. established that angular relationships (sagittal rotation or slip angle) are superior predictors of instability and progression compared to simple translational percentage. A high slip angle indicates severe localized lumbosacral kyphosis.


Surgical Management
Indications for Surgery
While conservative management (activity modification, NSAIDs, physical therapy, and rigid antilordotic bracing) is the first line of treatment for symptomatic low-grade slips, surgical intervention is indicated in the following scenarios:
1. Persistent, intractable back or leg pain failing 6 months of conservative care.
2. Progressive slip beyond Grade II (50%) in a growing child.
3. Presentation with a high-grade slip (Grade III, IV, or V), regardless of symptoms, due to the high risk of progression and sagittal imbalance.
4. Objective, progressive neurological deficit (e.g., foot drop, bowel/bladder dysfunction).
5. Severe postural deformity and gait abnormality (pelvic waddle).
Preoperative Planning and Positioning
Comprehensive preoperative planning requires full-length standing scoliosis films to calculate pelvic parameters (Pelvic Incidence, Pelvic Tilt, Sacral Slope).
The patient is positioned prone on a radiolucent Jackson spinal table. The abdomen must hang completely free to decrease intra-abdominal pressure, thereby reducing epidural venous engorgement and intraoperative bleeding. Hips are extended to maximize lumbar lordosis during the fusion phase.
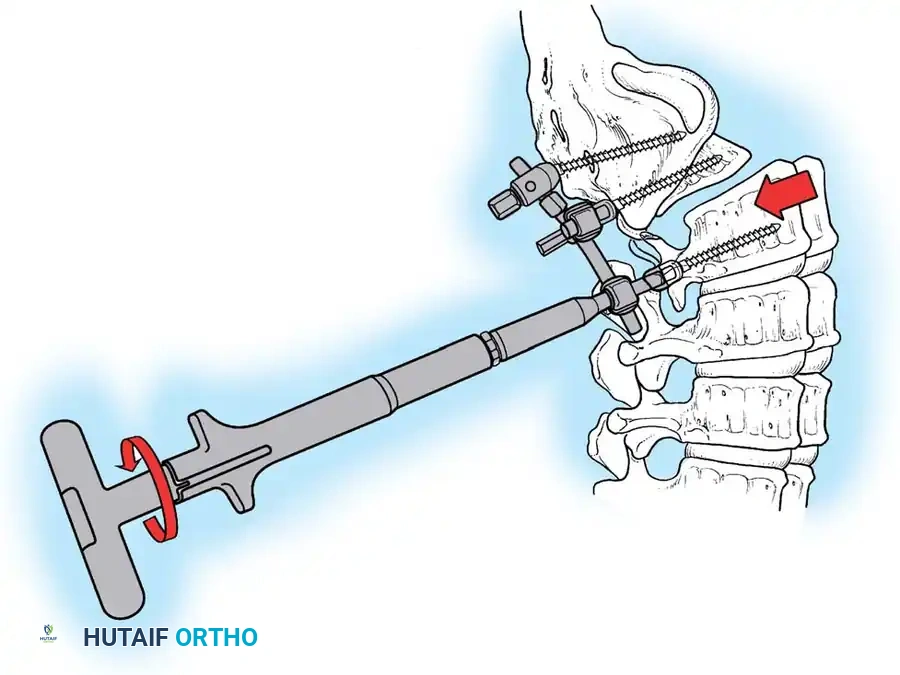
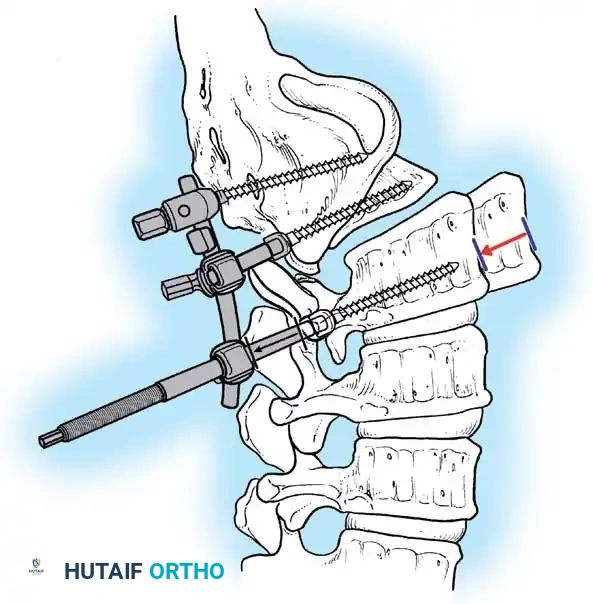
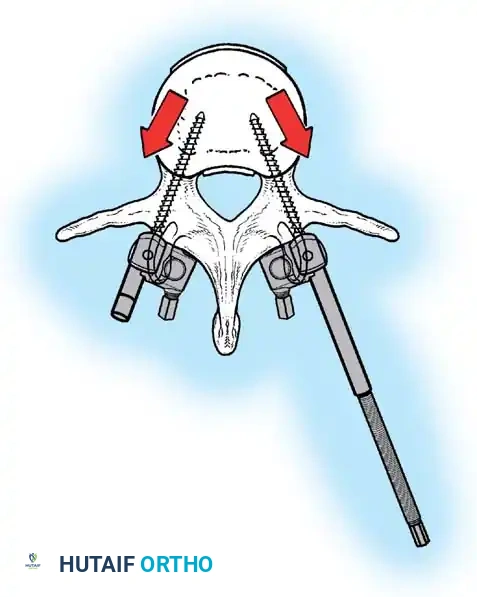
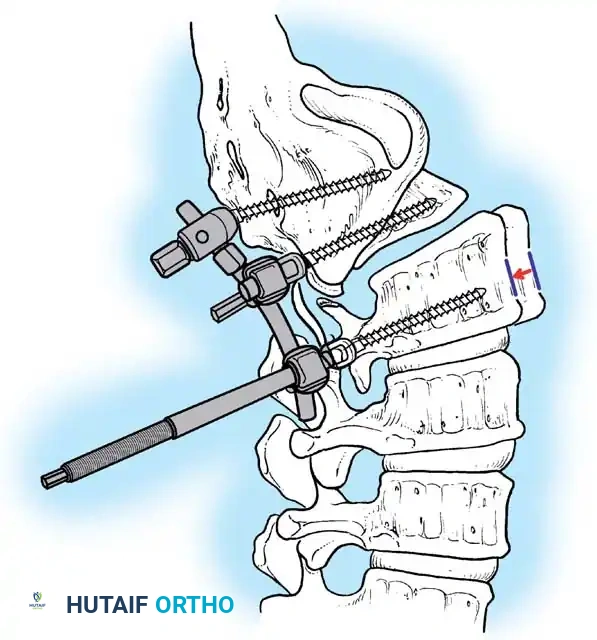
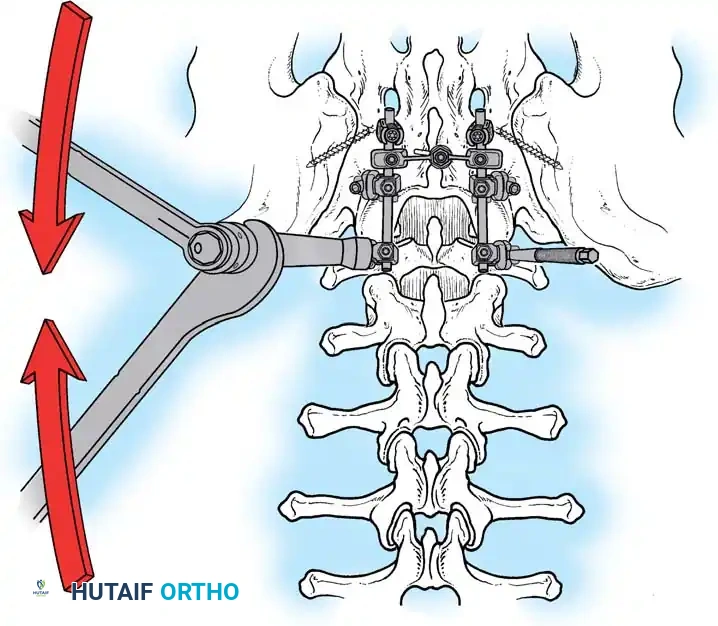
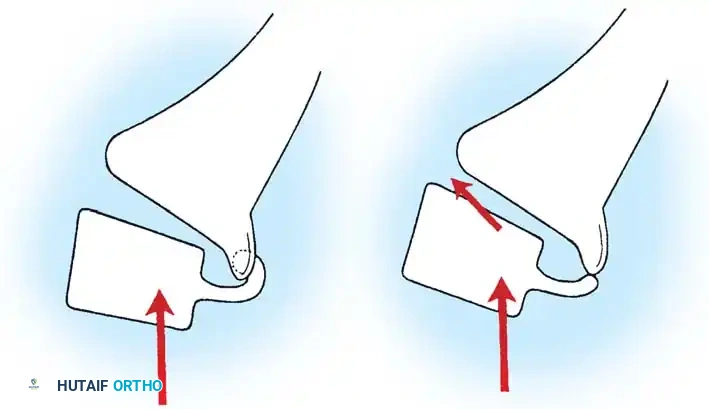
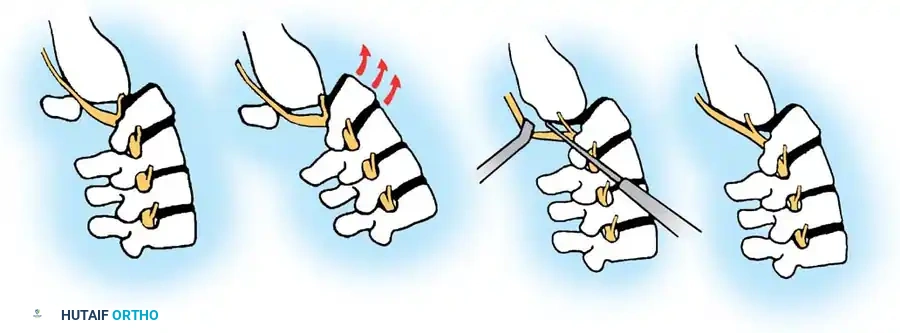
Surgical Approach and Decompression
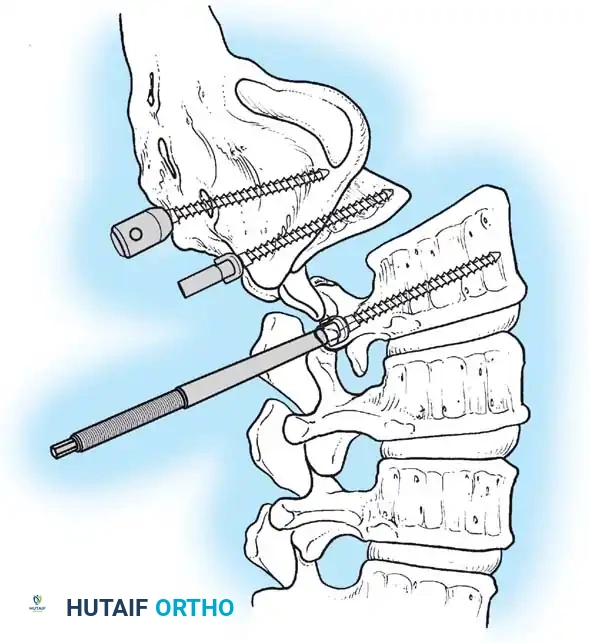
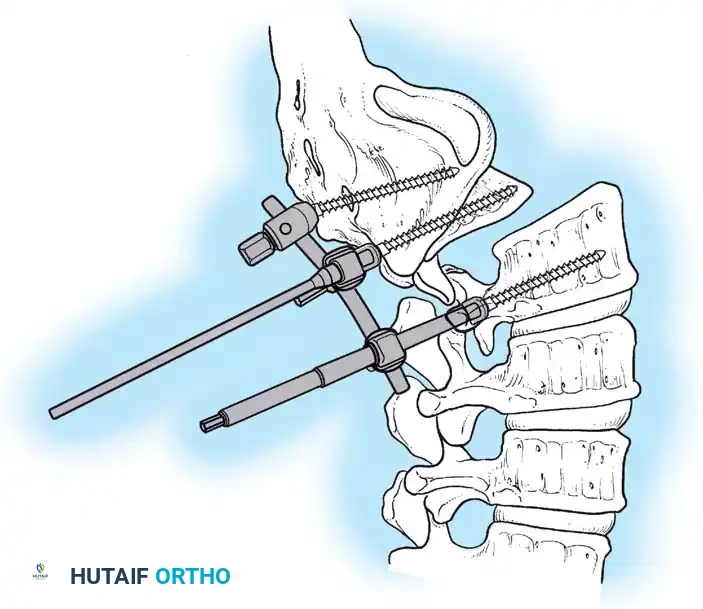
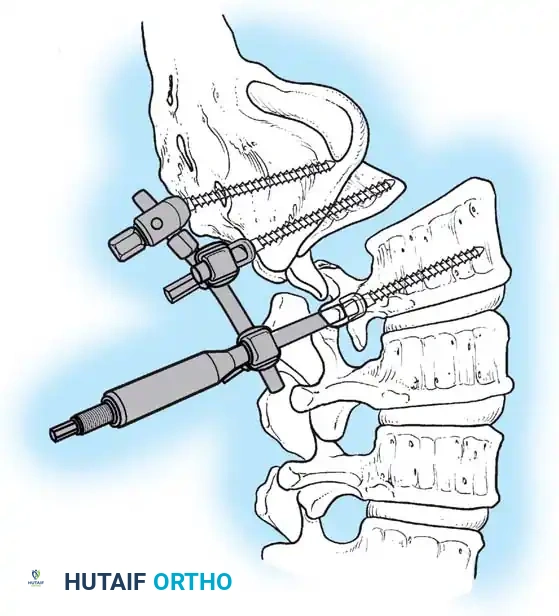
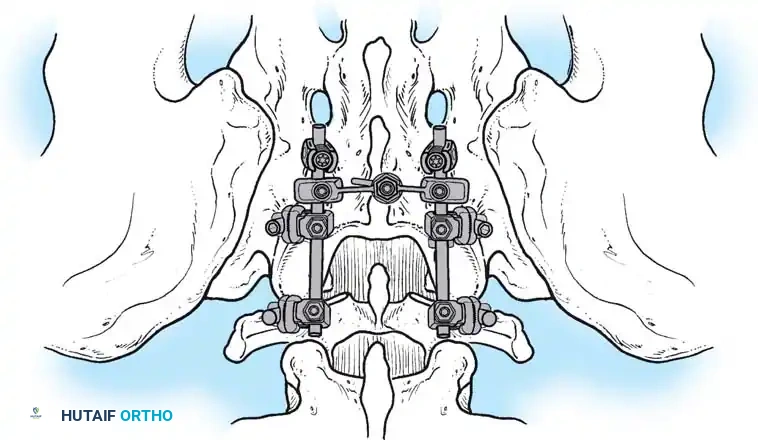
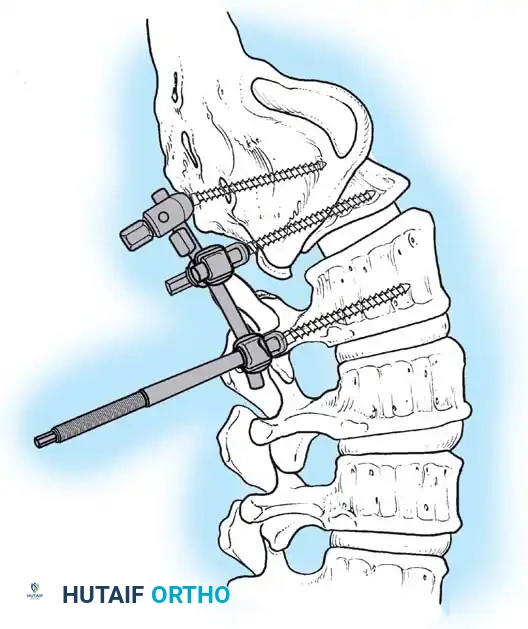
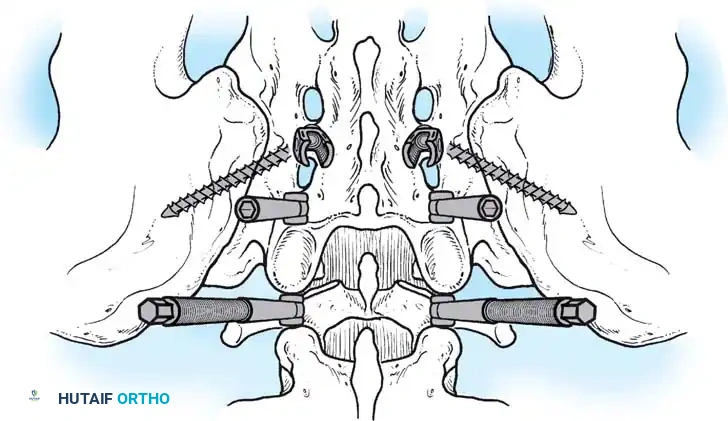
A standard posterior midline incision is utilized. Subperiosteal dissection exposes the spinous processes, laminae, pars interarticularis, and transverse processes of L4, L5, and the sacral ala.
Surgical Pitfall: In severe dysplastic slips, the anatomy is grossly distorted. The L5 lamina
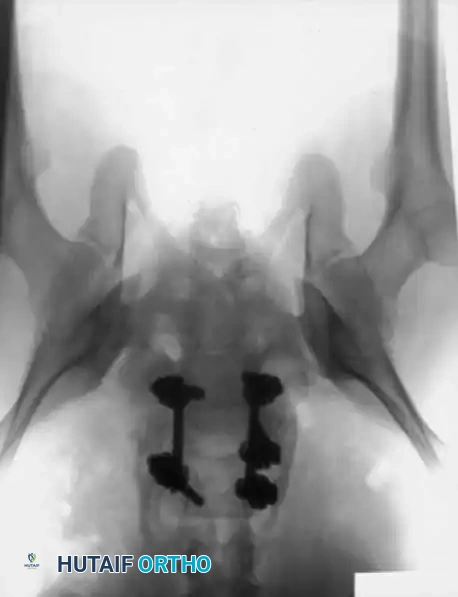
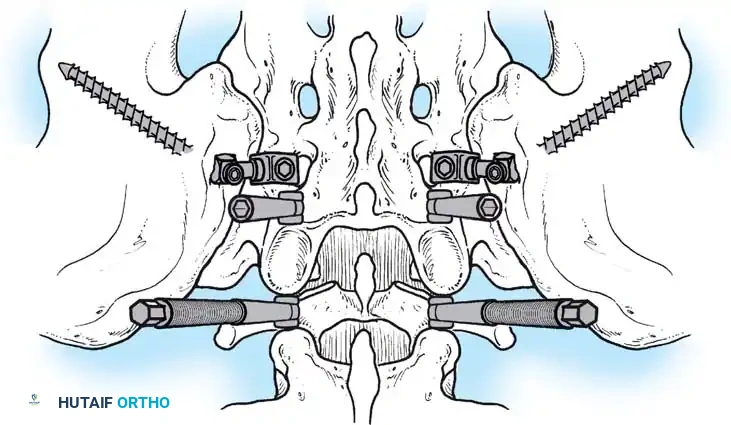
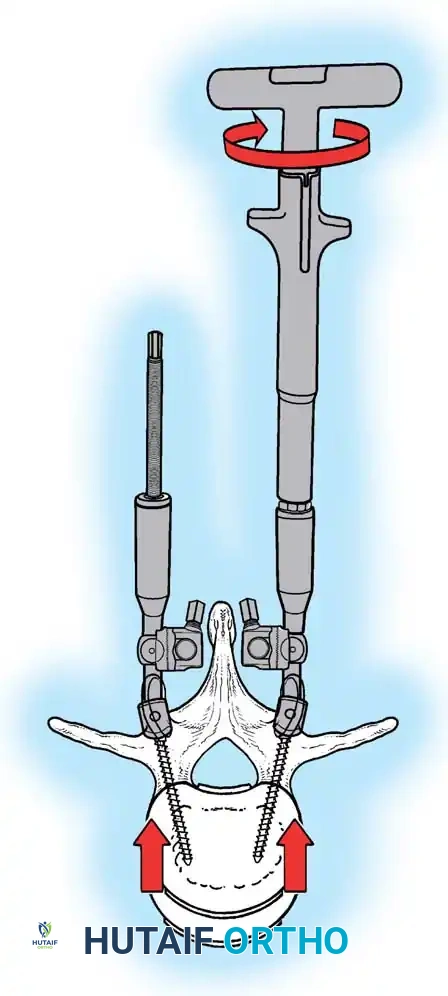
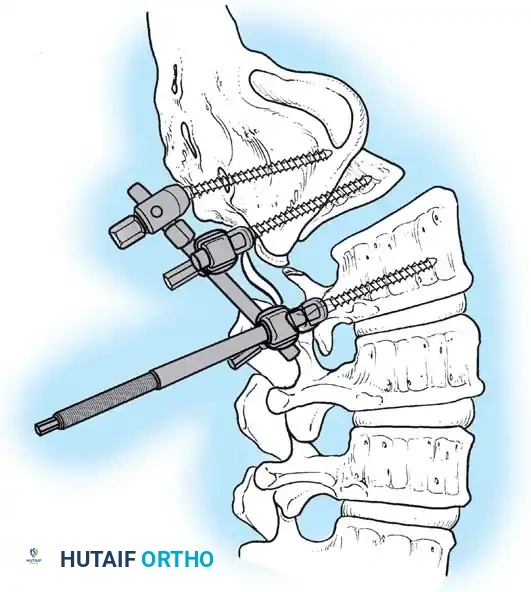
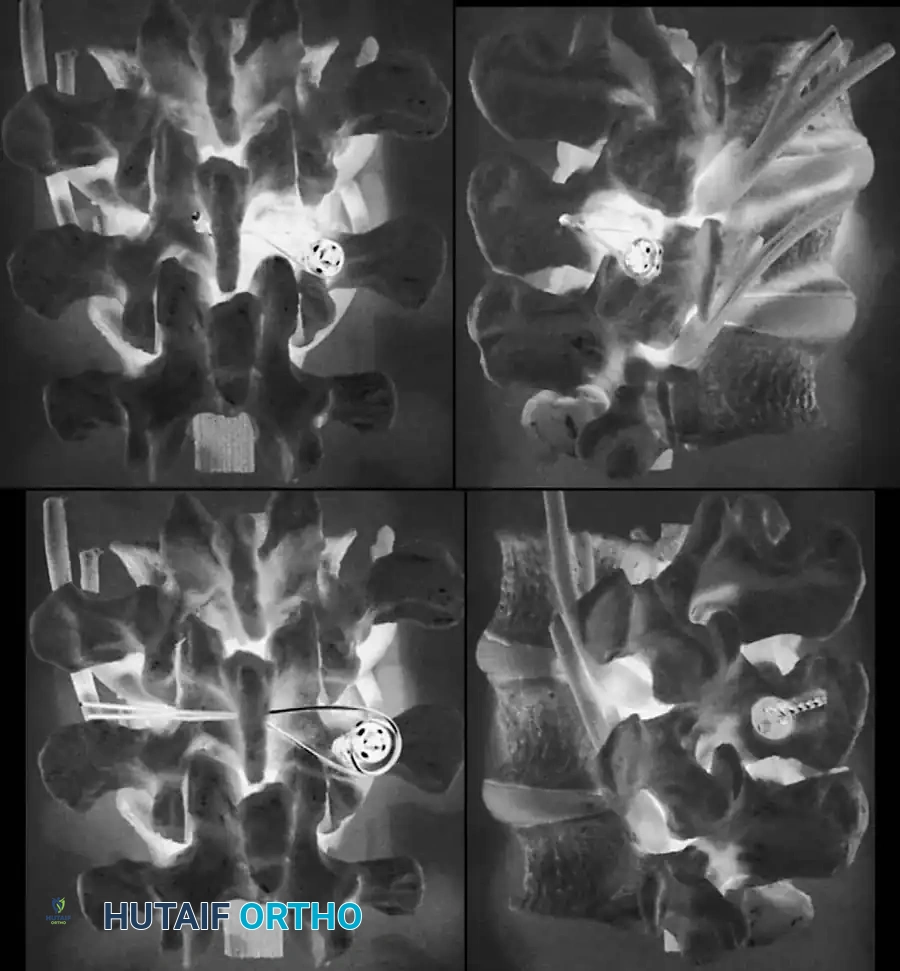
Associated Surgical & Radiographic Imaging