Mastering Shoulder Spaces: Essential Anatomy Revealed
Introduction & Epidemiology
Precise anatomical understanding of the shoulder girdle, particularly its intricate neurovascular spaces and intervals, is paramount for the orthopedic surgeon. Mastery of these regions facilitates accurate diagnosis, minimizes iatrogenic injury during surgical intervention, and optimizes patient outcomes. The shoulder's remarkable mobility relies on a complex interplay of osseous structures, ligaments, tendons, and muscles, all traversed by critical neurovascular bundles. Pathology arising within or adjacent to these confined spaces—such as nerve entrapment, vascular compromise, or tumor extension—often necessitates surgical intervention, underscoring the necessity of intimate anatomical knowledge.
Conditions affecting the neurovascular structures within these spaces, such as axillary nerve injury, suprascapular nerve entrapment, and radial nerve palsy, collectively present a significant clinical burden. Axillary nerve injury, for instance, can occur in up to 20% of proximal humerus fractures and 0.5-5% of primary shoulder arthroplasties or instability procedures. Suprascapular nerve entrapment, though less common, is a recognized cause of shoulder pain and weakness, particularly in overhead athletes, with varying reported incidence. Radial nerve palsy is the most frequent nerve injury associated with humeral shaft fractures, affecting 10-15% of patients. Surgical intervention in these areas demands not only an understanding of static anatomical boundaries but also their dynamic alterations during movement and surgical exposure.
Surgical Anatomy & Biomechanics
The shoulder girdle is anatomically rich, featuring multiple compartments, potential spaces, and critical neurovascular intervals. A thorough appreciation of these regions is fundamental to safe and effective surgical practice.

The primary focus for understanding critical posterior and posterolateral shoulder neurovascular anatomy lies within the quadrangular (quadrilateral) space, the triangular space, and the triangular interval. These three interconnected spaces are formed by the teres major, teres minor, long head of the triceps brachii, and the surgical neck or shaft of the humerus.
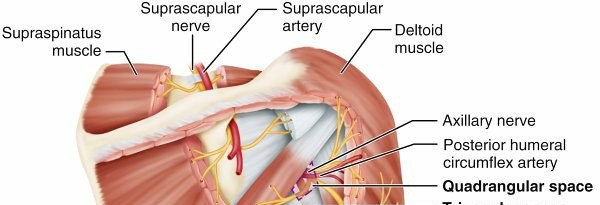
FIG. 2.4 Borders of the key spaces and intervals around the shoulder, including the suprascapular nerve course as well as the quadrangular space and triangular space/interval.
Table 2.3 Space Borders Nerve Artery
Quadrangular (quadrilateral) space
| Superior: lower border of teres minor
Inferior: upper border of teres major
Medial: long head of triceps Lateral: surgical neck of humerus | Axillary | Posterior
humeral circumflex
Triangular space
| Superior: lower border of teres minor
Inferior: upper border of teres major
Lateral: long head of triceps | |
Circumflex
scapular
Triangular interval
| Superior: lower border of teres major
Medial: long head of triceps Lateral: shaft of humerus | Radial | Profunda
brachii
Quadrangular (Quadrilateral) Space
This four-sided aperture is surgically significant due to its critical neurovascular contents.
*
Borders:
*
Superior:
Lower border of teres minor
*
Inferior:
Upper border of teres major
*
Medial:
Long head of triceps
*
Lateral:
Surgical neck of humerus
*
Contents:
The
axillary nerve
and the
posterior humeral circumflex artery
(with accompanying veins).
*
Clinical Significance:
The axillary nerve, a branch of the posterior cord of the brachial plexus (C5-C6), supplies motor innervation to the deltoid and teres minor muscles and provides sensory innervation to the "regimental badge" area over the deltoid. Its vulnerability within this space is high. It can be compressed (Quadrilateral Space Syndrome), particularly in overhead athletes or due to fibrous bands, hypertrophy of musculature, or space-occupying lesions. It is also at significant risk during approaches to the inferior capsule, posterior glenoid, proximal humeral fracture fixation, and deltoid detachment/repair. Damage can lead to profound deltoid weakness and atrophy. The posterior humeral circumflex artery is a major blood supply to the deltoid and humeral head.
Triangular Space (Medial Triangular Space)
This three-sided region, medial to the quadrangular space, primarily transmits a vascular structure.
*
Borders:
*
Superior:
Lower border of teres minor
*
Inferior:
Upper border of teres major
*
Lateral:
Long head of triceps
*
Contents:
The
circumflex scapular artery
(a branch of the subscapular artery, which itself is a branch of the axillary artery) and its accompanying veins.
*
Clinical Significance:
While no major nerve traverses this space, the circumflex scapular artery is crucial for collateral circulation around the scapula, especially in cases of proximal axillary artery occlusion. It also contributes to the blood supply of the infraspinatus and teres minor. It is a potential pedicle for free tissue transfer.
Triangular Interval (Lateral Triangular Space)
Located inferior and lateral to the quadrangular space, this interval is defined by musculature and bone.
*
Borders:
*
Superior:
Lower border of teres major
*
Medial:
Long head of triceps
*
Lateral:
Shaft of humerus
*
Contents:
The
radial nerve
and the
profunda brachii artery
(deep brachial artery) with its accompanying veins.
*
Clinical Significance:
The radial nerve (C5-T1), a major nerve of the upper limb, supplies the triceps brachii and all posterior compartment muscles of the forearm, as well as providing sensory innervation to a portion of the posterior forearm and hand. It spirals around the humerus in the radial groove (spiral groove), making it highly vulnerable to injury in mid-shaft humeral fractures. Surgical approaches to the posterior humerus, such as for fracture fixation, necessitate meticulous identification and protection of this nerve within the triangular interval as it transitions into the radial groove. The profunda brachii artery is the main arterial supply to the triceps brachii.

Other Critical Shoulder Spaces and Intervals
Beyond these three, several other anatomical spaces are surgically relevant for the shoulder surgeon.
-
Suprascapular Notch: Located on the superior border of the scapula, medial to the coracoid process. It is bridged by the superior transverse scapular ligament, which ossifies in a significant percentage of the population.
- Contents: The suprascapular nerve passes under the ligament, while the suprascapular artery and vein typically pass over the ligament.
- Clinical Significance: A common site for suprascapular nerve entrapment, leading to pain and weakness in the supraspinatus and infraspinatus muscles. Ganglion cysts, direct trauma, or ligament hypertrophy can cause compression.
-
Spinoglenoid Notch: Located between the glenoid neck and the base of the scapular spine.
- Contents: The motor branch of the suprascapular nerve to the infraspinatus muscle and terminal branches of the suprascapular artery and vein.
- Clinical Significance: Another site of suprascapular nerve entrapment, often associated with paralabral cysts, leading specifically to isolated infraspinatus atrophy and weakness.
-
Rotator Interval: An anatomical gap in the anterior-superior shoulder capsule, situated between the anterior border of the supraspinatus and the superior border of the subscapularis.
- Borders: Medially by the coracoid process, superiorly by the supraspinatus tendon, and inferiorly by the superior border of the subscapularis tendon.
- Contents: Contains the coracohumeral ligament (CHL), superior glenohumeral ligament (SGHL), and the biceps pulley system (reflected head of the long head of biceps brachii).
- Clinical Significance: Critical for shoulder stability, particularly resisting inferior translation and external rotation. It is a common site for arthroscopic portal placement (e.g., anterosuperior portal). Pathology here is associated with adhesive capsulitis (thickening/contraction of CHL and SGHL) and biceps tendon instability.
-
Subacromial Space: The potential space beneath the acromion and coracoacromial ligament, and above the rotator cuff.
- Contents: Subacromial-subdeltoid bursa, supraspinatus tendon.
- Clinical Significance: The primary site of impingement syndrome and rotator cuff pathology (bursitis, tendinopathy, tears). Surgical decompression (acromioplasty) and rotator cuff repair are commonly performed here.
-
Subdeltoid Space: A deeper extension of the subacromial space, between the deep surface of the deltoid muscle and the superficial surface of the rotator cuff/greater tuberosity.
- Contents: Subdeltoid bursa.
- Clinical Significance: Can be involved in bursitis or extensions of rotator cuff tears.

Biomechanics
The dynamic nature of the shoulder girdle significantly influences these spaces. Arm abduction and external rotation can stretch the axillary nerve, potentially increasing compression within the quadrangular space, especially in athletes. Similarly, arm positioning during surgery must consider the tension on neurovascular structures. For instance, excessive arm traction in lateral decubitus for arthroscopy can stretch the brachial plexus. Movements of the scapula and humerus dynamically alter the dimensions and relationships of all these critical spaces, impacting surgical exposure and safety.
Indications & Contraindications
Understanding the indications and contraindications for surgical intervention involving these shoulder spaces is essential for appropriate patient selection and risk stratification. Surgical indications generally arise from conditions causing neural compression, vascular compromise, or structural instability, or from the need for direct access for fracture fixation, tumor excision, or joint reconstruction.
Indications for Surgical Intervention
-
Nerve Entrapment Syndromes:
- Axillary Nerve (Quadrilateral Space Syndrome): Failed conservative management (physical therapy, NSAIDs, activity modification, injections), progressive motor weakness of the deltoid or teres minor, demonstrable muscle atrophy, persistent intractable pain, or a clear space-occupying lesion (e.g., ganglion cyst, fibrous band) on advanced imaging (MRI).
- Suprascapular Nerve (Suprascapular or Spinoglenoid Notch): Persistent pain and weakness (supraspinatus/infraspinatus) refractory to conservative treatment, documented progressive atrophy, electrophysiological evidence of ongoing denervation, or presence of a space-occupying lesion (ganglion cyst, osteophyte) causing compression.
- Radial Nerve (Triangular Interval/Humeral Shaft): Acute complete radial nerve palsy in the setting of an open humeral shaft fracture, persistent nerve palsy after appropriate observation (typically 3-6 months) for closed fractures without signs of recovery, nerve entrapment by fracture fragments or callus, or iatrogenic nerve laceration.
-
Vascular Pathology:
- Traumatic transection or pseudoaneurysm formation of the posterior humeral circumflex, circumflex scapular, or profunda brachii arteries.
- Vascular compromise requiring direct repair or bypass.
- Harvesting of vascularized flaps (e.g., circumflex scapular artery flap).
-
Trauma:
- Complex proximal humerus fractures or glenoid fractures requiring open reduction and internal fixation, where precise knowledge of the axillary nerve trajectory is critical.
- Humeral shaft fractures requiring open reduction and internal fixation where the radial nerve is at risk or requires exploration.
- Scapular fractures involving the suprascapular or spinoglenoid notches, necessitating nerve decompression.
-
Rotator Cuff Pathology:
- Symptomatic full-thickness rotator cuff tears unresponsive to conservative management.
- Arthroscopic subacromial decompression for impingement syndrome.
- Addressing paralabral cysts compressing the suprascapular nerve.
-
Shoulder Instability:
- Recurrent glenohumeral instability requiring capsular plication or labral repair, with particular attention to the axillary nerve during inferior capsular shifts.
- Management of rotator interval lesions.
- Tumors: Excision of soft tissue or osseous tumors located within or adjacent to these critical spaces.
- Infection: Drainage of deep-seated abscesses within these compartments.
Contraindications for Surgical Intervention
-
Absolute Contraindications:
- Uncontrolled systemic infection or sepsis.
- Significant medical comorbidities precluding safe anesthesia and surgery (e.g., severe cardiopulmonary disease, uncontrolled diabetes).
- Active local skin infection at the surgical site.
-
Relative Contraindications:
- Patient non-compliance with post-operative rehabilitation.
- Unrealistic patient expectations regarding outcomes.
- Minor symptoms responding well to conservative management.
- Poor soft tissue envelope or severe scarring from previous surgeries, increasing risk of iatrogenic injury.
Operative vs. Non-Operative Indications
| Condition/Pathology | Operative Indications | Non-Operative Indications |
|---|---|---|
| Axillary Nerve Entrapment (Quadrilateral Space Syndrome) | Failed conservative management (physical therapy, NSAIDs, injections), progressive motor weakness, muscle atrophy, persistent intractable pain, demonstrable space-occupying lesion (e.g., ganglion cyst). | Early presentation, mild or intermittent symptoms, no significant motor deficit, positive response to conservative measures (rest, activity modification, NSAIDs, targeted physical therapy, corticosteroid injections). |
| Suprascapular Nerve Entrapment (Notch/Spinoglenoid) | Persistent pain and weakness despite conservative management, progressive atrophy of supraspinatus/infraspinatus, electrodiagnostic evidence of ongoing denervation, presence of ganglion cyst or space-occupying lesion. | Mild symptoms, initial presentation, no significant motor deficit, response to physical therapy, NSAIDs, corticosteroid injections, small asymptomatic ganglion cysts. |
| Humeral Shaft Fractures with Radial Nerve Palsy | Open fractures with nerve laceration, neurovascular compromise, irreducible fractures, segmental fractures, pathological fractures, associated vascular injury, persistent radial nerve palsy after 3-6 months of observation for closed fractures without recovery, nerve entrapment by bone fragment. | Closed, stable, non-displaced or minimally displaced fractures, isolated radial nerve palsy at presentation in closed fractures (often observed for spontaneous recovery), acceptable alignment achievable with conservative means (coaptation splint, Sarmiento brace). |
| Rotator Cuff Tears | Full-thickness symptomatic tears, failed non-operative management, acute traumatic tears in younger/active patients, significant functional deficit, irreparable tears requiring advanced reconstruction techniques. | Partial-thickness tears, small asymptomatic full-thickness tears, elderly/low-demand patients, good response to physical therapy/injections, tendinopathy. |
| Shoulder Instability (e.g., Recurrent Dislocations) | Recurrent dislocations/subluxations despite comprehensive rehabilitation, significant bony defects (e.g., large Bankart or Hill-Sachs lesions), engagement lesion, failed arthroscopic stabilization. | First-time traumatic dislocation (especially in older patients without significant risk factors for recurrence), voluntary subluxation/dislocation (often psychological, requires careful assessment), generalized hyperlaxity without functional impairment. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical for minimizing complications and achieving optimal surgical outcomes when operating around the shoulder spaces.
Pre-Operative Planning
- Clinical Assessment: A thorough history focusing on the onset, duration, character, and aggravating/alleviating factors of symptoms. A comprehensive physical examination should assess range of motion, strength, sensation, specific provocative tests, and neurovascular status.
-
Imaging:
- Radiographs: Essential for evaluating osseous pathology (fractures, osteophytes, degenerative changes). Specific views (e.g., trauma series for humerus) are crucial.
- Magnetic Resonance Imaging (MRI): Gold standard for soft tissue evaluation, delineating rotator cuff integrity, labral pathology, capsular status, and most importantly, identifying nerve compression (e.g., ganglion cysts, fibrous bands) or nerve edema/atrophy. MR Neurography can offer enhanced nerve visualization.
- Computed Tomography (CT) Scan: Superior for complex bony anatomy (fractures, glenoid erosion, scapular morphology). Can be combined with angiography (CTA) for vascular assessment.
- Electrodiagnostic Studies (EMG/NCS): Indispensable for confirming nerve entrapment, localizing the lesion, assessing severity (neuropraxia, axonotmesis, neurotmesis), and monitoring recovery, especially for axillary, suprascapular, and radial nerve palsies.
- Surgical Approach Selection: Based on the pathology, anatomical location, and surgeon preference, selecting the most appropriate open or arthroscopic approach. This selection directly impacts which spaces are accessed, or which neurovascular structures are at risk.
- Informed Consent: Detailed discussion with the patient regarding the proposed procedure, expected outcomes, and specific risks, including neurovascular injury (e.g., axillary, suprascapular, radial nerve palsy) and potential complications.
Patient Positioning
The choice of patient position dictates surgical exposure, access to specific spaces, and management of neurovascular bundles.
-
Beach Chair Position:
- Advantages: Excellent for anterior, superior, and some posterior aspects of the shoulder. Allows for easy conversion to open procedures. Provides good airway control and ability to assess neurovascular status of the hand.
- Setup: Patient is semi-recumbent (30-70 degrees of trunk elevation). Head stabilized to prevent lateral flexion or rotation. The affected arm is typically supported in a traction device or freely draped.
- Considerations for Spaces: Ideal for subacromial decompression, rotator cuff repair, instability repair, and suprascapular nerve decompression (anterior approach). Care must be taken to prevent brachial plexus stretch, especially with head rotation, and to pad the ulnar nerve at the elbow.
-
Lateral Decubitus Position:
- Advantages: Excellent for posterior, superior, and lateral aspects of the shoulder. Often preferred for arthroscopic procedures involving the posterior capsule, glenoid, or spinoglenoid notch. Provides gravity-assisted glenohumeral distraction.
- Setup: Patient is positioned on the unaffected side, secured with axillary roll and hip/torso supports. The affected arm is suspended in a traction tower with weights (typically 10-15 lbs).
- Considerations for Spaces: Optimal for accessing the posterior aspect of the glenohumeral joint, spinoglenoid notch for suprascapular nerve decompression, and posterior aspects of the humerus. Extreme care required to pad all pressure points, especially the contralateral axilla (brachial plexus), ulnar nerve, and peroneal nerve. Excessive traction can cause traction neurapraxia of the brachial plexus.
-
Prone Position:
- Advantages: Less common for general shoulder surgery but can provide excellent access for posterior scapular or posterior humeral shaft pathologies, offering direct visualization of the quadrangular, triangular, and triangular interval spaces.
- Setup: Patient is prone on the operating table, supported by chest rolls. The arm can be freely draped or supported.
- Considerations for Spaces: When performing extensive posterior approaches to the scapula or proximal humerus, this position allows for direct visualization of the teres major/minor interval and the long head of the triceps. Special attention to padding the face, eyes, and neurovascular structures in the neck and upper extremities.
Regardless of position, neurovascular status (e.g., radial pulse, capillary refill) must be frequently monitored. Regional nerve blocks (e.g., interscalene block) can aid in post-operative pain control but can also mask immediate signs of iatrogenic nerve injury, necessitating careful intra-operative assessment.
Detailed Surgical Approach / Technique
Surgical intervention involving shoulder spaces necessitates precise anatomical dissection, a clear understanding of internervous planes, and meticulous technique to protect vital neurovascular structures. The specific approach chosen is dictated by the pathology and the target anatomical space.
General Principles of Dissection
- Anatomical Landmarks: Always identify superficial and deep anatomical landmarks.
- Internervous Planes: Utilize internervous planes whenever possible to minimize muscle injury and preserve function.
- Neurovascular Identification: Proactively identify, dissect, and protect all at-risk neurovascular structures. Magnification (loupes) is highly recommended.
- Hemostasis: Meticulous hemostasis to maintain a clear surgical field and prevent hematoma formation, which can compromise nerve recovery.
Approaches Relevant to Specific Spaces
1. Posterior Approach to the Shoulder (Utilizing Teres Minor/Major Interval)
This approach provides access to the posterior glenoid, infraspinatus, teres minor, and the quadrangular space.
- Indications: Posterior instability, glenoid fractures, infraspinatus/teres minor repair, posterior glenohumeral arthrodesis, and exploration/decompression of the quadrangular space.
- Patient Positioning: Lateral decubitus or Beach Chair, allowing for adequate posterior exposure.
- Incision: A curvilinear incision starting from the posterolateral corner of the acromion, extending inferiorly along the posterior deltoid border for 6-8 cm.
- Superficial Dissection: Skin and subcutaneous tissues are incised. The posterior deltoid fascia is identified.
- Internervous Plane: The deltoid muscle (innervated by the axillary nerve) can be split. Crucially, the split should be limited to 5 cm distal to the acromial angle to avoid injury to the axillary nerve, which wraps around the surgical neck of the humerus approximately 5-7 cm from the acromion. Deep to the deltoid, the interval between the infraspinatus and teres minor (both supplied by the suprascapular nerve and axillary nerve respectively) can be exploited.
-
Deep Dissection:
- Deltoid Reflection: The posterior deltoid is either split or elevated off the posterior aspect of the scapular spine, exposing the infraspinatus and teres minor.
- Identification of Teres Minor/Major Interval: The infraspinatus (superior) and teres minor (inferior) muscles are identified. The teres major lies inferior to the teres minor. The interval between the teres minor (superior) and teres major (inferior) is developed.
- Quadrangular Space Exposure: By retracting the teres minor superiorly and the teres major inferiorly, and the long head of triceps medially, the quadrangular space is visualized. The surgical neck of the humerus forms its lateral border.
- Neurovascular Protection: The axillary nerve and posterior humeral circumflex artery emerge from the quadrangular space and wrap around the surgical neck of the humerus. These structures must be identified and protected. This is often the most critical step. For direct access to the posterior humerus, the deltoid is often elevated carefully from the humerus, exposing the nerve and vessel.
-
Surgical Maneuvers within the Quadrangular Space:
- For axillary nerve decompression: Careful release of fibrous bands, excision of ganglion cysts.
- For fracture fixation: Plate application on the posterior aspect of the humerus, ensuring screws do not violate the nerve.
2. Posterior Approach to the Humeral Shaft (Triceps Splitting Approach)
This approach is primarily used for humeral shaft fractures and provides access to the triangular interval.
- Indications: Humeral shaft fractures requiring open reduction and internal fixation, particularly those with associated radial nerve palsy, or tumor excision from the posterior humerus.
- Patient Positioning: Prone or lateral decubitus.
- Incision: A longitudinal incision centered over the posterior aspect of the humerus.
- Superficial Dissection: Skin and subcutaneous tissues are incised. The deep fascia is opened.
- Internervous Plane: No true internervous plane is utilized here; rather, the triceps muscle is split.
-
Deep Dissection:
- Triceps Identification: The long head of the triceps (most medial), lateral head, and medial head are identified.
- Triceps Split: A longitudinal split is made through the belly of the triceps (often through the long head or between the long and lateral heads), exposing the humeral shaft.
- Triangular Interval Exposure: As the triceps is retracted, the triangular interval is visible between the teres major (superior), long head of triceps (medial), and humeral shaft (lateral).
- Neurovascular Identification: The radial nerve and profunda brachii artery lie within the triangular interval, deep to the triceps, intimately associated with the periosteum of the posterior humeral shaft in the spiral groove. These structures are identified proximally within the triangular interval and traced distally.
- Protection: The radial nerve and profunda brachii artery are carefully dissected free from the humerus and protected (e.g., with vessel loops) throughout the procedure.
3. Suprascapular Nerve Decompression
- Indications: Suprascapular nerve entrapment syndrome (suprascapular or spinoglenoid notch), often due to ganglion cysts, hypertrophied ligaments, or traction injury.
-
Approaches:
-
Open Posterior Approach:
- Incision: Oblique incision along the scapular spine.
- Dissection: Deltoid detached from the scapular spine, retracted laterally. Infraspinatus muscle exposed. For suprascapular notch: infraspinatus is retracted inferiorly. For spinoglenoid notch: infraspinatus is split or retracted.
- Notch Identification: The suprascapular or spinoglenoid notch is carefully identified.
- Nerve Release: The superior transverse scapular ligament (for suprascapular notch) or spinoglenoid ligament (for spinoglenoid notch) is sharply incised, decompressing the nerve. Any ganglion cysts are excised.
-
Arthroscopic Approach:
Increasingly preferred, utilizing posterior and anterolateral portals.
- Technique: Arthroscope is placed to visualize the suprascapular notch or spinoglenoid notch. Specialized instruments are used to identify and release the compressing ligament or resect the ganglion cyst. This avoids deltoid detachment and minimizes soft tissue disruption.
-
Open Posterior Approach:
4. Rotator Cuff Repair / Subacromial Decompression (Involving Subacromial/Subdeltoid Spaces)
- Indications: Symptomatic rotator cuff tears, impingement syndrome.
- Approach: Open, mini-open, or arthroscopic.
-
Technique:
- Portal/Incision: Arthroscopic portals (posterior, lateral, anterolateral) or a mini-open deltoid-splitting incision (limited to 5 cm from acromion to protect axillary nerve) are established.
- Subacromial Space Preparation: The subacromial bursa is debrided to expose the rotator cuff and undersurface of the acromion.
- Acromioplasty (if indicated): Bone resection of the anterior-inferior acromion to create more space for the rotator cuff.
- Cuff Repair: Torn rotator cuff tendons are mobilized and repaired to their footprint on the greater tuberosity using suture anchors.
- Rotator Interval Management: For specific instability patterns or biceps pathology, the rotator interval can be addressed (e.g., capsular plication, biceps tenodesis/tenotomy).
Reduction and Fixation
When treating fractures (e.g., proximal humerus, humeral shaft), the principles of reduction and fixation must be integrated with anatomical knowledge of the surrounding spaces:
- Indirect Reduction Techniques: Minimally invasive plate osteosynthesis (MIPO) can reduce soft tissue stripping and further neurovascular compromise.
- Direct Reduction: When necessary, open reduction is performed with careful identification and protection of nerves and vessels (e.g., axillary nerve in proximal humerus fracture fixation, radial nerve in humeral shaft plating).
- Plate Positioning: Plates for proximal humerus fractures should be positioned anteriorly or laterally to avoid impinging on the axillary nerve posteriorly. Distal screws must not penetrate the quadrangular space or impinge on the axillary nerve. For humeral shaft plating, plates are often placed laterally to reduce radial nerve exposure, but if posterior placement is chosen, the radial nerve must be elevated and protected.
- Screws: Screw length must be carefully measured to avoid neurovascular penetration on the far cortex, particularly in regions adjacent to the triangular interval and quadrangular space.
Complications & Management
Surgical interventions around the shoulder spaces, despite meticulous technique, carry inherent risks of complications, particularly neurovascular injuries. Proactive prevention, early recognition, and appropriate management are crucial.
General Complications
- Infection: Superficial or deep surgical site infections.
- Hematoma/Seroma: Accumulation of blood or fluid, potentially compressing nerves.
- Adhesive Capsulitis (Stiffness): Post-operative shoulder stiffness, especially after open procedures or prolonged immobilization.
- Deep Venous Thrombosis (DVT) / Pulmonary Embolism (PE): Though less common in shoulder surgery than lower extremity procedures, remains a risk.
- Anesthetic Complications: Related to regional or general anesthesia.
Specific Neurovascular Complications and Management
| Complication | Incidence | Salvage Strategies |
|---|---|---|
| Axillary Nerve Injury | Varies widely (e.g., 0.5-20% in specific surgeries like reverse TSA, instability repair, proximal humerus fx fixation, deltoid detachment). |
Prevention:
Meticulous dissection, careful portal placement (arthroscopy), limited deltoid splitting (max 5 cm from acromion), identifying nerve safe zones.
Management: 1. Observation: For neuropraxia (most common type, especially after traction or blunt trauma) spontaneous recovery often occurs within 6-12 months. Regular clinical assessment for deltoid function and sensation. 2. Electrodiagnostic Monitoring (EMG/NCS): Essential for confirming injury, localizing, assessing severity, and tracking recovery. Performed at 3-6 weeks post-injury, then periodically. 3. Nerve Exploration: Indicated for open injuries with suspected laceration, closed injuries with no signs of recovery after 3-4 months (complete motor loss, no EMG evidence of reinnervation), or presence of known compressive lesion not amenable to conservative care. Neurolysis for compression, direct repair (primary neurorrhaphy) for clean lacerations, or nerve grafting for gaps. 4. Tendon Transfers: For irreparable axillary nerve damage or failed nerve repair (e.g., latissimus dorsi or triceps transfer to replace deltoid function), typically considered after 12-18 months with no recovery. |
| Suprascapular Nerve Injury | Varies (e.g., 10-30% in massive rotator cuff tears, 1-5% iatrogenic during rotator cuff repair or glenoid surgery). |
Prevention:
Careful dissection around the suprascapular and spinoglenoid notches, avoidance of excessive traction.
Management: 1. Observation: For mild neuropraxia, recovery can occur. Physiotherapy for muscle re-education. 2. Electrodiagnostic Monitoring: To assess nerve function and recovery. 3. Decompression: Surgical release of the superior transverse scapular ligament or spinoglenoid ligament (open or arthroscopic), excision of paralabral cysts or space-occupying lesions. This is the primary treatment for entrapment. 4. Nerve Repair/Grafting: Less common, but considered for direct nerve lacerations, often with poor outcomes. 5. Tendon Transfers: For chronic, irreparable nerve damage with significant muscle atrophy (e.g., trapezius transfer for supraspinatus function, deltoid for infraspinatus). |
| Radial Nerve Injury | 10-15% in humeral shaft fractures (often neuropraxia), 1-2% iatrogenic in posterior approaches to the humerus. |
Prevention:
Meticulous identification and protection during humeral shaft fixation, careful retraction.
Management: 1. Observation: Most common strategy for radial nerve palsy associated with closed humeral shaft fractures (neuropraxia). Spontaneous recovery occurs in 70-90% within 3-6 months. Splinting for wrist drop. 2. Electrodiagnostic Monitoring: Essential for assessing nerve status and recovery. 3. Nerve Exploration: Indicated for open fractures with nerve laceration, no signs of recovery after 3-4 months (for closed fracture-associated palsy), or nerve entrapment by fracture fragments or hardware. Neurolysis, direct repair, or nerve grafting. 4. Tendon Transfers: For chronic, irreparable radial nerve damage with persistent wrist and finger drop (e.g., pronator teres to ECRB, FCR to EDC, palmaris longus to EPL), typically after 12-18 months with no recovery. |
| Vascular Injury (e.g., Posterior Humeral Circumflex Artery, Profunda Brachii Artery) | Rare (<1% in most shoulder surgeries), but potentially limb-threatening if major vessels involved. |
Prevention:
Careful subperiosteal dissection, sharp dissection away from known vascular pathways, clear visualization.
Management: 1. Immediate Hemostasis: Direct pressure, tourniquet application (if feasible), vessel clamping. 2. Ligation: For smaller, non-critical vessels with good collateral circulation (e.g., terminal branches of posterior humeral circumflex if primary supply to humeral head is intact). 3. Repair: For larger, critical vessels; direct repair, interpositional vein graft, or synthetic graft by a vascular surgeon. Requires immediate recognition and surgical intervention to prevent ischemia. |
| Rehabilitation Non-Compliance/Poor Adherence | Common, patient-dependent. |
Prevention:
Pre-operative patient education, clear post-operative instructions, realistic goal setting.
Management: Intensive physical therapy, supervised rehabilitation programs, pain management, psychological support, manipulation under anesthesia for severe stiffness (if not improving with therapy). |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is integral to optimizing outcomes following shoulder surgery, particularly when neurovascular structures within key anatomical spaces have been addressed or were at risk. Protocols must be individualized, progressive, and responsive to the specific surgical procedure, quality of repair, and patient factors.
General Principles
- Pain Management: Adequate pain control is essential to facilitate early motion and patient compliance.
- Protection of Repair/Nerve: Initial immobilization or protected motion to safeguard surgical repairs (e.g., rotator cuff, nerve repair) and prevent undue tension on healing structures.
- Early Controlled Motion: Gradually progressing range of motion (ROM) to prevent stiffness, promote cartilage nutrition, and reduce scar tissue formation.
- Gradual Strengthening: Progressive resistance exercises to restore muscle strength and endurance.
- Neuromuscular Re-education: Specific exercises to improve proprioception, motor control, and coordination.
- Functional Progression: Tailoring activities to restore specific functional demands, including return to activities of daily living (ADLs), work, and sport.
Specific Considerations for Procedures Involving Shoulder Spaces
-
Nerve Decompression/Repair (Axillary, Suprascapular, Radial Nerves):
- Immobilization: Initial period (2-6 weeks) of immobilization in a brace or sling, often in a position that minimizes tension on the repaired or decompressed nerve. For radial nerve repair, a wrist extension splint may be used.
- Protected ROM: Gentle, passive range of motion, avoiding positions of extreme stretch for the specific nerve. For axillary nerve, caution with abduction and external rotation; for suprascapular nerve, caution with arm adduction and internal rotation; for radial nerve, caution with wrist/finger flexion.
- Neuromuscular Re-education: Specific exercises to stimulate reinnervated muscles, often involving biofeedback or electrical stimulation.
- Sensory Re-education: For sensory nerve recovery, techniques to retrain sensation.
- Progression: Gradual increase in ROM and strengthening as nerve recovery progresses (monitored clinically and with EMG/NCS). Return to full activity is often prolonged, guided by nerve regeneration.
-
Rotator Cuff Repair / Subacromial Decompression:
-
Phase 1 (0-6 weeks): Protection and Passive Motion:
- Sling immobilization (except for hygiene and exercises).
- Passive range of motion (PROM) within protected arcs, avoiding active elevation and external rotation. Focus on pendulum exercises, supine passive elevation.
- Emphasis on maintaining integrity of the rotator cuff repair in the subacromial space.
-
Phase 2 (6-12 weeks): Active-Assisted and Active Motion:
- Gradual discontinuation of sling.
- Active-assisted range of motion (AAROM) followed by active range of motion (AROM).
- Light isometric exercises for rotator cuff and scapular stabilizers.
-
Phase 3 (12-24 weeks): Strengthening and Advanced Activities:
- Progressive resistance exercises, targeting rotator cuff, deltoid, and scapular musculature.
- Emphasis on functional movements and endurance.
- Return to sport-specific training.
- Phase 4 (24+ weeks): Return to Sport/Work: Gradual return to full activities, guided by functional assessment and strength.
-
Phase 1 (0-6 weeks): Protection and Passive Motion:
-
Humeral Shaft Fracture Fixation (Radial Nerve at Risk/Repaired):
- Immobilization: Post-operative splint or brace for initial protection of fracture fixation.
- Early Motion: Early elbow and wrist ROM is encouraged to prevent stiffness, provided fracture stability allows and the radial nerve is not under undue tension if repaired.
- Radial Nerve Management: If radial nerve was repaired, strict immobilization to protect the repair site may be necessary for several weeks. If nerve was only explored or observed, wrist/finger splinting to prevent contractures while awaiting nerve recovery.
- Progressive Strengthening: Once fracture healing is evident and nerve recovery (if applicable) begins, progressive strengthening of the shoulder, elbow, wrist, and hand.
Long-Term Goals
- Restoration of full, pain-free range of motion.
- Return to pre-injury strength and functional capacity.
- Prevention of re-injury.
- For nerve injuries, maximal possible nerve recovery and functional adaptation.
Regular communication between the surgeon and rehabilitation team is paramount to tailor protocols and address any complications or plateaus in recovery.
Summary of Key Literature / Guidelines
The understanding and surgical management of shoulder spaces and their contained neurovascular structures are supported by a substantial body of literature, including anatomical studies, clinical series, and consensus guidelines.
- Anatomical Studies: Seminal cadaveric dissection studies remain foundational for delineating the precise borders and contents of the quadrangular space, triangular space, triangular interval, suprascapular notch, and spinoglenoid notch. These studies have defined "safe zones" for various surgical approaches (e.g., axillary nerve distance from the acromion, location of the radial nerve in relation to the spiral groove). For example, studies by Duparc et al. and Vastamäki et al. have provided detailed morphometric data on the suprascapular and spinoglenoid notches and the associated ligaments, guiding decompression techniques.
-
Axillary Nerve Injury/Quadrilateral Space Syndrome:
- Literature highlights the various etiologies, from trauma (proximal humerus fractures, dislocations) to iatrogenic causes (inferior capsular shifts, deltoid detachment, portal placement in arthroscopy).
- Guidance on "safe zones" for arthroscopic portals (e.g., posterior portal 2-3 cm inferior and 1 cm medial to the posterolateral acromial corner) aims to minimize axillary nerve injury.
- Studies by Cahill et al. and Hang et al. have characterized Quadrilateral Space Syndrome, detailing diagnostic criteria (MRI, EMG/NCS) and advocating for surgical decompression in refractory cases.
-
Suprascapular Nerve Entrapment:
- Numerous articles describe the pathology at the suprascapular and spinoglenoid notches, often involving ganglion cysts, hypertrophied ligaments, or traction injuries (e.g., massive rotator cuff tears, overhead athletes).
- The American Academy of Orthopaedic Surgeons (AAOS) and other societies provide guidelines for the diagnosis and management of shoulder pain, which often include consideration of nerve entrapment. Arthroscopic decompression has gained favor due to its less invasive nature compared to open techniques, with literature supporting good clinical outcomes.
-
Radial Nerve Palsy in Humeral Fractures:
- Consensus is generally to observe isolated radial nerve palsies associated with closed humeral shaft fractures for 3-6 months, given the high rate of spontaneous recovery (70-90%).
- Guidelines from trauma societies (e.g., Orthopaedic Trauma Association - OTA) outline indications for early nerve exploration (open fractures, vascular injury, nerve entrapment by hardware, no early signs of recovery).
- Surgical approaches to the humeral shaft, such as the posterior triceps-splitting approach, emphasize careful identification and protection of the radial nerve due to its intimate course in the spiral groove.
-
Rotator Interval and Instability:
- Research has elucidated the role of the rotator interval capsule and its ligaments (coracohumeral, superior glenohumeral) in glenohumeral stability and its involvement in adhesive capsulitis.
- Arthroscopic management of rotator interval pathology for instability or stiffness is well-documented, with studies demonstrating efficacy in improving range of motion and stability.
-
Arthroscopic Techniques and Nerve at Risk:
- Extensive literature defines the anatomical relationship of arthroscopic portals to surrounding neurovascular structures. For example, anterior portals carry a risk to the musculocutaneous nerve and cephalic vein, while posterior portals are generally safer but still require careful placement. The risk of axillary nerve injury from excessively inferior or deep anterior portals is a consistent theme.
- Guidelines for safe portal placement are routinely updated as arthroscopic techniques evolve.
The academic orthopedic surgeon is continually engaged with this evolving body of evidence to refine diagnostic algorithms, optimize surgical techniques, and improve patient care in the complex domain of shoulder pathology. Maintaining an up-to-date knowledge of these key anatomical spaces and their surgical implications is a continuous commitment to excellence in practice.
Clinical & Radiographic Imaging

