Interdigital (Morton's) Neuroma: Comprehensive Surgical Management
Key Takeaway
Interdigital neuroma, commonly known as Morton's neuroma, presents as forefoot pain radiating into the toes, predominantly in the third web space. Diagnosis is primarily clinical, highlighted by web space tenderness and a positive Mulder's click. While nonoperative measures like orthotics and corticosteroid injections are first-line treatments, surgical excision remains the definitive management for refractory cases. Successful neurectomy requires proximal transection to prevent stump neuroma formation and tethering by plantar nerve branches.
INTRODUCTION AND PATHOANATOMY
Interdigital neuroma, frequently referred to as Morton’s neuroma, is a common cause of metatarsalgia characterized by perineural fibrosis and nerve degeneration of the common digital nerve. Despite the nomenclature, it is not a true neoplastic neuroma but rather a reactive, compressive neuropathy. The condition predominantly affects the third web space, followed by the second web space, and is exceedingly rare in the first and fourth interspaces.
The unique predilection for the third web space is multifactorial. Anatomically, the third common digital nerve often receives anastomotic branches from both the medial and lateral plantar nerves, increasing its cross-sectional diameter and rendering it more susceptible to compression beneath the deep transverse intermetatarsal ligament (DTML). Furthermore, the third web space represents the biomechanical interface between the relatively mobile lateral column (fourth and fifth metatarsals) and the more rigid medial column (first, second, and third metatarsals), subjecting the nerve to increased shearing forces during the terminal stance phase of gait.
CLINICAL PRESENTATION: SIGNS AND SYMPTOMS
The primary and most debilitating symptom of an interdigital neuroma is pain, typically localized to the region of the metatarsal heads—most frequently the third and fourth. Patients classically describe the pain as burning, aching, or cramping, often accompanied by the sensation of "walking on a marble" or a "pebble in the shoe."
The onset of symptoms may be insidious or initiated by a specific traumatic event to the forefoot. The duration of pain is highly variable, ranging from a few weeks to several years. Symptoms are characteristically exacerbated by weight-bearing activities, walking, and the use of narrow, tight-fitting, or high-heeled footwear. Conversely, pain is reliably relieved by rest, removing the offending shoe, and massaging the forefoot.
Women are disproportionately affected compared to men, with an incidence ratio of approximately 8:1, largely attributed to footwear biomechanics (narrow toe boxes and elevated heels that hyperextend the metatarsophalangeal joints and tether the nerve against the DTML). The condition is usually unilateral.
Physical Examination
A meticulous physical examination is paramount, as the diagnosis of interdigital neuroma remains primarily clinical.
- Web Space Tenderness: The most frequent and reliable finding is exquisite tenderness localized to the affected web space, just distal to the transverse intermetatarsal ligament.
- Mulder's Click: Described by Mulder, this is a palpable and often audible click elicited by manually squeezing the metatarsal heads together while simultaneously applying dorsal pressure to the plantar aspect of the web space. This maneuver displaces the enlarged neuroma-bursal complex dorsally across the DTML.
- Clinical Nuance: While helpful when present, a positive Mulder's click can frequently be elicited in the opposite, asymptomatic foot. Therefore, the presence of the click must correlate with the patient's exact pain reproduction to be considered diagnostic.
- Examination Technique: The click is best appreciated with the patient lying prone. The examiner places their thumb dorsally and their index finger plantarward over the appropriate web space, gently rocking the hand back and forth.
- Sullivan's Sign: If an enlarged intermetatarsal bursa is present, or if the neuroma is exceptionally thick, a visible splaying or spreading of the adjacent toes at the affected web space may be observed when the patient stands.
- Sensory Deficits: Subjective numbness radiating into the adjacent halves of the toes of the involved interspace is a common complaint; however, objective signs of decreased sensibility (e.g., altered two-point discrimination or Semmes-Weinstein monofilament testing) are less frequently encountered.
CLINICAL PEARL: Differentiating Neuroma from Plantar Plate Tears
Palpating the web spaces with the patient standing is highly effective in differentiating a second web space neuroma from a plantar plate lesion or capsulitis at the second metatarsophalangeal (MTP) joint. If the tenderness is strictly localized to the soft tissue of the web space and not to the plantar aspect of the proximal phalanx base or the dorsolateral MTP joint capsule, a neuroma is highly likely. Furthermore, when the patient stands, tenderness in the third web space often becomes more pronounced, solidifying the diagnosis of a third web space neuroma over a traumatic inflammatory injury of the adjacent MTP joints.
Diagnostic Imaging
While the diagnosis is clinical, imaging modalities are utilized primarily to rule out competing pathologies such as stress fractures, Freiberg's infraction, or MTP joint arthritis.
* Radiographs: Weight-bearing anteroposterior, lateral, and oblique views of the foot should be routinely obtained. In isolated neuroma cases, these are typically normal but may show lateral toe splaying.
* Ultrasonography and MRI: Although frequently recommended, both modalities have been shown to be of limited value in altering the clinical management of a classic presentation. Pathological findings (e.g., enlarged nerves or bursitis) are occasionally found in asymptomatic interdigital nerves. The use of sensory action potentials (EMG/NCS) to objectively confirm the diagnosis has yielded highly variable results and is not routinely recommended.
NONOPERATIVE MANAGEMENT
A trial of conservative management is mandatory before considering surgical intervention. While results can be unpredictable, they are successful often enough to warrant a dedicated trial period.
- Footwear Modification: The cornerstone of nonoperative treatment is transitioning to shoes with a wide toe box and a low heel to reduce mechanical compression and MTP joint hyperextension.
- Orthotics: Metatarsal pads or bars placed proximal to the metatarsal heads can help splay the metatarsals and elevate the transverse arch, thereby decompressing the intermetatarsal space.
- Corticosteroid Injections: A local injection of a corticosteroid and local anesthetic preparation into the affected web space (typically via a dorsal approach to avoid plantar fat pad atrophy) can provide significant diagnostic information and therapeutic relief.
SURGICAL INDICATIONS AND PATIENT COUNSELING
The mainstay of treatment for refractory interdigital neuroma is surgical excision. Numerous reports have confirmed the efficacy of neuroma excision, particularly in the third web space. In most historical series, 80% to 95% of patients report being completely asymptomatic and highly satisfied with the surgical outcome.
However, modern outcomes literature necessitates cautious patient counseling.
SURGICAL WARNING: Managing Patient Expectations
Excision of an interdigital neuroma is a worthwhile procedure, but the essential criterion for a successful result is the relief of severe pain, not necessarily the restoration of a completely normal foot.A sobering report by Mann and Reynolds demonstrated that postoperatively:
* 65% of patients still noted some local plantar tenderness.
* 68% noted permanent numbness in the involved interspace.
* 20% subjectively rated their result as less than a 50% improvement in symptoms.Furthermore, Womack et al. found that long-term outcomes of neuroma excision were not as universally successful as previously reported, with up to 70% of patients experiencing some ongoing limitation in footwear.
Detailed preoperative examination and careful patient selection are paramount. The surgeon must look carefully for other causes of metatarsalgia (e.g., MTP instability, tarsal tunnel syndrome, peripheral neuropathy) that might coexist. The patient must be explicitly informed that any symptoms other than those directly caused by the neuroma will not be improved by its excision, and that permanent numbness in the web space is an expected outcome of neurectomy.
If symptoms occur following midfoot or forefoot trauma, surgical excision should be considered with extreme caution. It may require several months for tissue homeostasis to return and for post-traumatic inflammatory symptoms to resolve independently.
SURGICAL APPROACHES AND TECHNIQUES
Opinions vary regarding the optimal surgical approach (dorsal vs. plantar) and the specific procedure (neurectomy vs. neurolysis).
Epineural Neurolysis (Gauthier's Technique)
Gauthier proposed epineural neurolysis using a longitudinal dorsal approach, wherein the deep transverse intermetatarsal ligament is released to facilitate decompression, leaving the nerve intact. While this avoids the numbness associated with neurectomy, studies have shown that up to 28% of patients remain unimproved or have enough continued symptoms to warrant further ablative treatment. Division of the DTML without neurectomy remains controversial, as its isolated division may theoretically result in a "dropped" metatarsal or splaying of the forefoot, though clinical evidence of this is debated.
Primary Neurectomy: Dorsal vs. Plantar Approach
The choice between a dorsal or plantar incision is largely determined by the surgeon’s training and the specific clinical scenario.
- Dorsal Approach: Generally preferred for primary excisions. It allows for early weight-bearing and avoids a potentially painful plantar scar. However, identifying the proximal nerve stump can be challenging if the DTML is not divided.
- Plantar Approach: Provides direct, excellent exposure of the neuroma and the proximal nerve anatomy. It is highly recommended for recurrent neuromas. The primary disadvantage is that patients frequently complain of soreness around the plantar wound for many weeks, which can delay return to normal activities.
Studies comparing dorsal and plantar longitudinal approaches for primary excision have shown no significant difference in overall patient satisfaction, sensory loss, or sick leave duration. However, the dorsal group historically showed higher rates of missed nerves (due to inadequate proximal visualization) and stump neuromas, whereas the plantar group experienced minor intraincisional keratoses.
Surgical Technique: Dorsal Approach for Primary Excision
1. Positioning and Preparation:
The patient is placed supine on the operating table. A calf or thigh tourniquet is applied. The foot is prepped and draped in a standard sterile fashion.
2. Incision and Dissection:
A 3 to 4 cm longitudinal incision is made over the dorsal aspect of the affected web space, starting at the web commissure and extending proximally between the metatarsal heads. Care is taken to identify and retract any dorsal sensory cutaneous nerve branches.
3. Exposure of the Neuroma:
Blunt dissection is carried down through the subcutaneous tissue to the deep transverse intermetatarsal ligament. A lamina spreader is inserted between the metatarsal heads to splay the interspace and place the DTML under tension.
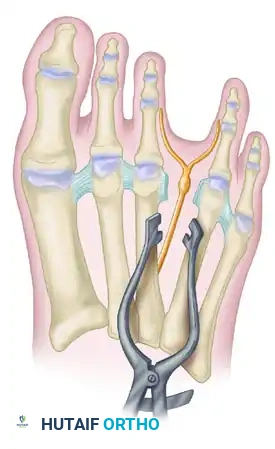
FIGURE 86-9 A: Lamina spreader used to expose the neuroma within the intermetatarsal space.
4. Ligament Release and Nerve Isolation:
The DTML is identified. Through the dorsal approach, the nerve is significantly better exposed in its proximal portion if the ligament is divided. The ligament is carefully transected longitudinally. Once released, digital pressure applied to the plantar aspect of the web space will push the neuroma dorsally into the surgical field.
5. Distal Transection:
The common digital nerve is traced distally to its bifurcation into the proper digital nerves. The proper digital branches are transected distal to the neuroma.
6. Proximal Transection (The Critical Step):
The nerve is then reflected proximally. It is imperative to transect the nerve as far proximally as the incision allows.
PITFALL: Inadequate Proximal Resection
Several plantarly directed nerve branches run from the common digital nerve into the forefoot pad. They are found in the highest concentration in the distal aspect of the common digital nerve, just proximal to its bifurcation. If the nerve is not transected well proximal to the DTML, these plantarly directed nerve fibers will tether the retracting common digital nerve. This prevents the nerve stump from retracting deep into the intrinsic musculature, leading to adherence near the weight-bearing metatarsal head and causing severe, recalcitrant recurrent symptoms.
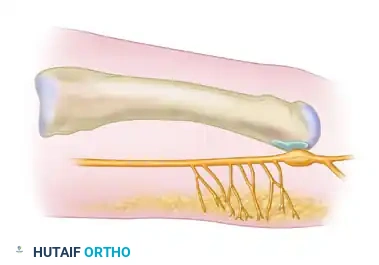
FIGURE 86-9 B: Lateral view of plantar branches of the digital nerve. (1) Previously recommended level of neurectomy; (2) Currently recommended level of neurectomy (at least 3 cm proximal to the ligament) to avoid plantarly directed nerve branches and prevent stump tethering.
The nerve must be transected at least 3 cm proximal to the ligament (Level 2 in the diagram above). Care must be taken during this proximal dissection not to injure the adjacent common digital branches supplying the second or fourth web spaces.
7. Closure:
The tourniquet is deflated, and meticulous hemostasis is achieved to prevent postoperative hematoma, which can lead to excessive scarring. The skin is closed with non-absorbable sutures. A bulky, compressive forefoot dressing is applied.
Surgical Technique: Plantar Approach for Recurrent Neuroma
Revision surgery for a "recurrent" interdigital neuroma (usually a symptomatic stump neuroma) is technically demanding. The results of revision surgery are not as predictably satisfactory as primary resection; up to 43% of patients in revision studies report dissatisfaction or major reservations regarding the efficacy of the procedure. Extensive preoperative counseling is mandatory.
For recurrent neuromas, a plantar approach is strictly recommended. The dorsal approach is fraught with difficulty due to dense scar tissue obscuring the nerve stump. The plantar approach allows the surgeon to identify the nerve in virgin, normal tissue proximally and dissect it distally into the scarred bed.
1. Incision:
A longitudinal or transverse plantar incision is made over the involved interspace, slightly proximal to the weight-bearing pad of the metatarsal heads.
2. Dissection:
The incision is carried through the plantar fat pad and plantar fascia. The deep transverse intermetatarsal ligament usually does not impair exposure of the proximal nerve from this approach and is typically left intact.
3. Nerve Identification and Resection:
The common digital nerve is identified in healthy tissue proximal to the previous surgical bed. Careful localization of the most tender area preoperatively helps guide the surgeon to the neuroma stump. Once identified, the nerve is dissected distally, freeing it from the surrounding scar tissue, and transected sharply as far proximally as possible, allowing the new stump to retract deep into the intrinsic muscles of the arch.
4. Closure:
The plantar fascia is not routinely repaired. The skin is closed with vertical mattress sutures to ensure eversion of the thick plantar skin.
POSTOPERATIVE PROTOCOL
Primary Dorsal Excision:
* 0-2 Weeks: Patients are placed in a rigid-soled postoperative shoe. Weight-bearing is permitted as tolerated, though heel-weight-bearing is encouraged to minimize forefoot swelling and wound tension. Elevation is critical for the first 48-72 hours.
* 2-3 Weeks: Sutures are removed once the incision is fully healed.
* 3-6 Weeks: Transition to a wide toe-box, supportive athletic shoe. High-impact activities and tight footwear are restricted.
* 6+ Weeks: Gradual return to full activities. Patients should be reminded that mild swelling and incisional sensitivity may persist for up to 3-4 months.
Revision Plantar Excision:
* 0-3 Weeks: Strict non-weight-bearing or touch-down weight-bearing in a controlled ankle motion (CAM) boot or splint to protect the plantar incision and prevent wound dehiscence or painful hypertrophic scarring.
* 3 Weeks: Suture removal. Gradual transition to weight-bearing in a rigid-soled shoe.
* Post-healing: Aggressive scar massage is instituted to desensitize the plantar scar.
CONCLUSION
Surgical excision of an interdigital neuroma is a highly effective procedure for alleviating the debilitating pain of this compressive neuropathy. However, success hinges on meticulous surgical technique—specifically, adequate proximal resection to prevent tethering by plantar branches—and rigorous preoperative patient counseling regarding the realities of postoperative numbness and the potential for residual, albeit improved, symptoms. When primary surgery fails, the plantar approach offers the most reliable anatomical exposure for managing the challenging stump neuroma.
You Might Also Like

