Pinpoint Posterior GH Instability: Diagnosis & Causes
Introduction & Epidemiology
Posterior glenohumeral (GH) instability represents a spectrum of conditions ranging from subtle subluxation to complete dislocation. While less common than anterior instability, it accounts for approximately 2-10% of all GH instabilities and often presents with delayed diagnosis due to its subtle clinical presentation and non-specific symptoms. A high index of suspicion is crucial, as chronic posterior instability can lead to significant functional impairment, pain, and articular cartilage degeneration.
The etiology of posterior instability is multi-factorial, encompassing traumatic, atraumatic, and microtraumatic mechanisms. Traumatic posterior dislocations are typically caused by axial loading of an adducted, internally rotated, and flexed arm, often seen in falls onto an outstretched hand (FOOSH), direct blows to the anterior shoulder, or convulsive disorders (seizures, electrocution). Atraumatic instability can be volitional or non-volitional, often associated with generalized ligamentous laxity, muscular imbalances, or repetitive overhead activities that stress the posterior capsule and labrum. Specific populations at higher risk include athletes involved in contact sports (e.g., American football linemen, rugby players), weightlifters, and individuals with neuromuscular disorders. Accurate diagnosis and understanding of the underlying causes are paramount for effective management and prevention of recurrence.
Surgical Anatomy & Biomechanics
A thorough understanding of the intricate anatomy and biomechanics of the posterior GH joint is fundamental to diagnosing and treating posterior instability. Stability is conferred by a complex interplay of static and dynamic restraints.
Bony Anatomy
- Glenoid Morphology : The glenoid fossa, typically pear-shaped, exhibits normal retroversion ranging from 0 to 7 degrees. Excessive glenoid retroversion (>7-10 degrees) reduces the anterior-posterior depth of the glenoid concavity, predisposing the shoulder to posterior subluxation or dislocation. Congenital glenoid hypoplasia or dysplastic morphology can further exacerbate this.
-
Humeral Head Morphology
:
- Reverse Hill-Sachs Lesion (Posteromedial Humeral Head Defect) : This impression fracture on the anteromedial aspect of the humeral head occurs when the posterior glenoid rim impacts the humeral head during a posterior dislocation. Its presence indicates a prior dislocation. An "engaging" reverse Hill-Sachs lesion, where the defect engages with the posterior glenoid rim during internal rotation and adduction, contributes significantly to recurrent instability.
- Reverse Bony Bankart Lesion : A fracture of the posterior-inferior glenoid rim, occurring due to the impact of the humeral head, leading to bone loss and a reduced glenoid articular arc.
- Posteromedial Humeral Head Osteonecrosis : A rare complication following posterior dislocation, particularly if reduction is delayed.
Soft Tissue Stabilizers
-
Capsuloligamentous Complex
:
- Posterior Capsule : A thickening of the posterior joint capsule, contributing significantly to posterior stability.
- Posterior Band of the Inferior Glenohumeral Ligament (IGHL) : The primary static stabilizer resisting posterior translation of the humeral head, especially when the arm is in adduction, flexion, and internal rotation. It forms part of the inferior glenohumeral ligament complex, which also includes the anterior band.
- Superior Glenohumeral Ligament (SGHL) and Coracohumeral Ligament (CHL) : Primarily resist inferior and external rotation forces but contribute secondarily to overall capsular tension.
-
Glenoid Labrum
: A fibrocartilaginous ring that deepens the glenoid fossa, increasing the contact area and providing a bumper effect.
- Posterior Labral Tears (Reverse Bankart Lesions) : Detachment of the posterior labrum from the glenoid rim, often accompanied by a posterior capsular avulsion.
- Kim Lesion : An avulsion of the posterior-inferior labrum from the glenoid rim with an associated partial tear or delamination of the glenoid cartilage, but without a discrete labral tear. This lesion is often subtle and can be missed.
-
Rotator Cuff Muscles (Dynamic Stabilizers)
:
- Infraspinatus and Teres Minor : These external rotators and posterior stabilizers are critical in counteracting posterior translation of the humeral head. Their coordinated action compresses the humeral head into the glenoid, particularly during overhead activities. Weakness or delayed activation of these muscles can contribute to posterior instability.
- Subscapularis : While primarily an internal rotator, its tendon contributes to anterior and inferior capsular stability, indirectly influencing posterior stability by maintaining overall GH joint mechanics.
- Scapular Stabilizers : The muscles responsible for scapular control (e.g., trapezius, rhomboids, serratus anterior) indirectly contribute to GH stability by providing a stable base for the glenoid. Scapular dyskinesis can alter the glenoid orientation, predisposing to instability.
Biomechanics of Instability
Posterior GH instability typically occurs when the arm is loaded in positions of adduction, internal rotation, and flexion. This position places maximal stress on the posterior capsule and labrum. Common mechanisms include:
*
Direct Trauma
: A direct blow to the anterior shoulder (e.g., football tackle) driving the humeral head posteriorly.
*
Axial Load
: A fall onto an outstretched arm, particularly when the arm is internally rotated and adducted.
*
Seizure/Electrocution
: Uncontrolled muscular contractions can lead to powerful internal rotation and adduction forces, causing bilateral posterior dislocations.
*
Repetitive Microtrauma
: In athletes, repeated eccentric loading of the posterior capsule and labrum can lead to stretching and attenuation.
Indications & Contraindications
Accurate diagnosis is paramount, as chronic posterior instability often results from missed or delayed recognition of the initial injury.
Diagnostic Approach
-
History
:
- Mechanism of Injury : Crucial for traumatic cases (FOOSH, direct blow, seizure). In atraumatic cases, inquire about repetitive activities, generalized laxity, and whether the instability is voluntary or involuntary.
- Symptoms : Posterior shoulder pain (often deep-seated), clicking, popping, catching, weakness, or a sense of apprehension/instability, especially during overhead activities or activities requiring internal rotation/adduction.
- Prior Treatments : Previous dislocations, attempts at reduction, rehabilitation efforts.
-
Physical Examination
:
- Observation : Look for signs of scapular dyskinesis, muscle atrophy (infraspinatus, teres minor), or obvious deformity (rare in subluxation).
- Range of Motion (ROM) : May be normal or limited by pain. Often, apprehension is noted with internal rotation, flexion, and adduction.
- Palpation : Tenderness over the posterior joint line.
-
Special Tests
:
- Posterior Apprehension Test : With the patient supine, the examiner applies a posterior force to the humeral head while moving the arm into flexion, adduction, and internal rotation. A positive test elicits apprehension or muscle guarding.
- Jerk Test : With the patient seated, the examiner grasps the elbow and internally rotates the arm, flexing it to 90 degrees. An axial load is then applied through the humerus while the arm is horizontally adducted. A sudden "jerk" or clunk indicates posterior subluxation, and a second clunk may be felt as the arm is returned to abduction.
- Kim Test : With the patient seated, the arm is abducted to 90 degrees. The examiner holds the elbow and lateral aspect of the proximal arm. An axial load and 45-degree elevation are applied, while a posterior and inferior force is applied to the proximal arm. A sudden pain in the posterior shoulder indicates a positive test for posteroinferior labral avulsion.
- Posterior Load and Shift Test : Performed with the patient supine, arm in 90 degrees abduction and slight flexion. The humeral head is loaded posteriorly, and the degree of translation is assessed relative to the glenoid (0-III).
- Sulcus Sign : Although typically associated with multidirectional instability, it can be present.
-
Imaging
:
-
Plain Radiographs
:
- Standard Series : AP, scapular Y, and axillary views. Often normal or subtly abnormal.
- Specific Views : West Point axillary view or Stryker notch view to assess for bony Bankart or Hill-Sachs lesions. Posterior dislocations can be missed on standard AP views.
-
Look for increased glenoid retroversion or a posterior osteochondral defect on the humeral head.

-
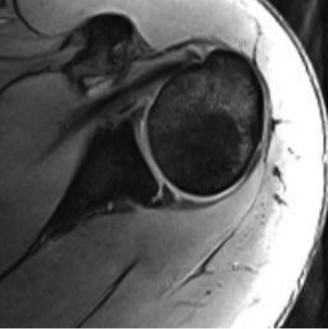
Magnetic Resonance Imaging (MRI) / MR Arthrography (MRA)
:
- The gold standard for evaluating soft tissue lesions.
- MRI : Identifies posterior labral tears (reverse Bankart), capsular avulsions, chondral damage, rotator cuff pathology, and bone bruising.
-
MRA
: Provides superior detail of the labrum and capsule by distending the joint with contrast, making subtle lesions like Kim lesions more apparent. It can delineate the exact extent of labral detachment and capsular laxity.

-
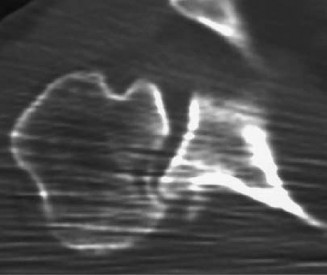
Computed Tomography (CT) / 3D CT
:
- Essential for assessing bony pathology, particularly glenoid bone loss, glenoid retroversion, and the size/location of a reverse Hill-Sachs lesion.
-
3D CT reconstruction
: Allows for accurate quantification of glenoid bone loss and assessment of the 'engaging' nature of a reverse Hill-Sachs lesion, critical for surgical planning.

-
Plain Radiographs
:
Indications for Operative vs. Non-Operative Management
The decision to proceed with operative versus non-operative management is individualized, based on the patient's age, activity level, frequency and severity of instability, associated pathology, and response to conservative treatment.
| Indication Category | Non-Operative Management | Operative Management |
|---|---|---|
| Instability Type | First-time subluxation/dislocation, atraumatic/voluntary (if controllable) | Recurrent instability (subluxation or dislocation), traumatic instability |
| Symptoms | Mild pain, minimal functional impairment | Significant pain, functional limitation, apprehension preventing activities |
| Associated Pathology | No significant labral tear, minimal/no bone loss, no engaging Hill-Sachs | Significant reverse Bankart lesion, Kim lesion, significant glenoid bone loss (>10-15%), engaging reverse Hill-Sachs lesion, capsular laxity |
| Patient Factors | Low-demand individuals, good compliance with rehab, older patients with low activity | High-demand athletes, younger patients, failed non-operative treatment, seizure patients with bony defects |
| Glenoid Retroversion | Normal or mild retroversion | Pathologic retroversion contributing to instability |
Contraindications
- Absolute : Active infection, severe medical comorbidities precluding safe anesthesia and surgery.
- Relative : Unrealistic patient expectations, poor compliance with post-operative rehabilitation, psychiatric conditions leading to volitional instability without structural pathology.
Pre-Operative Planning & Patient Positioning
Careful pre-operative planning is essential for a successful outcome in posterior GH stabilization, particularly given the often complex nature of the pathology.
Patient Education & Consent
- Comprehensive discussion regarding the diagnosis, surgical procedure, potential risks (e.g., recurrence, stiffness, nerve injury, infection), expected outcomes, and the rigorous post-operative rehabilitation protocol.
- Informed consent should explicitly cover the possibility of open conversion if arthroscopic findings necessitate it, or if significant bone loss is encountered.
Anesthesia
- Typically, general anesthesia is employed.
- An interscalene nerve block is often utilized pre-operatively for post-operative pain management, providing analgesia to the shoulder and arm.
Patient Positioning
For arthroscopic posterior stabilization, the lateral decubitus position is most commonly employed. The beach chair position can also be used, especially if there is a need for easier access to the anterior compartment or if combined anterior and posterior procedures are planned.
-
Lateral Decubitus Position
:
- The patient is positioned with the operative shoulder up.
- A beanbag or specialized positioning device is used to stabilize the torso.
- An axillary roll is placed in the contralateral axilla to protect the brachial plexus and prevent nerve compression.
- The operative arm is suspended in approximately 40-70 degrees of abduction and 15-20 degrees of forward flexion, allowing for traction and full intra-operative range of motion assessment. Traction should be applied gently (typically 10-15 lbs) to distract the joint.
-
The entire upper extremity is sterilely prepped and draped to allow full manipulation of the arm during the procedure.

-
Beach Chair Position
:
- Patient is semi-recumbent, similar to sitting in a beach chair.
- Head is supported to prevent cervical spine hyperextension.
- Care must be taken to maintain cerebral perfusion, monitoring blood pressure closely.
- Arm can be free-draped or held by an assistant.
Imaging Review & Templating
- Thorough review of pre-operative MRI/MRA and CT scans (especially 3D reconstructions) to identify the extent of labral tears, capsular pathology, glenoid retroversion, and bone loss.
- If significant bone loss is anticipated, templating for bone graft size and fixation may be necessary.
Equipment
- Standard arthroscopy tower with high-definition camera, light source, and fluid management system.
- Specific posterior arthroscopic instruments: cannulas, blunt trocars, suture passers, arthroscopic shavers, burrs, suture anchors (bioabsorbable or titanium), knot pushers.
- For open procedures or bone grafting: standard open shoulder instruments, specific drills, screws, and bone graft harvest instruments (if autograft is planned).
Prophylaxis
- Administer peri-operative intravenous antibiotics (e.g., cefazolin) within 60 minutes prior to incision.
- Consider DVT prophylaxis based on patient risk factors.
Detailed Surgical Approach / Technique
The choice between arthroscopic and open stabilization for posterior GH instability depends on the nature and extent of the pathology, particularly the presence of significant bone loss. Arthroscopic techniques are generally preferred for soft tissue lesions, while open procedures or hybrid approaches are reserved for cases with substantial bony defects or severe glenoid retroversion.
1. Arthroscopic Posterior Stabilization (Most Common for Soft Tissue Lesions)
-
Diagnostic Arthroscopy
:
- Standard posterior portal ("soft spot") is typically established first, 1-2 cm medial and 1 cm inferior to the posterolateral corner of the acromion.
- A thorough diagnostic arthroscopy of the entire glenohumeral joint is performed using a 30-degree or 70-degree arthroscope to assess the articular cartilage, labrum (anterior, superior, inferior, posterior), biceps anchor, rotator cuff, and capsular integrity.
- Carefully inspect the posterior labrum for tears (reverse Bankart), periosteal sleeve avulsions (Kim lesions), and capsular laxity. Evaluate the humeral head for a reverse Hill-Sachs lesion and its engagement with the posterior glenoid rim.
-
Accessory Portals
:
- Posterolateral Portal (Neviaser Portal) : Created 2-3 cm lateral to the posterior portal, directly through the posterior deltoid. This portal is often used for suture anchor placement, providing a more perpendicular trajectory to the posterior glenoid.
- Posterior-Inferior Portal : May be useful for instrumentation or anchor placement in more inferior lesions.
- Anterior Portals : Occasionally, an anterior portal (e.g., mid-glenoid or anterosuperior) may be used for visualization or to assist with instrument manipulation.
-
Lesion Preparation
:
- The detached posterior labrum and capsule are identified.
- A motorized shaver or burr is used to debride unstable labral tissue and prepare the glenoid neck bone, creating a bleeding, cancellous bed for healing. This decortication promotes healing of the labrum back to the glenoid.
- The posterior capsule may be released from the underlying glenoid neck to allow for adequate mobilization and tightening.
-
Suture Anchor Placement and Capsulolabral Repair
:
- Suture anchors (bioabsorbable PEEK or titanium) are typically placed along the posterior glenoid rim, from approximately the 5 o'clock to 7 o'clock position for a right shoulder (7 o'clock to 5 o'clock for a left shoulder). The number of anchors varies, usually 2-4, depending on the extent of the tear.
- The anchors are drilled and inserted approximately 2-3 mm from the articular margin, with care taken to avoid articular cartilage damage.
- Suture passers are used to retrieve the sutures and incorporate the posterior labrum and capsule.
- Capsular Shift/Plication : If significant posterior capsular laxity is present, a capsular shift or plication is performed by taking a generous bite of the capsule with the sutures before tying them down. This effectively reduces capsular volume and tightens the posterior restraints. The goal is to restore appropriate capsular tension without unduly restricting motion.
- Sutures are tied extracapsularly, securing the labrum and tightening the posterior capsule against the glenoid rim.
-
Assessment of Stability
:
- After anchor placement and suture tying, the stability of the glenohumeral joint is carefully assessed under arthroscopic visualization and fluoroscopic guidance (if available) through a full range of motion. The goal is to achieve adequate posterior stability without causing impingement or overly restricting internal rotation.
2. Open Posterior Stabilization (For Significant Bone Loss or Failed Arthroscopy)
Open posterior approaches are indicated for cases with substantial posterior glenoid bone loss (>15-20%), large engaging reverse Hill-Sachs lesions, severe glenoid retroversion, or failed arthroscopic stabilization.
-
Surgical Approach
:
- Incision : A curvilinear or straight incision is made over the posterior aspect of the shoulder, centered over the glenoid. The length depends on the required exposure.
- Deltoid Split : The deltoid muscle is split in line with its fibers. Care must be taken to identify and protect the axillary nerve, which typically courses horizontally approximately 5-7 cm distal to the acromial angle.
- Internervous Plane : The approach utilizes the interval between the infraspinatus (innervated by the suprascapular nerve) and the teres minor (innervated by the axillary nerve). The infraspinatus is typically detached from its insertion on the greater tuberosity (often with a small cuff of bone for easier repair) and reflected medially. Alternatively, an intramuscular split of the infraspinatus can be performed for more limited exposure.
- Capsular Incision : The posterior capsule is incised longitudinally to expose the glenohumeral joint.
-
Bone Grafting for Glenoid Bone Loss (Posterior Latarjet or Iliac Crest Autograft)
:
- For significant glenoid bone loss, augmentation of the posterior glenoid rim is necessary.
- Posterior Latarjet Procedure (Rarely performed) : Transfer of the coracoid process (or a portion of it) with its attached conjoined tendon and pectoralis minor to the posterior glenoid rim. This provides a bony block and a sling effect from the conjoined tendon, similar to its anterior counterpart. Fixation is typically with screws.
- Iliac Crest Autograft/Allograft : A tricortical bone graft harvested from the iliac crest (or structural allograft) is shaped and fixed to the posterior glenoid neck using screws, effectively extending the posterior glenoid rim.
-
Addressing Reverse Hill-Sachs Lesion (Remplissage)
:
- For engaging reverse Hill-Sachs lesions (often those occupying >25% of the humeral head articular surface), a remplissage procedure (French for "to fill in") can be performed. This involves tenodesing the infraspinatus tendon and posterior capsule into the humeral head defect using suture anchors. This effectively fills the defect, preventing it from engaging the posterior glenoid rim during internal rotation and adduction. It can be performed arthroscopically or open.
- For very large, displaced, or arthritic reverse Hill-Sachs lesions, osteochondral allograft or even prosthetic replacement may be considered.
- Capsulorrhaphy : The posterior capsule is meticulously repaired and tightened to reduce joint volume and prevent posterior translation. This may involve a T-plasty closure or overlapping sutures.
- Closure : The infraspinatus tendon is repaired back to its insertion. The deltoid is repaired, and skin closure is performed in layers.
Complications & Management
While shoulder stabilization surgery for posterior GH instability generally yields good results, specific complications can occur. Awareness and timely management are crucial for optimal patient outcomes.
| Complication | Incidence | Management / Salvage Strategy Posterior Deltoid-Splitting Approach for Posterior Glenoid Osteoplasty :**
- Incision : A straight skin incision is made from the posterior acromial angle extending inferomedially towards the posterior axillary fold.
- Superficial Dissection : The subcutaneous tissue is incised, and cutaneous nerves identified and protected. The deep fascia overlying the deltoid muscle is incised.
- Deltoid Split : The fibers of the posterior deltoid are carefully split. This is a critical step. The split must remain parallel to the muscle fibers. The axillary nerve crosses the posterior shoulder approximately 5-7 cm inferior to the acromial angle, often closer than anticipated. It must be identified or carefully protected by limiting the distal extent of the deltoid split. The split should not extend more than 5 cm distally from the acromion to avoid injury to the axillary nerve.
- Infraspinatus & Teres Minor Identification : Beneath the deltoid, the infraspinatus and teres minor muscles are identified. The interval between them is the internervous plane.
-
Exposure of Joint Capsule
: The infraspinatus can be mobilized and reflected medially either by:
- Infraspinatus Release : Detaching the infraspinatus tendon from its insertion on the greater tuberosity (with a small bone cuff if possible for reattachment). This provides excellent exposure.
- Infraspinatus Split : An intramuscular split of the infraspinatus can be performed for more limited exposure, protecting the suprascapular nerve which innervates the infraspinatus medially.
- Capsular Incision : Once the posterior capsule is exposed, a T-shaped or inverted T-shaped incision is typically made. This allows for thorough evaluation of the posterior labrum, glenoid rim, and humeral head.
-
Lesion Addressing
:
- Posterior Labral Repair/Capsulorrhaphy : Similar to arthroscopic, the labrum is reattached and the capsule tightened, but under direct visualization. Anchors are placed into the glenoid.
- Glenoid Osteoplasty/Bone Grafting : For significant posterior glenoid bone loss or retroversion, an osteotomy of the glenoid can be performed to reorient it, or a bone block (autograft from iliac crest, or allograft) can be rigidly fixed to the posterior glenoid to reconstruct the articular arc.
- Remplissage : If an open approach is chosen and a humeral head defect is present, the infraspinatus and posterior capsule can be directly tenodesed into the defect.
-
Closure
: The posterior capsule is meticulously closed and imbricated to achieve appropriate tension. The infraspinatus tendon is repaired back to its insertion. The deltoid muscle is repaired, and the superficial layers are closed.
 (This image depicts a posterior shoulder approach, likely open)
(This image depicts a posterior shoulder approach, likely open)
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a critical determinant of surgical success and must be tailored to the specific surgical procedure performed, patient factors, and the surgeon's preference. Strict adherence to a structured, progressive protocol is essential to protect the repair, restore range of motion, and regain strength and function.
Phase I: Protection & Early Motion (Weeks 0-6)
- Goals : Protect the repair, reduce pain/inflammation, prevent stiffness, initiate early passive range of motion.
-
Immobilization
:
- Sling immobilization for 4-6 weeks, typically with the arm in a neutral or slight abduction/external rotation position, avoiding the positions of posterior instability (adduction, internal rotation, flexion).
- Sling removal only for hygiene and exercises.
-
Pain & Edema Management
:
- Cryotherapy, NSAIDs (if not contraindicated), appropriate analgesics.
-
Passive Range of Motion (PROM)
:
- Initiated early, usually within the first week, under the guidance of a physical therapist.
- Focus on protected arcs of motion , avoiding stress on the posterior repair.
- Avoid combined adduction, internal rotation, and flexion.
- PROM for flexion to 90-120 degrees, abduction to 90 degrees, and neutral rotation. External rotation PROM is typically limited initially to avoid anterior capsular stretch.
- No internal rotation past neutral for the first 4-6 weeks.
-
Scapular Stabilization
:
- Gentle isometric scapular exercises (e.g., scapular squeezes, protraction/retraction in supine).
-
Elbow, Wrist, Hand Exercises
:
- Active ROM exercises to prevent stiffness and maintain circulation.
Phase II: Gradual Strengthening & Increased Motion (Weeks 6-12)
- Goals : Progress ROM, initiate active control, begin strengthening.
- Sling Discontinuation : Gradual weaning from the sling, typically by week 6, as tolerated.
-
Active-Assistive Range of Motion (AAROM) & Active Range of Motion (AROM)
:
- Progress from PROM to AAROM and then AROM, gradually increasing the range in all planes, still respecting pain and avoiding provocative positions.
- Gradually increase internal rotation with caution.
-
Isometric Strengthening
:
- Initiate gentle isometric exercises for the rotator cuff (infraspinatus, teres minor, subscapularis) and deltoid, always in protected positions.
-
Scapular Strengthening
:
- Progressive exercises for scapular retractors and protractors (e.g., rows, push-ups against a wall).
-
Proprioceptive Exercises
:
- Wall slides, rhythmic stabilization exercises with therapist assistance.
Phase III: Advanced Strengthening & Return to Activity (Weeks 12-24+)
- Goals : Restore full ROM, maximize strength, power, endurance, and neuromuscular control; prepare for return to sport/activity.
-
Progressive Resistance Strengthening
:
- Advance to isotonic and isokinetic exercises using resistance bands, dumbbells, and weight machines.
- Focus on rotator cuff strength (especially external rotators: infraspinatus, teres minor), deltoid, and periscapular musculature.
- Eccentric strengthening of the posterior rotator cuff.
-
Sport-Specific Training
:
- For athletes, incorporate exercises mimicking the demands of their sport (e.g., throwing mechanics, overhead movements, contact drills).
-
Plyometric Training
:
- Initiate plyometric exercises for power generation and dynamic stability, only after adequate strength and control are achieved.
-
Return to Activity
:
-
Criteria for return to unrestricted activity or sport typically include:
- Full, pain-free ROM.
- Strength symmetry >90% compared to the contralateral side (especially external rotators).
- Absence of apprehension or instability.
- Good neuromuscular control and confidence.
- Return to contact sports is typically delayed for 6-9 months post-surgery.
-
Criteria for return to unrestricted activity or sport typically include:
Summary of Key Literature / Guidelines
Posterior glenohumeral instability, though less common, has garnered increasing attention in orthopedic literature due to its diagnostic challenges and potential for significant morbidity. Key themes in recent research and clinical guidelines include:
-
Enhanced Imaging for Diagnosis : The critical role of advanced imaging, particularly MR Arthrography (MRA) and 3D Computed Tomography (CT) , cannot be overstated. MRA provides superior visualization of soft tissue lesions such as subtle posterior labral tears (e.g., Kim lesions) and capsular pathology, which are often missed on standard MRI. 3D CT is indispensable for quantifying glenoid bone loss and characterizing reverse Hill-Sachs lesions, informing surgical strategy. The concept of an "engaging" reverse Hill-Sachs lesion, where the defect contacts the posterior glenoid rim during internal rotation and adduction, is a crucial determinant for surgical intervention and the need for humeral head augmentation (e.g., remplissage or osteochondral grafting).
- Reference example : Gerber et al. (1987) elucidated the concept of the engaging Hill-Sachs lesion in anterior instability, which has been extrapolated to the posterior context. Subsequent studies by Provencher et al. and others have emphasized the importance of bony defects in recurrent posterior instability.
-
Biomechanics and Pathoanatomy : Research consistently highlights the importance of the posterior inferior glenohumeral ligament (PIGHL) as the primary static restraint against posterior translation, particularly in adduction and internal rotation. Studies on glenoid retroversion, both congenital and acquired, demonstrate its contribution to reduced posterior glenoid stability and a propensity for posterior subluxation.
- Reference example : Harryman et al. (1992) extensively studied glenohumeral ligaments and their role in stability. Newer cadaveric studies continue to refine our understanding of load-bearing structures in posterior instability.
-
Arthroscopic vs. Open Approaches :
- Arthroscopic stabilization is generally preferred for isolated posterior labral tears (reverse Bankart lesions) and capsular laxity without significant bone loss. Outcomes are largely comparable to anterior stabilization for similar soft tissue pathologies. The focus is on robust labral reattachment and capsular plication, with an emphasis on recreating the posterior bumper and tightening the posterior IGHL complex.
-
Open techniques or hybrid approaches
are indicated for complex cases involving substantial bony defects, such as significant glenoid bone loss (>15-20% of the glenoid diameter) or large, engaging reverse Hill-Sachs lesions.
- For glenoid bone loss, the concept of posterior glenoid augmentation with autogenous bone graft (e.g., iliac crest) or allograft is well-established to restore the glenoid arc and prevent recurrent engagement. While less common, the posterior Latarjet procedure (transfer of the coracoid to the posterior glenoid) has been described, mirroring its anterior counterpart, but carries greater technical complexity and risk.
- For engaging reverse Hill-Sachs lesions, the arthroscopic remplissage procedure (infraspinatus tenodesis into the humeral head defect) has gained traction as an effective adjunct to posterior labral repair, mitigating recurrent engagement. Long-term follow-up studies are maturing, showing promising results regarding stability without significant loss of external rotation.
- Reference example : The American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines for shoulder instability emphasize individualized treatment based on patient age, activity level, and the presence of bony defects. Recent reviews by Provencher et al. (2014, 2018) provide comprehensive overviews of current surgical strategies for posterior instability.
-
Rehabilitation : Adherence to a structured, progressive rehabilitation protocol is crucial. Early emphasis is placed on protecting the repair by avoiding positions of combined adduction, internal rotation, and flexion, followed by a gradual progression of range of motion and strengthening. Specific attention to strengthening the posterior rotator cuff (infraspinatus and teres minor) and scapular stabilizers is paramount for restoring dynamic stability.
-
Outcomes & Recurrence : Recurrence rates for posterior instability surgery are generally lower than for anterior instability but can range from 5-15% depending on the study population, surgical technique, and extent of initial pathology. Factors associated with higher recurrence include younger age, participation in collision sports, presence of significant unrepaired bone loss, and inadequate capsular tensioning.
In conclusion, managing posterior GH instability requires a meticulous diagnostic workup, a comprehensive understanding of complex pathoanatomy, and a tailored surgical approach. The evolution of arthroscopic techniques and the refined management of bony defects have significantly improved outcomes for this challenging condition. Continued research focusing on long-term outcomes, optimal bone graft choices, and precise indications for various augmentation procedures will further refine treatment algorithms.
