Mastering Skin Coverage in the Hand: Grafts, Flaps, and Scar Reconstruction
Key Takeaway
Effective skin coverage in the hand is paramount for preserving joint mobility, tendon glide, and tactile sensation. This comprehensive guide details the surgical management of granulating wounds and restrictive scars. It explores the biomechanics of dorsal and palmar skin, indications for split-thickness and full-thickness grafts, and advanced flap reconstruction techniques. Mastery of these principles ensures optimal functional and aesthetic outcomes in complex hand trauma and reconstructive surgery.
Introduction to Skin Coverage in the Hand
The soft tissue envelope of the hand is a highly specialized, dynamic structure that must accommodate extreme ranges of motion while providing durable, sensate coverage for underlying neurovascular bundles, tendons, and osteoarticular frameworks. Loss of this envelope, whether through acute trauma, infection, or surgical extirpation, demands immediate and meticulous reconstruction.
Failure to achieve stable, pliable skin coverage rapidly leads to desiccation of deep structures, infection, and the formation of restrictive scar tissue. In the hand, form and function are inextricably linked; therefore, the reconstructive surgeon must possess a profound understanding of tissue biomechanics, graft physiology, and the precise indications for various coverage modalities, ranging from simple skin grafts to complex vascularized free tissue transfers.
Management of Granulating Areas
A granulating wound on the hand should rarely, if ever, be permitted to heal by secondary intention. Healing by secondary intention relies heavily on myofibroblast-mediated wound contraction, which inevitably results in a dense, inelastic scar that severely compromises hand mechanics.
If the hand has not been completely covered with skin during the initial treatment of an acute injury, a split-thickness skin graft (STSG) should be applied as soon as the wound bed is adequately prepared. The surface must be clean, highly vascularized, and free of necrotic debris or critical bacterial colonization to support graft survival through the phases of plasmatic imbibition and inosculation.
Surgical Warning: Even if the entire granulating surface is not uniformly clean, any portion that is viable and clean enough should be grafted immediately to halt the progression of contracture.
However, skin grafts require a vascularized bed. Exposed avascular structures—specifically tendons devoid of paratenon, joints devoid of capsule, or cortical bone devoid of periosteum—cannot support a free skin graft. These critical structures mandate immediate coverage with vascularized tissue, such as local, regional, or distant flap grafts, to prevent desiccation and necrosis.
Pathophysiology and Biomechanics of Hand Scars
A scar is a fundamentally poor substitute for native skin. It is composed of disorganized, densely packed collagen bundles that lack the elastin fibers necessary for normal tissue compliance. Furthermore, scar tissue lacks normal sensory end-organs, rendering it insensate or dysesthetic.
The absence of elasticity in a scar restricts the motion of otherwise unobstructed underlying joints and interferes with the microvascular nutrition of adjacent tissues. Frequently, the scar adheres to deep structures, including joint capsules, extensor paratenon, and flexor tendon sheaths, creating a tethering effect that further limits excursion and motion.
The Fallacy of Passive Stretching
A scar actively contracts during the proliferative and remodeling phases of healing and does not spontaneously stretch later. Attempts to stretch a scar therapeutically are often misunderstood; any perceived benefit is usually due to the stretching of the normal, compliant skin surrounding the scar, rather than the scar itself.
When a linear scar spans a joint, the intermittent tension caused by active motion stimulates mechanotransduction pathways, leading to continuous collagen deposition and subsequent scar hypertrophy.
Clinical Pearl: Forced passive stretching of a mature scar is contraindicated. It causes the inelastic scar tissue to rupture and fissure at a microscopic level. This microtrauma incites a renewed inflammatory response, causing the scar to heal even thicker and more unyielding than before.
Beyond mechanical restriction, scars can become profoundly painful if they adhere to or entrap regenerating nerve endings, leading to the formation of symptomatic neuromas.
Indications and Timing for Surgical Revision of Scars
While scars cannot be entirely eliminated—since the very act of surgical revision relies on the production of new scar tissue—they can be partially replaced by tissue of superior quality. Furthermore, the vector, direction, or location of the scar lines can be surgically altered to minimize interference with biomechanical function.
Surgical intervention for hand scars is indicated for the following primary reasons:
1. To eliminate structural deformity.
2. To restore joint motion and tendon excursion.
3. To provide durable skin coverage for vulnerable parts or to permit subsequent operations on deeper structures (e.g., tenolysis, nerve grafting).
4. To relieve pain associated with tethering or neuroma entrapment.
5. To improve the aesthetic appearance of the hand (occasionally).
Timing of Intervention
As a general rule, a scar should not be surgically revised until it has fully matured. Scar maturation is characterized by a decrease in erythema, softening of the tissue, and flattening of the scar profile, which typically requires a minimum of 3 to 6 months. Operating on an immature, hyperemic scar often leads to excessive bleeding, poor tissue handling, and a high recurrence rate of hypertrophy.
The Exception to the Rule:
Scars must be treated earlier, regardless of maturation, when they cause severe, progressive joint contractures. For example, when a metacarpophalangeal (MCP) joint is held in rigid extension, or a proximal interphalangeal (PIP) joint is held in rigid flexion, severe secondary contractures of the collateral ligaments and volar plates develop rapidly. In these instances, the offending scar must be released or excised as soon as possible to prevent irreversible joint stiffness.
For the purposes of surgical planning, scars are classified morphologically as linear scars or area scars. Either type may be located on the volar or dorsal surface and may or may not involve deep structural adhesions.
Surgical Techniques for Correcting Linear Scars
Disabling linear scars typically result from poorly planned surgical incisions or traumatic lacerations that cross the transverse flexion creases of the digits, palm, or wrist at a perpendicular angle.
Dorsal vs. Volar Linear Scars
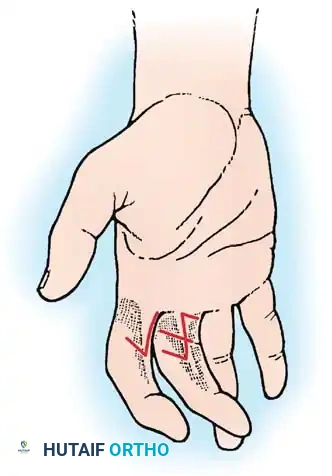
When a narrow linear scar on a finger is surrounded by mobile, normal tissue, it can often be released and redirected using a Z-plasty. The Z-plasty transposes triangular flaps to change the direction of the scar (ideally placing the central limb parallel to the skin creases) and elongates the contracted tissue at the expense of adjacent transverse width.
Fig. 62-36A: Severe flexion contractures caused by linear scars crossing the volar flexion creases of the digits.

Fig. 62-36B: The contractures have been successfully released and redirected utilizing multiple Z-plasties.
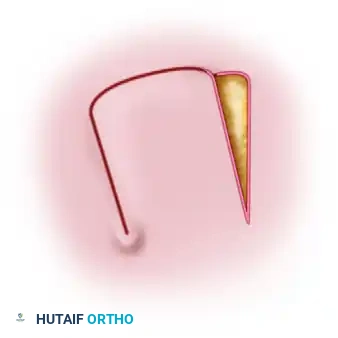
However, the biomechanics of the volar and dorsal skin differ significantly. On the dorsum of the hand, the skin is highly mobile and loosely attached to the underlying extensor paratenon, making most disabling dorsal linear scars highly amenable to correction by Z-plasty.
Conversely, the volar skin is firmly tethered to the underlying palmar fascia and flexor tendon sheaths by Cleland's and Grayson's ligaments to provide a stable surface for gripping. Because of this lack of mobility, a volar linear scar that is more than 2 mm wide is exceedingly difficult to correct with a simple Z-plasty. The adjacent skin cannot be mobilized sufficiently without excessive tension.
In these instances, the contracted linear scar must be completely excised and replaced by:
* A full-thickness skin graft (FTSG).
* A cross-finger flap.
* A local advancement or transposition flap.
On the palm, a linear scar often represents a true loss of skin substance rather than simple contraction. Correcting a palmar scar contracture by Z-plasty is notoriously difficult and often fails. In this region, complete excision of the scar followed by a free split-thickness or full-thickness graft is the indicated approach.
Surgical Management of Area Scars
An area scar represents a significant initial loss of skin. Because the wound has contracted during the healing process, the visible area of the final scar is always smaller than the original tissue defect.
Surgical Principle: When an area scar is excised, the surrounding normal skin will immediately retract to its native anatomical position. Therefore, the resulting surgical defect will be substantially larger than the scar that was removed. The replacement graft or flap must always be planned and harvested to be larger than the visible scar.
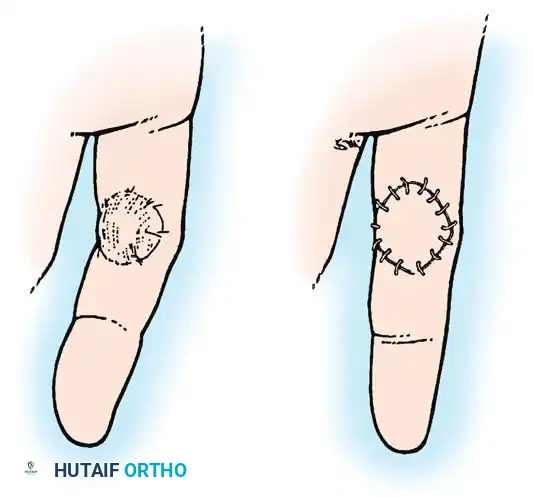
Fig. 62-37: An area scar (A) has been completely excised and replaced by a full-thickness skin graft (B) that is significantly larger than the original scar footprint, accommodating the true tissue defect.
Flap Selection for Area Scars
The fundamental principle of reconstructive surgery is to replace "like with like." Therefore, skin used for any graft should be as similar to the lost skin as possible in terms of thickness, pigmentation, hair bearing qualities, and sensibility.
- Small Area Losses: A local flap or a cross-finger flap is preferable, as it brings vascularized tissue of similar quality into the defect.
- Large Area Losses or Deep Defects: If the area is extensive, or if excision of the scar exposes bare bone, joint capsule, or tendon devoid of paratenon, a free skin graft will fail. In these scenarios, a distant ("remote") pedicled flap (e.g., groin flap) or a vascularized free tissue transfer (e.g., anterolateral thigh flap, lateral arm flap) containing skin and subcutaneous fat is mandatory.
When applying a flap over a previously scarred bed, deeper parts of the scar tissue may be excised to create a healthy recipient bed. However, reconstructive procedures on deep structures, such as tendon grafting or nerve repair, should generally be staged and performed later.
Surgical Warning: When secondary deep procedures are performed beneath a previously placed flap, the tendons or nerves must be exposed through an incision placed carefully along the edge of the flap, never directly through the center of the flap, to avoid compromising its vascular supply.
Dorsal Area Scars and Skin Excursion
An area scar on the dorsum of the hand that involves only the superficial skin layers may be replaced by a medium or thick split-thickness skin graft. Careful preoperative planning regarding the size of the graft is critical due to the unique biomechanics of dorsal hand skin.
The normal adult hand possesses significant skin redundancy on the dorsum to accommodate motion:
* Longitudinal Redundancy: Approximately 5 cm of extra skin is required longitudinally to allow for simultaneous full flexion of the wrist and the digits.
* Transverse Redundancy: Approximately 2.5 cm of extra skin is required transversely to allow for the development of the metacarpal arch when making a tight fist.
A graft placed on the dorsum must account for this required extra skin, the immediate expansion of the defect upon scar excision, and the inevitable secondary contraction of the graft itself during healing.
Crucially, the graft must be placed and immobilized while the hand is held in the position of maximum skin tension; otherwise, the healed graft will be too tight, restricting flexion. Burm et al. demonstrated that the greatest amount of skin can be grafted to the dorsum of the hand when it is immobilized in the "fist" position, noting that the anatomical position actually allows for more skin surface area than the traditional "safe" position.

Fig. 62-38A: Anatomical positioning.

Fig. 62-38B: The "Safe" position (intrinsic plus).

Fig. 62-38C: The Fist position, which maximizes the dorsal surface area for grafting.
However, the surgeon must balance the need for maximal dorsal skin coverage with the risk of joint stiffness. In most clinical situations, holding the fingers in full flexion (the fist position) for prolonged periods risks the development of severe proximal interphalangeal (PIP) joint flexion contractures. Therefore, careful monitoring and timely initiation of rehabilitation are essential.
Palmar Area Scars and Specialized Glabrous Skin
Reconstructing an area scar on the palm presents a unique challenge because palmar skin is highly specialized. It is glabrous (hairless), highly innervated, tethered to the underlying fascia to prevent shearing, and uniquely designed to withstand immense friction and shock. Similar skin is found anatomically only on the sole of the foot.
- Superficial Palmar Scars: If the scar is superficial and the underlying fat pads and fascia are intact, a thick split-thickness skin graft can be utilized.
- Deep Palmar Scars: If deep, vulnerable structures are involved, a full-thickness skin graft (FTSG) is preferable. FTSGs provide better durability and contract less than STSGs. However, they are more technically demanding to handle, have higher metabolic requirements (making them slightly less likely to survive if the bed is suboptimal), and are limited in size because the donor site must be closed primarily.
Restoring Sensibility in Critical Areas:
For an insensitive, large area scar located on the critical contact surfaces of the hand—specifically the radial side of an otherwise normal index finger or the volar pinch area of the thumb—simple skin grafting is insufficient because it does not restore protective or tactile sensation. In these highly specific indications, a neurovascular island pedicle flap (e.g., transferring sensate skin from the ulnar aspect of the ring finger) is indicated to restore critical pinch biomechanics and proprioception.
When any graft is applied to the hand, the fundamental rules guiding the location and direction of hand incisions must be meticulously followed. The margins of the graft will heal to the normal surrounding skin with a linear scar. If these marginal scars cross flexion creases perpendicularly, they will inevitably lead to secondary linear contractures.
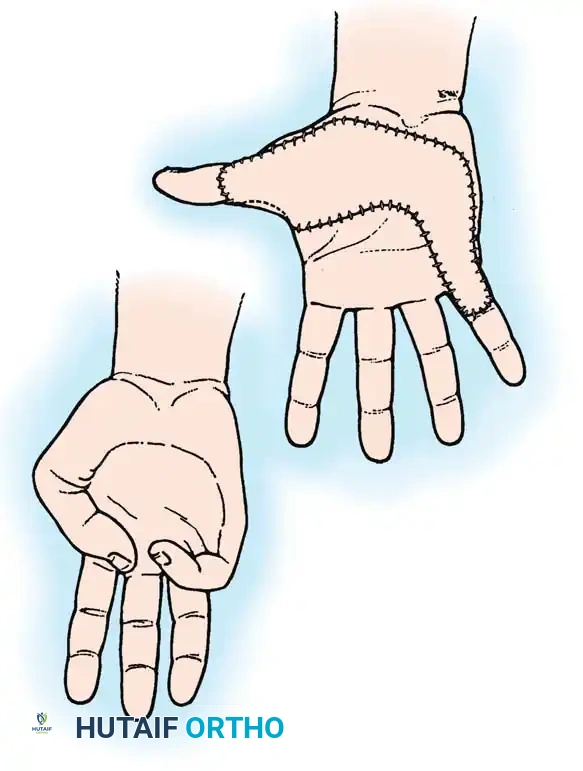
Fig. 62-39: An area scar on the palm (A) has been excised and replaced by a graft (B). Note that the margins of the graft have been meticulously designed to follow the rules that guide the location and direction of hand incisions, utilizing darting and zig-zag patterns to prevent secondary linear contractures.
Postoperative Protocols and Rehabilitation
The success of skin coverage in the hand relies as much on postoperative management as it does on surgical execution.
- Immobilization: Skin grafts must be immobilized to prevent shearing forces that disrupt the fragile ingrowth of capillaries (inosculation) during the first 3 to 5 days. Tie-over bolster dressings are highly recommended to maintain uniform pressure and prevent hematoma or seroma accumulation beneath the graft.
- Splinting: The hand should be splinted in a position that maintains the graft at its maximum functional length without placing excessive tension on the marginal sutures.
- Rehabilitation: Once graft take is confirmed (typically at 7 to 10 days), gentle active range of motion (AROM) is initiated. Passive range of motion (PROM) is delayed until the graft is fully stable to prevent tearing.
- Scar Management: As the graft and marginal scars mature, aggressive scar management is instituted. This includes the use of custom-molded silicone gel sheeting, compressive garments (e.g., Isotoner gloves), and deep friction massage to align collagen fibers and prevent adherence to underlying tendons.
By adhering to these strict biomechanical and physiological principles, the orthopaedic surgeon can successfully navigate the complexities of hand skin coverage, restoring both the structural integrity and the intricate function of the hand.
You Might Also Like