Lumbar Spinal Stenosis: Comprehensive Pathoanatomy and Surgical Management

Key Takeaway
Lumbar spinal stenosis is a progressive narrowing of the spinal canal, lateral recess, or neural foramina, leading to compression of neural elements. Clinically presenting as neurogenic claudication, it is primarily driven by the degenerative cascade involving facet hypertrophy, disc bulging, and ligamentum flavum thickening. Surgical management, primarily via decompressive laminectomy with or without fusion, is indicated for patients with severe, refractory symptoms, offering significant improvements in pain and functional endurance.
Introduction and Historical Context
Before the advent of advanced cross-sectional imaging, paralysis and severe lower extremity dysfunction caused by the narrowing of the spinal canal were only sporadically reported in the medical literature. The first verifiable report of lumbar spinal stenosis successfully treated by a two-level laminectomy was published by Sachs and Fraenkel in 1900. Subsequently, Bailey and Casamajor (1911) and Elsberg (1913) provided similar descriptions of the pathological findings and the profound relief afforded by surgical decompression.
However, the syndrome was not universally understood or systematically diagnosed until Verbiest’s landmark publication in 1954. Verbiest described the classic pathognomonic findings in middle-aged and older adults: back and lower extremity pain precipitated by standing and walking, and characteristically aggravated by lumbar hyperextension. Verbiest delineated congenital narrowing of the spinal canal as a primary contributing factor, upon which the secondary development of degenerative changes precipitated symptomatic neural compression. Since that time, the pathophysiology of degenerative spinal stenosis has been recognized as a progressive disorder involving the entire spinal motion segment.
Pathoanatomy and Biomechanics
Degenerative spinal stenosis is initiated by the degenerative cascade of the intervertebral disc. As the disc desiccates and loses height, relative instability and hypermobility of the facet joints ensue. Dunlop, Adams, and Hutton demonstrated in a seminal cadaveric study that disc space narrowing, combined with increasing angles of extension, leads to a significant exponential increase in pressure on the facet joints.
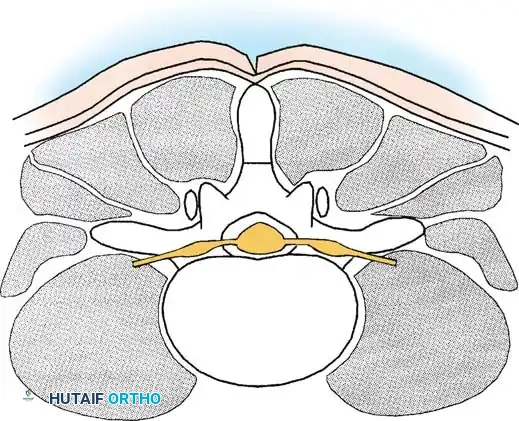
This abnormal load transmission stimulates hypertrophy of the facet joint, particularly the superior articular process (SAP). As joint destruction progresses, the hypertrophic process may ultimately result in local ankylosis. Concurrently, the ligamentum flavum undergoes hypertrophy and buckling due to the loss of disc height. The anatomical end-result is a critical reduction in spinal canal dimensions, leading to mechanical compression of the neural elements and localized venous congestion. This venous hypertension within the nerve roots is widely considered the primary biochemical and physiological driver of intermittent neurogenic claudication.
Anatomical Zones of Stenosis
A precise description of spinal stenosis requires a rigorous understanding of the affected anatomy and the use of standardized terminology. Stenosis can be categorized by the anatomical region of the vertebral segment affected.
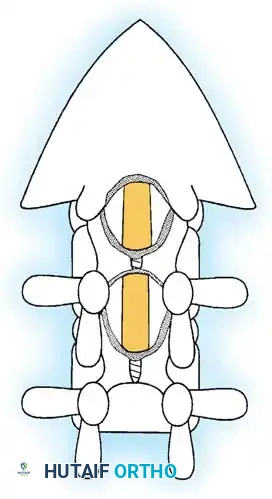
Central Spinal Stenosis:
This denotes involvement of the area between the facet joints, occupied by the thecal sac and its contents. Stenosis in this region is typically caused by a combination of a bulging annulus, osteophyte formation, and a buckled, thickened ligamentum flavum. Symptomatic central stenosis classically results in bilateral neurogenic claudication.
Lateral Canal Stenosis:
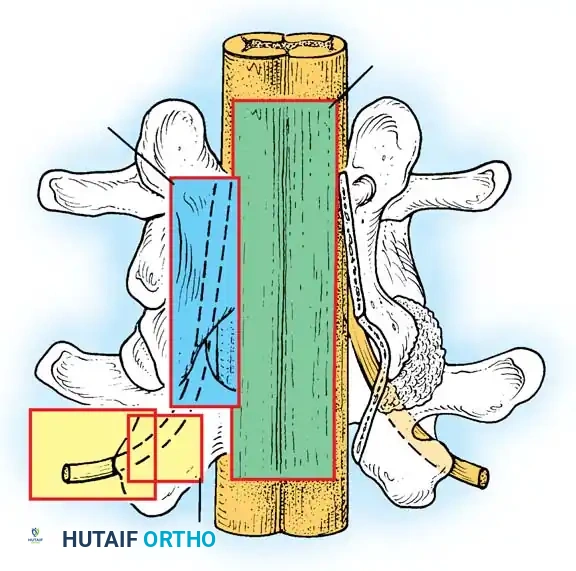
Lateral to the dura is the lateral canal, which contains the exiting nerve roots. Compression in this region results in radiculopathy. The lateral canal is further subdivided into three distinct zones, originally described by Lee:
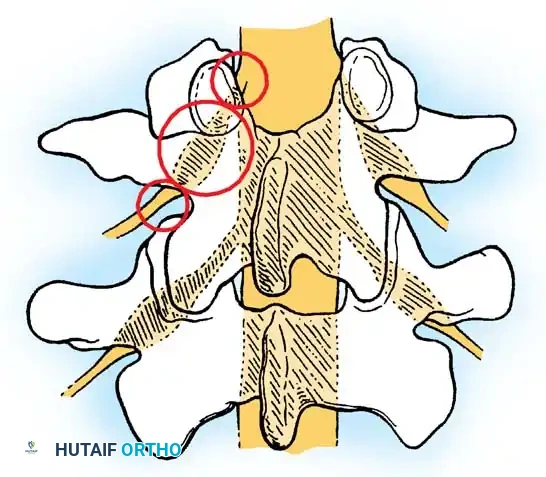
- The Lateral Recess (Entrance Zone): Begins at the lateral border of the dura and extends to the medial border of the pedicle. The borders are the pedicle laterally, the superior articular facet dorsally, the disc and posterior longitudinal ligament ventrally, and the central canal medially. Facet arthritis and hypertrophy of the superior articular process most frequently cause stenosis in this zone.
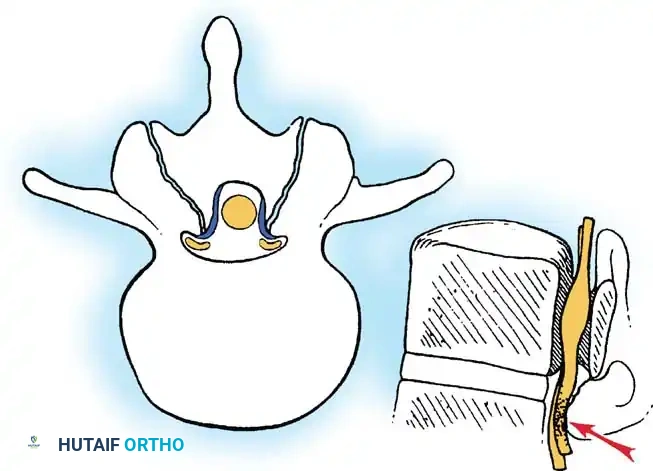
- The Foraminal Region (Midzone): Lies ventral to the pars interarticularis. Its borders are the lateral recess medially, the posterior vertebral body and disc ventrally, the pars dorsally, and the lateral border of the pedicle laterally. The dorsal root ganglion (DRG) and ventral motor root occupy approximately 30% of this space.
- The Extraforaminal Region (Exit Zone): Identified as the area lateral to the facet joint. The nerve root can be compressed here by a "far-lateral" disc herniation, degenerative spondylolisthesis, or lateral facet osteophytes.
Clinical Pearl: When evaluating a patient with dermatomal radiculopathy rather than classic bilateral claudication, maintain a high index of suspicion for isolated lateral recess or foraminal stenosis. The L4-L5 level is the most commonly involved, followed by L5-S1 and L3-L4.
Classification of Spinal Stenosis
Spinal stenosis is broadly classified into congenital and acquired forms.
Congenital Stenosis
Congenital spinal stenosis is usually central and evident on early imaging studies. Idiopathic congenital narrowing typically involves a reduction in the anteroposterior (AP) dimension of the canal secondary to congenitally short pedicles. In achondroplasia, the canal is narrowed in both the AP plane (shortened pedicles) and the lateral diameter (diminished interpedicular distance).
Acquired Stenosis
Acquired forms are predominantly degenerative. This process is most commonly localized to the facet joints and ligamentum flavum.
* Degenerative Spondylolisthesis: Frequently exacerbates canal narrowing, particularly at L4-L5 in older females with sagittally oriented facets.
* Iatrogenic: Post-laminectomy instability or adjacent segment disease post-fusion.
* Metabolic/Systemic: Paget disease, fluorosis, and Diffuse Idiopathic Skeletal Hyperostosis (DISH) can result in acquired stenosis. Paget disease is notable as it often responds well to medical management with calcitonin or bisphosphonates.
Natural History
The natural history of most forms of spinal stenosis is characterized by an insidious, slowly progressive development of symptoms. Crucially, not all patients with radiographic narrowing develop clinical symptoms.
Observational studies have demonstrated that a significant percentage of patients remain stable over time. Johnsson et al. reported that 70% of patients with moderate, untreated spinal stenosis remained unchanged after 4 years of observation. In a landmark prospective randomized study by Amundsen et al., pain relief was noted after 3 months in most patients regardless of treatment modality. However, at 4-year follow-up, 80% of patients treated operatively maintained good results, compared to only 50% of those treated nonoperatively.
Surgical Warning: Worsening of neurological symptoms, progressive motor weakness, or the onset of cauda equina syndrome despite adequate conservative treatment are absolute indications for urgent operative intervention.
Clinical Evaluation
The hallmark symptom of central spinal stenosis is neurogenic claudication, characterized by pain, heaviness, or cramping in the buttocks, thighs, and calves that is exacerbated by standing or walking and relieved by sitting or lumbar flexion.
Differentiating Neurogenic vs. Vascular Claudication
Differentiation between neurogenic and vascular claudication is a critical component of the orthopedic evaluation:
* Vascular Claudication: Symptoms are typically felt in the calf muscles, are brought on by a specific distance of walking, and are relieved rapidly (within 5 minutes) by simply standing still. Walking uphill exacerbates the pain due to increased metabolic demand.
* Neurogenic Claudication: Symptoms improve with trunk flexion, stooping, or lying down, but may require up to 20 minutes of rest to fully resolve. Patients often report better endurance when walking uphill, pushing a grocery cart, or riding a stationary bicycle, as these activities promote lumbar flexion, which transiently increases the cross-sectional area of the spinal canal.
Physical examination findings may be subtle. Patients often exhibit a "simian stance" (slight hip and knee flexion with a forward-flexed trunk). Neurological deficits may only become apparent after the patient is asked to walk until symptoms are reproduced (the "stress test").
Imaging and Diagnostics
Advanced imaging is mandatory for surgical planning.
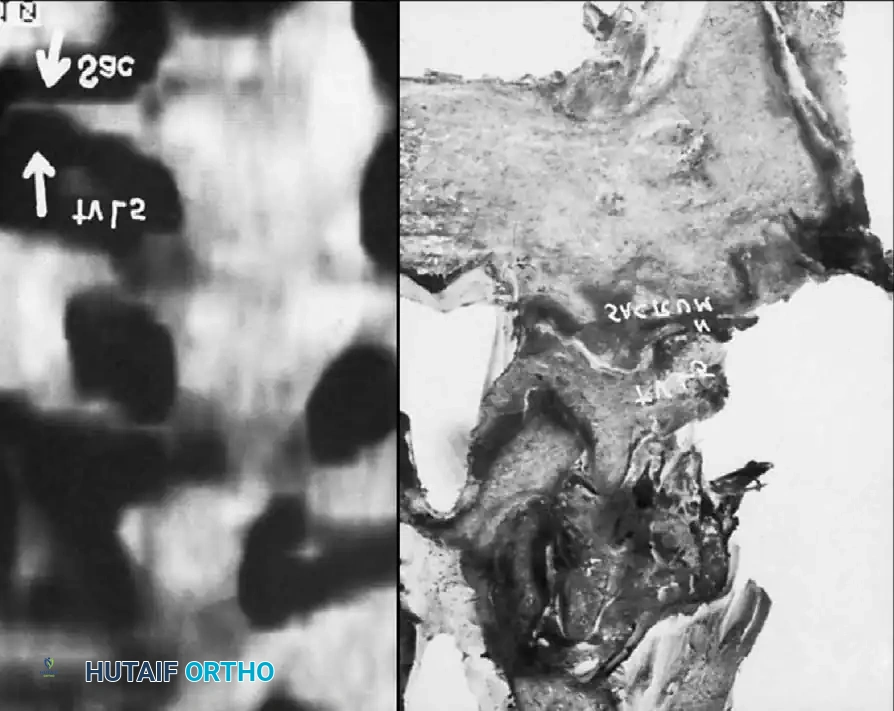
Magnetic Resonance Imaging (MRI):
MRI is the gold standard, providing excellent soft-tissue contrast to evaluate the intervertebral discs, ligamentum flavum, and neural elements. T2-weighted axial and sagittal images are critical for assessing the degree of cerebrospinal fluid (CSF) effacement and nerve root compression.

Computed Tomography (CT) and CT Myelography:
CT is invaluable for assessing bony anatomy, facet hypertrophy, and ossification of the posterior longitudinal ligament (OPLL). CT myelography is reserved for patients with contraindications to MRI (e.g., incompatible pacemakers) or those with significant prior spinal instrumentation causing MRI artifact.
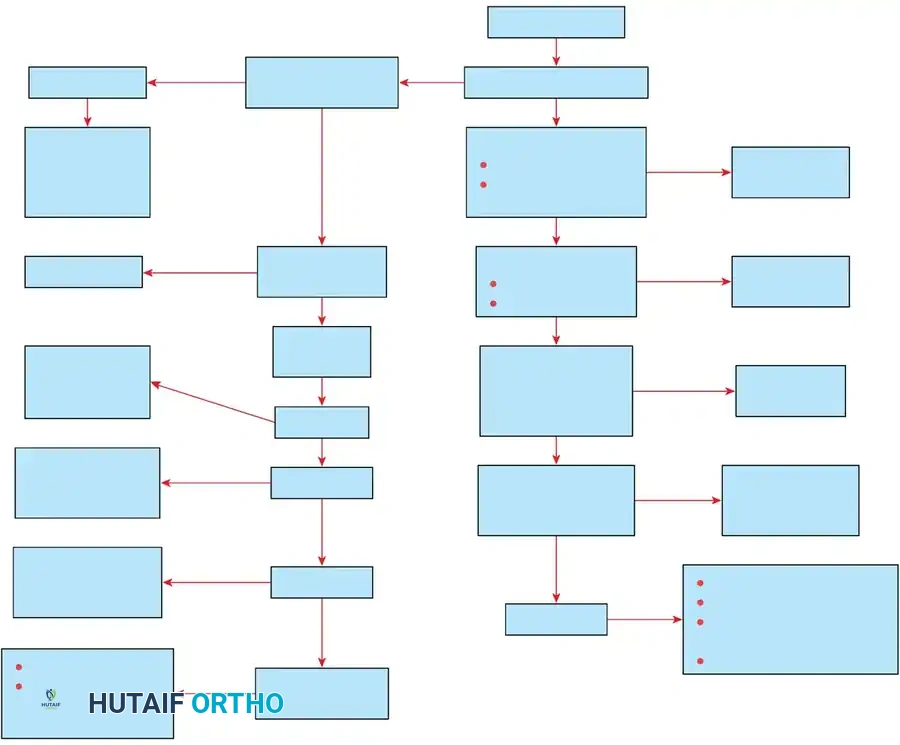
Treatment Algorithm
Management of lumbar spinal stenosis should follow a stepwise, evidence-based algorithm.
- Conservative Management: First-line treatment includes NSAIDs, physical therapy (focusing on core strengthening and flexion-based exercises), and lifestyle modifications. Epidural steroid injections (ESIs) may provide temporary symptomatic relief and serve as a diagnostic tool.
- Surgical Intervention: Indicated for patients with refractory pain, progressive neurological deficits, or profound functional limitations that fail to improve after 3 to 6 months of comprehensive conservative care.
Surgical Management: Operative Technique
The primary goal of surgery is the meticulous decompression of the neural elements while preserving spinal stability. The gold standard remains the decompressive laminectomy, though minimally invasive techniques are increasingly utilized.
Preoperative Positioning
Proper positioning is critical to minimize intraoperative bleeding. The patient is placed prone on a radiolucent Jackson table or Wilson frame. The abdomen must hang completely free; any abdominal compression increases intra-abdominal pressure, which is transmitted to the epidural venous plexus (Batson's plexus), resulting in excessive epidural bleeding.
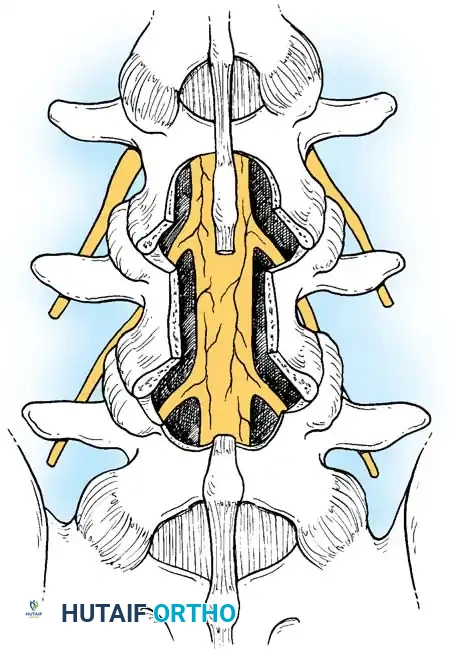
The Standard Open Laminectomy
1. Exposure:
A midline longitudinal incision is made over the affected levels, confirmed by intraoperative fluoroscopy. Subperiosteal dissection of the paraspinal musculature is performed bilaterally to expose the spinous processes, laminae, and medial aspect of the facet joints.
2. Bony Resection:
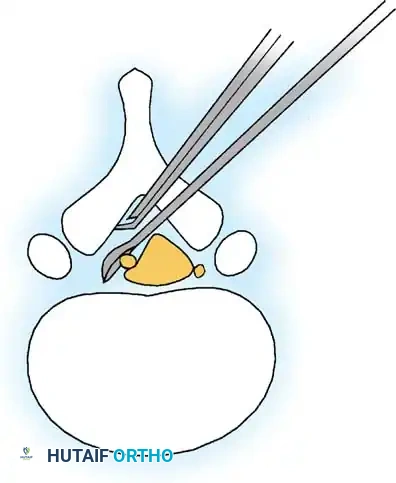
The spinous processes and interspinous ligaments are resected using a Leksell rongeur or a high-speed burr. The laminectomy is initiated by thinning the lamina. A Kerrison rongeur is then used to carefully resect the remaining lamina and the hypertrophied ligamentum flavum.
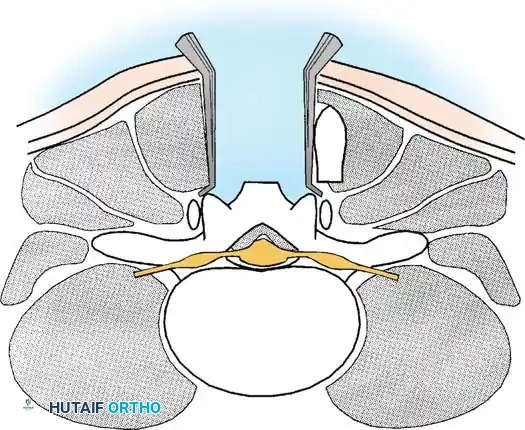
3. Undercutting Facetectomy and Lateral Recess Decompression:
To decompress the lateral recess without causing iatrogenic instability, an "undercutting" technique is employed. The medial aspect of the superior articular process is resected using a Kerrison rongeur.
Surgical Pitfall: Resection of more than 50% of the pars interarticularis or the facet joint complex significantly increases the risk of postoperative iatrogenic spondylolisthesis. Always angle the Kerrison rongeur laterally to undercut the facet rather than resecting it dorsally.

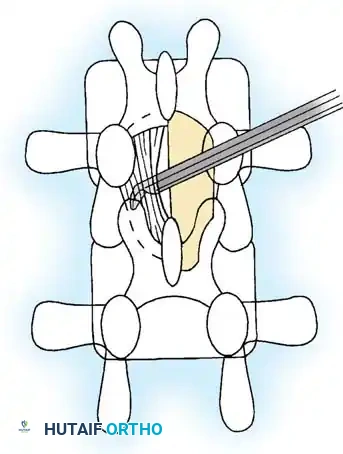
4. Foraminotomy:
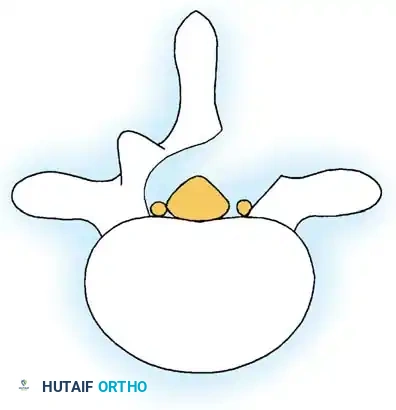
The exiting nerve root is identified and followed into the neural foramen. A Woodson elevator or a nerve hook is used to palpate the pedicle and ensure the foramen is widely patent. The decompression is complete when the thecal sac expands and the nerve roots are completely free of tension.
Minimally Invasive (Tubular) Decompression
For select patients, minimally invasive surgery (MIS) utilizing tubular retractors offers the advantage of decreased muscle crush injury, reduced blood loss, and faster postoperative recovery.
Technique:
Under fluoroscopic guidance, a sequential dilation system is introduced over the target lamina, and a tubular retractor is docked. Using a surgical microscope, a unilateral laminotomy is performed. By angling the microscope and the tube medially, the base of the spinous process is undercut, allowing for a bilateral decompression via a unilateral approach (the "over-the-top" technique).
The Role of Concomitant Fusion
Decompression alone is sufficient for the majority of patients with isolated spinal stenosis. However, concomitant instrumented posterolateral fusion (with or without interbody fusion) is indicated in the following scenarios:
* Preoperative dynamic instability (e.g., >3mm of translation or >10 degrees of angular change on flexion-extension radiographs).
* Degenerative spondylolisthesis with associated mechanical back pain.
* Iatrogenic instability created during the decompression (resection of >50% of bilateral facets).
* Stenosis associated with degenerative scoliosis requiring deformity correction.
Postoperative Protocol and Rehabilitation
Immediate Postoperative Phase (0-2 Weeks):
Patients are mobilized on the day of surgery or postoperative day one. A lumbar corset may be used for comfort but is not strictly required unless a fusion was performed. The primary focus is on early ambulation to prevent deep vein thrombosis (DVT) and pulmonary complications. Bending, lifting (greater than 10 lbs), and twisting are restricted.
Intermediate Phase (2-6 Weeks):
Once the surgical incision has healed, patients begin a formal physical therapy program. The initial focus is on neural mobilization, gentle core activation (transversus abdominis), and cardiovascular endurance (stationary cycling or aquatic therapy).
Long-Term Rehabilitation (6+ Weeks):
Therapy progresses to dynamic core stabilization, lumbar extensor strengthening, and functional restoration. Patients are generally cleared to return to full activities, including golf and recreational sports, by 3 to 6 months postoperatively, depending on the extent of the surgery and whether a fusion was performed.
Complications
While decompressive laminectomy is highly successful, surgeons must be prepared to manage potential complications:
* Incidental Durotomy: The most common intraoperative complication (incidence 5-10%). It must be recognized and repaired primarily with 4-0 or 5-0 non-absorbable suture. A Valsalva maneuver should be performed to confirm a watertight seal. Postoperatively, the patient may be kept flat for 24-48 hours to prevent a CSF fistula.
* Epidural Hematoma: Can cause acute postoperative cauda equina syndrome. Meticulous hemostasis using bipolar electrocautery and hemostatic agents (e.g., Gelfoam, thrombin) is essential.
* Wrong-Level Surgery: Prevented by rigorous adherence to intraoperative fluoroscopic localization protocols prior to any bony resection.
Conclusion
Lumbar spinal stenosis is a pervasive degenerative condition that significantly impairs the quality of life in the aging population. A profound understanding of the complex pathoanatomy—specifically the interplay between disc degeneration, facet hypertrophy, and ligamentum flavum buckling—is essential for accurate diagnosis. When conservative measures fail, meticulous surgical decompression, tailored to the patient's specific anatomical zones of stenosis and stability profile, provides excellent, durable clinical outcomes.
📚 Medical References
- lumbar spinal stenosis: analysis of the cortical evoked poten- tials, microvasculature, and histopathology, J Bone Joint Surg 72A:110, 1990.
- Del Bigio MR, Johnson GE: Clinical presentation of spinal cord concussion, Spine 14:37, 1989.
- Denis F: The three-column spine and its signifi cance in the classifi cation of acute thoracolumbar spinal injuries, Spine 8:817, 1983.
- Denis F, Armstrong GWD, Searls K, et al: Acute thoracolumbar burst fractures in the absence of neurologic defi cit (a comparison between operative and nonoperative treatment), Clin Orthop Relat Res 189:142, 1984.
- Denis F, Burkus JK: Diagnosis and treatment of cauda equina entrapment in the vertical lamina fracture of lumbar burst fractures, Spine 16:S433, 1991.
- Denis F, Burkus JK: Shear fracture-dislocations of the thoracic and lumbar spine associated with forceful hyperextension (lumberjack paraplegia), Spine 17:156, 1992.
- Denis F, Davis S, Comfort T: Sacral fractures: an important problem, though frequently undiagnosed and untreated: retrospective analysis of two hundred and three consecutive cases, Orthop Trans 11:118, 1987.
- Denis F, Fuiz H, Searls K: Comparison between square-ended distraction rods and standard round-ended distraction rods in the treatment of thoracolumbar spinal injuries: a statistical analysis, Clin Orthop Relat Res 189:162, 1984.
- Devilee R, Sanders R, de Lange S: Treatment of fractures and dislocations of the thoracic and lumbar spine by fusion and Harrington instrumentation, Arch Orthop Trauma Surg 114:100, 1995.
- Deramond H, Mathis JM: Vertebroplasty in osteoporosis, Semin Musculoskelet Radiol 6:263, 2002.
- DeWald RL: Burst fractures of the thoracic and lumbar spine, Clin Orthop Relat Res 189:150, 1984.
- Deyo RA, Cherkin DC, Loeser JD, et al: Morbidity and mortality in association with operations on the lumbar spine, J Bone Joint Surg 74A:536, 1992.
- Dick W: The “fi xateur interne” as a versatile implant for spine surgery, Spine 12:882, 1987.
- Dickman CA, Yahiro MA, Lu HTC, et al: Surgical treatment alternatives for fi xation of unstable fractures of the thoracic and lumbar spine: a meta-analysis, Spine 19(suppl):2266, 1994.
- Dickson JH, Harrington PR, Erwin WD: Harrington instrumentation in the fractured, unstable thoracic and lumbar spine, Texas Med 69:91, 1973.
- Dickson JH, Harrington PR, Erwin WD: Results of reduction and stabilization of the severely fractured thoracic and lumbar spine, J Bone Joint Surg 60A:799, 1978.
- Dietemann JL, Runge M, Dosh JC, et al: Radiology of posterior lumbar apophyseal ring fractures: report of 13 cases, Neuroradiology 30:337, 1988.
- Dimar JR II, Wilde PH, Glassman SD, et al: Thoracolumbar burst fractures treated with combined anterior and posterior surgery, Am J Orthop 25:159, 1996.
- Doerr TE, Montesano PX, Burkus JK, et al: Spinal canal decompression in traumatic thoracolumbar burst fractures: posterior distraction rods versus transpedicular screw fi xation, J Orthop Trauma 5:403, 1991.
- Donovan DJ, Polly DW Jr, Ondra SL: The removal of a transdural pedicle screw placed for thoracolumbar spine fracture, Spine 21:2495, 1996.
- Drummond D, Gaudagni J, Keene JS, et al: Interspinous process segmental spinal instrumentation, J Pediatr Orthop 4:397, 1984.
- Drummond D, Keene J: A technique of segmental spinal instrumentation without the passing of sublaminar wires, Mediguide Orthop 6:1, 1985.
- Drummond D, Keene JS, Breed A: The Wisconsin system: a technique of interspinous segmental spinal instrumentation, Contemp Orthop 8:29, 1984.
- Ebelke DK, Asher MA, Neff JR, et al: Survivorship analysis of VSP spine instrumentation in the treatment of thoracolumbar and lumbar burst fractures, Spine 16:S432, 1991.
- Ebraheim NA, Biyani A, Salpietro B: Zone III fractures of the sacrum: a case report, Spine 21:2390, 1996.
- Edwards CC, Levine AM: Early rod-sleeve stabilization of the injured thoracic and lumbar spine, Orthop Clin North Am 17:327, 1986.
- Edwards CC, Levine AM: Complications associated with posterior instrumentation for thoracolumbar injuries and their prevention, Semin Spine Surg 5:108, 1993.
- Eismont FJ, Green BA, Berkowitz BM, et al: The role of intraoperative ultrasonography in the treatment of thoracic and lumbar spine fractures, Spine 9:782, 1984.
- Elattrache N, Fadale PD, Fu F: Thoracic spine fracture in a football player, Am J Sports Med 21:157, 1993.
- Erickson DL, Leider LC Jr, Brown WE: One-stage decompression-stabilization for thoraco-lumbar fractures, Spine 2:53, 1977.
- Esses SI: The placement and treatment of thoracolumbar spine fractures: an algorithmic approach, Orthop Rev 17:571, 1988.
- Esses SI: The AO spinal internal fi xator, Spine 14:373, 1989.
- Esses SI, Botsford DJ, Kostuik JP: Evaluation of surgical treatment for burst fractures, Spine 15:667, 1990.
- Faden AI, Jacobs TP, Patrick DH, et al: Megadose corticosteroid therapy following experimental traumatic spinal injury, J Neurosurg 60:712, 1984.
- Farooq N, Pack JC, Pollintine P, et al: Can vertebroplasty restore normal load-bearing to fractured vertebrae? Spine 30:1723, 2005.
- Ferguson RL, Allen BL Jr: A mechanistic classifi cation of thoracolumbar spine fractures, Clin Orthop Relat Res 189:77, 1984.
- Finkelstein JA, Chapman JR, Mirza S: Anterior cortical allograft in thoracolumbar fractures, J Spinal Disord 12:424, 1999.
- Flesch JR, Leider LL, Erickson D, et al: Harrington instrumentation and spine fusion for unstable fractures and fracture dislocations of the thoracic and lumbar spine, J Bone Joint Surg 59A:143, 1977.
- Folman Y, Gepstein R: Late outcome of nonoperative management of thoracolumbar vertebral wedge fractures, J Orthop Trauma 17:190, 2003.
- Fountain SS, Hamilton RD, Jameson RM: Transverse fractures of the sacrum: a report of six cases, J Bone Joint Surg 59A:486, 1977.
- Francaviglia N, Bragazzi R, Maiello M, et al: Surgical treatment of fractures of the thoracic and lumbar spine via the transpedicular route, Br J Neurosurg 9:511, 1995.
- Fredrickson BE, Yuan HA, Miller H: Burst fractures of the fi fth lumbar vertebra, J Bone Joint Surg 64A:1088, 1982.
- Fribourg D, Tang C, Sra P, et al: Incidence of subsequent vertebral fracture after kyphoplasty, Spine 29:2270, 2004.
- Gaebler C, Maier R, Kukla C, et al: Long-term results of pedicle-stabilized thoracolumbar fractures in relation to the neurological defi cit, Injury 28:661, 1997.
- Gaines RW, Breedlove RF, Munson G: Stabilization of thoracic and thoracolumbar fracture-dislocations with Harrington rods and sublaminar wires, Clin Orthop Relat Res 189:195, 1984.
- Gaines RW, Humphreys WG: A plea for judgment in management of thoracolumbar fractures and fracture-dislocations: a reassessment of surgical indications, Clin Orthop Relat Res 189:36, 1984.
- Garcia F, Florez MT, Conejero JA: A butterfl y vertebra or a wedge fracture? Int Orthop 17:7, 1993.
- Garfi n S: What the experts say: treatment options for VCF, including balloon kyphoplasty. Available at http://kyphon. com. Garfi n SD, Jacobs RR, Stoll J, et al: Results of a locking-hook spinal rod for fractures of the thoracic and lumbar spine, Spine 15:275, 1990.
- Garfi n SR, Mowery CA, Guerra J Jr, et al: Confi rmation of the posterolateral technique to decompress and fuse thoracolumbar spine burst fractures, Spine 10:218, 1985.
- Gertzbein SD: Neurologic deterioration in patients with thoracic and lumbar fractures after admission to the hospital, Spine 19:1723, 1994.
- Gertzbein SD: Spine update: classifi cation of thoracic and lumbar fractures, Spine 19:626, 1994.
- Gertzbein SD, Jacobs RR, Stoll J, et al: Results of a lockinghook spinal rod for fractures of the thoracic and lumbar spine, Spine 15:275, 1990.
- Ghanayem AJ, Zdeblick TA: Anterior instrumentation in the management of thoracolumbar burst fractures, Clin Orthop Relat Res 335:89, 1997.
- Gorczyca JT, Varga E, Woodside T, et al: The strength of iliosacral lag screws and transiliac bars in the fi xation of vertically unstable pelvic injuries with sacral fractures, Injury 27:561, 1996.
- Grasland A, Pouchot J, Mathieu A, et al: Sacral insuffi ciency fractures: an easily overlooked cause of back pain in elderly women, Arch Intern Med 56:668, 1996.
- Greenfi eld RT, Grant RE, Bryant D: Pedicle screw fi xation in the management of unstable thoracolumbar spine injuries, Orthop Rev 21:701, 1992.
- Grob D, Scheier HJG, Dvorak J, et al: Circumferential fusion of the lumbar and lumbosacral spine, Arch Orthop Trauma Surg 111:20, 1991.
- Grootboom MJ, Govender S: Acute injuries of the upper dorsal spine, Injury 24:389, 1993.
- Gurr KR, McAfee PC, Shih C: Biomechanical analysis of posterior instrumentation systems following decompressive laminectomy (an unstable calf spine model), NIH grant, Johns Hopkins University School of Medicine, May 8, 1987.
- Gurwitz GS, Dawson JM, McNamara MJ, et al: Biomechanical analysis of three surgical approaches for lumbar burst fractures using short-segment instrumentation, Spine 18:977, 1993.
- Guttmann L: The treatment and rehabilitation of patients with injuries of the spinal cord. In Cope Z, ed: Medical history of the Second World War: surgery, London, 1953, His Majesty’s Stationery Offi ce. Guttmann L: A new turning-tilting bed, Paraplegia 3:193, 1965.
- Guttmann L: Spinal deformities in traumatic paraplegics and tetraplegics following surgical procedures, Paraplegia 7:38, 1969.
- Ha KI, Han SH, Chung M, et al: A clinical study of the natural remodeling of burst fractures of the lumbar spine, Clin Orthop Relat Res 323:210, 1996.
- Hack HP, Zielke K, Harms J: Spinal instrumentation and monitoring (technique manual), Greensburg, Penn, 1985, Stuart. Hanley EN Jr, Eskay ML: Thoracic spine fractures, Orthopedics 12:689, 1989.
- Hardaker WT, Cook WA, Friedman AH, et al: Bilateral transpedicular decompression and Harrington rod stabilization in the management of severe thoracolumbar burst fractures, Spine 17:162, 1992.
- Harkonen M, Kataja M, Keski-Nisula L, et al: Fractures of the lumbar spine: clinical and radiological results in 94 patients, Orthop Trauma Surg 94:43, 1979.
- Harrington PR: The history and development of Harrington instrumentation (1973 Nicholas Andry Award Contribution), Clin Orthop Relat Res 93:110, 1973.
- Harris MB: The role of anterior stabilization with instrumentation in the treatment of thoracolumbar burst fractures, Orthopedics 15:347, 1992.
- Hartman MB, Chrin AM, Rechtine GR: Nonoperative treatment of thoracolumbar fractures, Paraplegia 33:73, 1995.
- Harvey J, Tanner S: Low back pain in young athletes: a practical approach, Sports Med 12:394, 1991.
- Hatem SF, West OC: Vertical fracture of the central sacral canal: plane and simple, J Trauma 40:138, 1996.
- Heggeness MH, Doherty BJ: The trabecular anatomy of thoracolumbar vertebrae: implications for burst fractures, J Anat 191:309, 1997.
- Heinig CF, Chapman TM, Chewning SJ Jr, et al: Preliminary report on VSP spine fi xation system. Unpublished data, 1988.
- Herring JA, Wenger DR: Segmental spine instrumentation, Spine 7:285, 1982.
- Hitchon PW, Torner JC: Recumbency in thoracolumbar fractures, Neurosurg Clin N Am 8:509, 1997.
- Holdsworth FW, Hardy A: Early treatment of paraplegia from fractures of the thoraco-lumbar spine, J Bone Joint Surg 35B:540, 1953.
- Hu SS, Capen DA, Rimoldi RL, et al: The effect of surgical decompression on neurologic outcome after lumbar fractures, Clin Orthop Relat Res 288:166, 1993.
- Huang TJ, Chen JY, Shih HN, et al: Surgical indications in low lumbar burst fractures: experiences with anterior locking plate system and reduction fi xation system, J Trauma 39:910, 1995.
- Hulme PA, Krebs J, Ferguson SJ, et al: Vertebroplasty and kyphoplasty: a systematic review of 69 clinical studies, Spine 31:1983, 2006.
- Jacobs RR, Asher MA, Snider RK: Thoracolumbar spinal injuries: a comparative study of recumbent and operative treatment in 100 patients, Spine 5:463, 1980.
- Jacobs RR, Casey MP: Surgical management of thoracolumbar spinal injuries (general principles and controversial considerations), Clin Orthop Relat Res 189:22, 1984.
- Jacobs RR, Nordwall A, Nachemson A: Reduction, stability and strength provided by internal fi xation systems for thoracolumbar spinal injuries, Clin Orthop Relat Res 171:300, 1982.
- Jacobs RR, Schlaepfer F, Mathys R Jr, et al: A locking-hook spinal rod system for stabilization of fracture-dislocations and correction of deformities of the dorsolumbar spine: a biomechanical evaluation, Clin Orthop Relat Res 189:168, 1984.
- James KS, Wenger KH, Schlegel JD, et al: Biomechanical evaluation of the stability of thoracolumbar burst fractures, Spine 19:1731, 1994.
- Jane MJ, Freehafer AA, Hazel C, et al: Autonomic dysrefl exia: a cause of morbidity and mortality in orthopedic patients with spinal cord injury, Clin Orthop Relat Res 169:151, 1982.
- Jelsma RK, Kirsch PT, Jelsma LF, et al: Surgical treatment of thoracolumbar fractures, Surg Neurol 3:156, 1982.
- Johnson JR, Leatherman KD, Holt RT: Anterior decompression of the spinal cord for neurologic defi cit, Spine 8:396, 1983.
- Johnson KD, Dadambis A, Seibert GB: Incidence of adult respiratory distress syndrome in patients with multiple musculoskeletal injuries: effect of early operative stabilization of fractures, J Trauma 25:375, 1985.
- Johnson LP, Nasca RJ, Bonnin JM: Pathoanatomy of a burst fracture, Surg Rounds Orthop 2:43, 1988.
- Johnston CE II, Ashman RB, Sherman MC, et al: Mechanical consequences of rod contouring and residual scoliosis in sublaminar segmental instrumentation, J Orthop Res 5:206, 1987.
- Kahanovitz N, Bullough P, Jacobs RR: The effect of internal fi xation without arthrodesis on human facet joint cartilage, Clin Orthop Relat Res 189:204, 1984.
- Kaneda K, Abumi K, Fujiya M: Burst fractures with neurologic defi cits of the thoracolumbar-lumbar spine: results of anterior decompression and stabilization with anterior instrumentation, Spine 9:788, 1984.
- Kaneda K, Gaines RW: Kaneda anterior spinal instrumentation for the thoracolumbar spine, 2nd ed, Cleveland, 1990, Acromed. Kaneda K, Taneichi H, Abumi K, et al: Anterior decompression and stabilization with the Kaneda device for thoracolumbar burst fractures associated with neurological defi cits, J Bone Joint Surg 79A:69, 1997.
- Kaplan SS, Wright NM, Yundt KD, et al: Adjacent fracturedislocations of the lumbosacral spine: case report, Neurosurgery 44:1134, 1999.
- Karjalainen M, Aho AJ, Katevuo K: Operative treatment of unstable thoracolumbar fractures by the posterior approach with the use of Williams plates or Harrington rods, Int Orthop 16:219, 1992.
- Katonis PG, Kontakis GM, Loupasis GA, et al: Treatment of unstable thoracolumbar and lumbar spine injuries using CotrelDubousset instrumentation, Spine 24:2352, 1999.
- Kelly RP, Whitesides TE Jr: Treatment of lumbodorsal fracturedislocations, Ann Surg 167:705, 1968.
- Kennedy JG, Soffe KE, McGrath A, et al: Predictors of outcome in cauda equina syndrome, Eur Spine J 8:317, 1999.
- Kim NH, Lee HM, Chun IM: Neurologic injury and recovery in patients with burst fracture of the thoracolumbar spine, Spine 24:290, 1999.
- King AG: Burst compression fractures of the thoracolumbar spine: pathologic anatomy and surgical management, Orthopedics 10:1711, 1987.
- Kirkpatrick JS, Wilber RG, Likavec M, et al: Anterior stabilization of thoracolumbar burst fractures using the Kaneda device: a preliminary report, Orthopedics 18:673, 1995.
- Korovessis PG, Baikousis A, Stamatakis M: Use of the Texas Scottish Rite Hospital instrumentation in the treatment of thoracolumbar injuries, Spine 22:882, 1997.
- Korovessis P, Sidiropoulos P, Dimas A: Complete fracturedislocation of the thoracic spine without neurologic defi cit: case report, J Trauma 36:122, 1994.
- Kostuik JP: Anterior spinal cord decompression for lesions of the thoracic and lumbar spine: techniques: new methods of internal fi xation, results, Spine 8:512, 1983.
- Kraemer WJ, Schemitsch EH, Lever J, et al: Functional outcome of thoracolumbar burst fractures without neurological defi cit, J Orthop Trauma 10:541, 1996.
- Krag MH, Weaver DL, Beynnon BD, et al: Morphometry of the thoracic and lumbar spine related to transpedicular screw placement for surgical spinal fi xation, Spine 13:27, 1988.
- Kramer DL, Rodgers WB, Mansfi eld FL: Transpedicular instrumentation and short-segment fusion of thoracolumbar fractures: a prospective study using a single instrumentation system, J Orthop Trauma 9:499, 1995.
- Krompinger WJ, Frederickson BE, Mino DE, et al: Conservative treatment of fractures of the thoracic and lumbar spine, Orthop Clin North Am 17:161, 1986.
- Krueger MA, Green DA, Hoyt D, et al: Overlooked spine injuries associated with lumbar transverse process fractures, Clin Orthop Relat Res 327:191, 1996.
- Kulkarni MB, McArdle CB, Kopaniky D, et al: Acute spinal cord injury: MR imaging at 115 T1, Neuroradiology 164:837, 1987.
- Kupferschmid JP, Weaver ML, Raves JJ, et al: Thoracic spine injuries in victims of motorcycle accidents, J Trauma 29:593, 1989.
- Laborde JM, Bahniuk E, Bohlman HH, et al: Comparison of fi xation of spinal fractures, Clin Orthop Relat Res 152:305, 1980.
- Lafollete BF, Levine MI, McNiesh LM: Bilateral fracturedislocation of the sacrum, J Bone Joint Surg 68A:1099, 1986.
- Lee HM, Kim HS, Kim DJ, et al: Reliability of magnetic resonance imaging in detecting posterior ligament complex injury in thoracolumbar spinal fractures, Spine 25:2079, 2000.
- Levine AM, Bosse M, Edwards CC: Bilateral facet dislocations in the thoracolumbar spine, Spine 13:630, 1988.
- Levine AM, Edwards CC: Low lumbar burst fractures: reduction and stabilization using the modular spine fi xation system, Orthopedics 1:9, 1988.
- Limb D, Shaw DL, Dickson RA: Neurological injury in thoracolumbar burst fractures, J Bone Joint Surg 77B:774, 1995.
- Lindahl S, Willen J, Nordwall A, et al: The crush-cleavage fracture: a “new” thoracolumbar unstable fracture, Spine 8:559, 1983.
- Lindsey RW, Dick W: The fi xateur interne in the reduction and stabilization of thoracolumbar spine fractures in patients with neurologic defi cit, Spine 16(suppl):140, 1991.
- Lindsey RW, Dick W, Nunchuck S, et al: Residual intersegmental spinal mobility following limited pedicle fi xation of thoracolumbar spine fractures with the fi xateur interne, Spine 18:474, 1993.
- Louis R: Fusion of the lumbar and sacral spine by internal fi xation with screw plates, Clin Orthop Relat Res 203:18, 1986.
- Luque ER, Cassis N, Ramirez-Wiella G: Segmental spinal instrumentation in the treatment of fractures of the thoracolumbar spine, Spine 7:312, 1982.
- Macmillan M, Stauffer ES: Transient neurologic defi cits associated with thoracic and lumbar spine trauma without fracture or dislocation, Spine 15:466, 1990.
- Magerl FP: Stabilization of the lower thoracic and lumbar spine with external skeletal fi xation, Clin Orthop Relat Res 189:125, 1984.
- Maiman DJ, Pintar F, Yoganandan N, et al: Effects of anterior vertebral grafting on the traumatized lumbar spine after pedicle screw-plate fi xation, Spine 18:2423, 1993.
- Mann KA, McGowan DP, Fredrickson BE, et al: A biomechanical investigation of short segment spinal fi xation for burst fractures with varying degrees of posterior disruption, Spine 15:407, 1990.
- Markel DC, Graziano GP: A comparison study of treatment of thoracolumbar fractures using the ACE Posterior Segmental Fixator and Cotrel-Dubousset instrumentation, Orthopedics 18:679, 1995.
- McAfee PC: Biomechanical approach to instrumentation of the thoracolumbar spine: a review article, Adv Orthop Surg 8:313, 1985.
- McAfee PC, Bohlman HH: Anterior decompression of traumatic thoracolumbar fractures with incomplete paralysis through the retroperitoneal approach, Orthop Trans 8:392, 1984.
- McAfee PC, Bohlman HH: Complications following Harrington instrumentation for fractures of the thoracolumbar spine, J Bone Joint Surg 67A:672, 1985.
- McAfee PC, Bohlman HH, Yuan HA: Anterior decompression of traumatic thoracolumbar fractures with incomplete neurological defi cit using a retroperitoneal approach, J Bone Joint Surg 67A:89, 1985.
- McAfee PC, Levine AM, Anderson PA: Surgical management of thoracolumbar fractures, Instr Course Lect 44:47, 1995.
- McAfee PC, Werner FW, Glisson RR: A biomechanical analysis of spinal instrumentation systems in thoracolumbar fractures: comparison of traditional Harrington side traction instrumentation with segmental spinal instrumentation, Spine 10:204, 1985.
- McAfee PC, Yuan HA, Fredrickson BE, et al: The value of computed tomography in thoracolumbar fractures, J Bone Joint Surg 64A:461, 1983.
- McAfee PC, Yuan HA, Lasda NA: The unstable burst fracture, Spine 7:365, 1982.
- McBride GG: Surgical stabilization of thoracolumbar fractures using Cotrel-Dubousset rods, Semin Spine Surg 2:24, 1990.
- McCrory BJ, VanderWilde RS, Currier BL: Diagnosis of subtle thoracolumbar burst fractures: a new radiographic sign, Spine 18:2282, 1993.
- McDonough PW, Davis R, Tribus C, et al: The management of acute thoracolumbar burst fractures with anterior corpectomy and Z-plate fi xation, Spine 29:1901, 2004.
- McFarland EG, Giangarra C: Sacral stress fractures in athletes, Clin Orthop Relat Res 329:240, 1996.
- McGuire RA Jr: The role of anterior surgery in the treatment of thoracolumbar fractures, Orthopedics 20:959, 1997.
- McGuire RA, Freeland AE: Flexion-distraction injury of the thoracolumbar spine, Orthopedics 15:379, 1992.
- Mehta JS, Reed MR, McVie JL, et al: Weight-bearing radiographs in thoracolumbar fractures: do they infl uence management? Spine 29:564, 2004.
- Meldon SW, Moettus LN: Thoracolumbar spine fractures: clinical presentation and the effect of altered sensorium and major injury, J Trauma 39:1110, 1995.
- Mermelstein LE, McLain RF, Yerby SA: Reinforcement of the thoracolumbar burst fractures with calcium phosphate cement: a biomechanical study, Spine 23:664, 1998.
- Meves R, Avanzi O: Correlation between neurological defi cit and spinal canal compromise in 198 patients with thoracolumbar and lumbar fractures, Spine 30:787, 2005.
- Meves R, Avanzi O: Correlation among canal compromise, neurologic defi cit, and injury severity in thoracolumbar burst fractures, Spine 31:2137, 2006.
- Meyer PR: Complications of treatment of fractures and dislocations of the dorsolumbar spine. In Epps CH, ed: Complications in orthopaedic surgery, Philadelphia, 1978, Lippincott. Miyakoshi N, Abe E, Shimada Y, et al: Anterior decompression with single segmental spinal interbody fusion for lumbar burst fracture, Spine 24:67, 1999.
- Moorman CT, Richardson WJ, Fitch RD, et al: Flexiondistraction injuries to the lumbar spine in children, J South Orthop Assoc 1:296, 1992.
- Morgan FH, Wharton W, Austin GN: The results of laminectomy in patients with incomplete spinal cord injuries, Paraplegia 9:14, 1971.
- Mozes GC, Kollender Y, Sasson AA: Transpedicular screw-rod fi xation in the treatment of unstable lower thoracic and lumbar fractures, Bull Hosp Jt Dis 53:37, 1993.
- Mumford J, Weinstein JN, Spratt KF, et al: Thoracolumbar burst fractures: the clinical effi cacy and outcome of nonoperative management, Spine 18:955, 1993.
- Munro AHG, Irwin CG: Interlocked articular processes complicating fracture-dislocation of the spine, Br J Surg 25:621, 1938.
- Myllynen P, Bostman O, Riska E: Recurrence of deformity after removal of Harrington’s fi xation of spine fractures (seventy-six cases followed for 2 years), Acta Orthop Scand 59:497, 1988.
- Nagai H, Shimizu K, Shikata J: Chylous leakage after circumferential thoracolumbar fusion for correction of kyphosis resulting from fracture: report of three cases, Spine 22:2766, 1997.
- Nagel DA, Koogle TA, Piziali RL, et al: Stability of the upper lumbar spine following progressive disruptions in the application of individual internal and external fi xation devices, J Bone Joint Surg 63A:62, 1981.
- Nicoll EA: Fractures of the dorso-lumbar spine, J Bone Joint Surg 31B:376, 1949.
- Nork SE, Jones CD, Harding SP, et al: Percutaneous stabilization of U-shaped sacral fractures using iliosacral screws: technique and early results, J Orthop Trauma 15:238, 2001.
- Oda T, Panjabi MM: Pedicle screw adjustments affect stability of thoracolumbar burst fracture, Spine 26:2328, 2001.
- Oda T, Panjabi MM, Kato Y: The effects of pedicle screw adjustments on the anatomical reduction of thoracolumliar burst fractures, Eur Spine J 10:505, 2001.
- Okuyama K, Abe E, Chiba M, et al: Outcome of anterior decompression and stabilization for thoracolumbar unstable burst fractures in the absence of neurologic defi cits, Spine 21:620, 1996.
- Olerud C, Sjöström L, Jónsson H, et al: Posterior reduction of a pathologic spinal fracture: a case of indirect anterior dual decompression, Acta Orthop Scand 63:345, 1992.
- Oner FC, van-Gils AP, Dhert WJ, et al: MRI fi ndings of thoracolumbar spine fractures: a categorisation based on MRI examinations of 100 fractures, Skeletal Radiol 28:433, 1999.
- Oner FC, van-der-Rijt RR, Ramos LM, et al: Changes in the disc space after fractures of the thoracolumbar spine, J Bone Joint Surg 80B:833, 1998.
- Osebold WR, Weinstein SL, Sprague BL: Thoracolumbar spine fractures: results of treatment, Spine 6:13, 1981.
- Osti OL, Fraser RD, Cornish BL: Fractures and fractures-dislocations of the lumbar spine: a retrospective study of 70 patients, Int Orthop 11:323, 1987.
- Ozturk C, Ersozlu S, Aydinli U: Importance of greenstick lamina fractures in low lumbar burst fractures, Int Orthop 30:295, 2006.
- Panjabi MM, Kifune M, Wen L, et al: Dynamic canal encroachment during thoracolumbar burst fractures, J Spinal Disord 8:39, 1995.
- Panjabi MM, Oxland TR, Kifune M, et al: Validity of the threecolumn theory of thoracolumbar fractures: a biomechanic investigation, Spine 20:1122, 1995.
- Panjabi MM, Oxland TR, Lin RM, et al: Thoracolumbar burst fracture: a biomechanical investigation of its multidirectional fl exibility, Spine 19:578, 1994.
- Parfenchuck TA, Chambers J, Goodrich JA, et al:
You Might Also Like


