Patient Presentation & History
A 28-year-old right-hand dominant male presented to the emergency department following a high-energy fall during a rugby match. The mechanism of injury involved direct impact to the posterior aspect of the shoulder while the arm was abducted and externally rotated, resulting in a forceful anterior dislocation. He reported immediate, severe pain in the left shoulder, complete loss of function, and a visible deformity. This was his third episode of anterior glenohumeral dislocation on the left side within 18 months, with the previous two occurring during sports activities and successfully reduced in the emergency department. He denied any significant pre-existing shoulder pathology, systemic diseases, or bleeding diatheses. His medical history was otherwise unremarkable, with no known allergies and no regular medications. Social history included active participation in competitive contact sports and no tobacco or illicit drug use.
Clinical Examination
Upon initial assessment, the patient was in acute distress, cradling his left arm.
*
Inspection:
Marked deformity of the left shoulder was evident, characterized by a flattened deltoid contour anteriorly and laterally, with a prominent acromion. There was a palpable sulcus beneath the acromion anteriorly, and the humeral head was palpable anteriorly beneath the coracoid process, consistent with an anterior glenohumeral dislocation. No open wounds or ecchymoses were noted initially, though mild swelling was present.
*
Palpation:
Tenderness was localized globally around the shoulder joint, with exquisite pain upon any attempted movement. The humeral head was distinctly palpable in the anterior subcoracoid position. Crepitus was not elicited.
*
Range of Motion (ROM):
Actively, the patient had zero range of motion due to pain. Passively, any attempt to move the glenohumeral joint was met with significant resistance and severe pain, confirming a locked dislocation.
*
Neurological Assessment:
A thorough neurovascular examination was performed prior to any reduction attempts. Axillary nerve function was assessed by sensation over the regimental badge area and deltoid contraction (if possible), which was diminished but not absent. Musculocutaneous, median, ulnar, radial, and suprascapular nerve functions were intact distally.
*
Vascular Assessment:
Distal pulses (radial, ulnar) were strong and symmetric bilaterally. Capillary refill was brisk in all digits. No pallor or paresthesias were present in the hand or forearm.
Given the history of recurrent dislocations and the mechanism of injury, a high index of suspicion for associated bony and soft tissue lesions, including a critical Hill-Sachs lesion and anterior glenoid bone loss, was established.
Imaging & Diagnostics
Initial imaging in the emergency department confirmed an anterior glenohumeral dislocation and allowed for assessment of associated bony pathology.
-
X-rays:
A standard shoulder series including AP, Y-scapular, and axillary views was obtained.
- The AP view demonstrated the humeral head dislocated inferior and medial to the glenoid, lying beneath the coracoid.
- The Y-scapular view unequivocally confirmed the anterior displacement of the humeral head relative to the glenoid and coracoid.
-
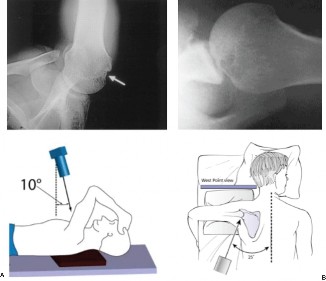
The
axillary view
(or a Velpeau view if an axillary view was too painful or difficult to obtain) provided crucial information regarding the presence and extent of bony defects.
Initial AP radiograph demonstrating an anterior glenohumeral dislocation of the left shoulder.
Following successful closed reduction under conscious sedation, post-reduction X-rays were obtained to confirm concentric reduction and re-evaluate for occult fractures or persistent bony defects. A large, impression fracture on the posterosuperior aspect of the humeral head – a Hill-Sachs lesion – was identified on the post-reduction internal rotation AP and axillary views. There was also suspicion of an anterior glenoid rim fracture (osseous Bankart lesion).
-
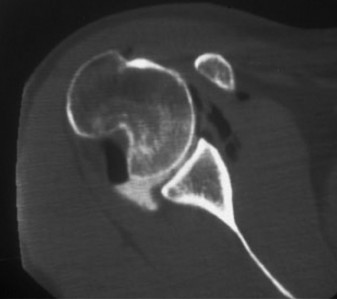
CT Scan: Due to the recurrent nature of the dislocations, the presence of a Hill-Sachs lesion on X-ray, and suspicion of glenoid bone loss, a computed tomography (CT) scan with 3D reconstructions was indicated and performed.
- The CT scan was critical for accurate quantification of glenoid bone loss and precise characterization of the Hill-Sachs lesion.
- It revealed a significant anterior-inferior glenoid bone defect, estimated to be approximately 20-25% of the inferior glenoid diameter, consistent with an osseous Bankart lesion.
-
Crucially, the CT scan also confirmed a large Hill-Sachs lesion involving the posterosuperior humeral head. Measurements indicated the lesion was approximately 2.5 cm in width and 0.8 cm in depth. The 3D reconstruction facilitated assessment of its engaging potential, demonstrating that in typical positions of apprehension (abduction and external rotation), the Hill-Sachs defect engaged with the anterior glenoid rim, significantly contributing to the instability.

Axial CT image demonstrating a significant Hill-Sachs lesion on the humeral head (arrow) and an anterior glenoid bone defect.
-
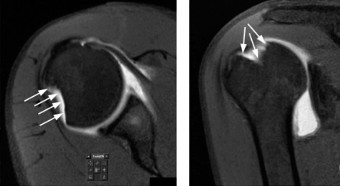
MRI Scan: While CT was paramount for bony assessment, an MRI was obtained to evaluate the extent of soft tissue injuries, including the labral complex, rotator cuff, and capsuloligamentous structures.
- MRI confirmed a full-thickness tear of the anterior-inferior labrum extending from 2 to 6 o'clock (classic Bankart lesion), contiguous with the osseous Bankart lesion.
- There was evidence of extensive capsular stretching and redundant inferior glenohumeral ligament complex.
- No rotator cuff tears were identified, and the biceps tendon was intact.
- The MRI further characterized the Hill-Sachs lesion, confirming its location and depth, and importantly, its relationship with the posterior rotator cuff tendons, which were intact.
Based on imaging, the patient presented with recurrent anterior glenohumeral instability, significant anterior glenoid bone loss (>20%), and an engaging Hill-Sachs lesion, indicating a "bipolar bone loss" scenario which significantly increases the risk of recurrent dislocation after isolated soft tissue repair.
Differential Diagnosis
Given the presentation of shoulder pain and instability following trauma, several differential diagnoses must be considered, particularly in the acute phase prior to definitive imaging.
| Condition | Key Clinical Features | Distinctive Imaging Findings | Management Implications |
|---|---|---|---|
| Anterior Glenohumeral Dislocation (Acute) | Acute severe pain, loss of function, visible deformity (flattened deltoid, palpable humeral head anteriorly), apprehension test positive post-reduction. Recurrent in this case. | Humeral head displaced anteriorly on AP, Y-scapular, and axillary X-rays. CT/MRI confirm Hill-Sachs, Bankart (osseous/soft tissue), capsular laxity. | Urgent closed reduction. Immobilization. Thorough workup for associated injuries (Hill-Sachs, glenoid bone loss, rotator cuff, nerve injury). High risk of recurrence with significant bone loss, often requiring surgical stabilization. This is the primary diagnosis. |
| Posterior Glenohumeral Dislocation | Less common, often associated with seizures or electrocution. Arm held in internal rotation and adduction. Flattened anterior deltoid, prominent coracoid. Restricted external rotation. | AP X-ray may appear normal ("lightbulb sign" of humeral head). Axillary and Y-scapular views crucial. Reverse Hill-Sachs (impression fracture on anterior humeral head) and reverse Bankart (posterior glenoid rim fracture) on CT/MRI. | Urgent closed reduction. High risk of missing diagnosis on initial X-rays. Watch for posterior labral tears or reverse Hill-Sachs. Surgical fixation often required for recurrent cases or large bony lesions. |
| Rotator Cuff Tear (Isolated) | Acute pain, weakness with specific movements (abduction, external rotation). No gross deformity if no dislocation. May occur with trauma or degeneration. | MRI shows full-thickness or partial-thickness tear of supraspinatus, infraspinatus, subscapularis, or teres minor tendons. No glenohumeral dislocation. | Non-operative management with physiotherapy for partial tears. Surgical repair for symptomatic full-thickness tears, especially in active patients. Rehabilitation focused on strength and ROM without concern for instability. |
| Proximal Humerus Fracture (Non-dislocated) | Acute pain, swelling, ecchymosis, crepitus, deformity localized to proximal humerus. Variable ROM depending on fracture type. Shoulder joint may appear intact. | X-rays clearly show fracture lines in surgical neck, anatomical neck, greater tuberosity, or lesser tuberosity without glenohumeral dislocation. CT for comminution, articular involvement. | Management depends on fracture pattern (Neer classification). Non-operative for stable, minimally displaced fractures. ORIF or arthroplasty for displaced, comminuted, or articular fractures. Focus on fracture healing and alignment, not primarily instability. |
| Acromioclavicular (AC) Joint Separation | Localized pain and tenderness over AC joint. Deformity with "step-off" at superior aspect of shoulder. Pain with cross-body adduction. | AP Zanca view or weight-bearing views show increased coracoclavicular distance and/or AC joint widening. May be associated with coracoid process fracture in severe cases. | Non-operative for Type I-II separations. Surgical fixation for Type III-VI (controversial for Type III) to restore stability and alignment. Focus on clavicular reduction and stabilization rather than glenohumeral joint. |
| Biceps Tendon Rupture (Proximal) | Acute "pop" sensation, sudden pain, ecchymosis, visible "Popeye" muscle deformity (distal migration of muscle belly). Weakness in elbow flexion/supination. | MRI demonstrates rupture of long head of biceps tendon at bicipital groove or labral attachment (SLAP lesion). No acute glenohumeral instability. | Non-operative for older, less active patients. Surgical tenodesis or tenotomy for younger, active individuals or those with cosmetic concerns. Primary focus on pain and strength, not joint instability. |
Surgical Decision Making & Classification
The decision for operative intervention in this patient was multifaceted and driven by several critical factors:
- Recurrent Instability: This was the patient's third episode of dislocation, indicating inherent instability despite conservative management (immobilization and physical therapy after previous reductions).
- Patient Demographics and Activity Level: A young, active individual involved in competitive contact sports has a high demand on shoulder stability and a significantly increased risk of re-dislocation after non-operative treatment or isolated soft tissue repair alone.
-
Bony Defects ("Bipolar Bone Loss"):
- Anterior Glenoid Bone Loss: The CT scan demonstrated an osseous Bankart lesion resulting in 20-25% loss of the inferior glenoid diameter. Glenoid bone loss is a major predictor of recurrence after arthroscopic Bankart repair. A loss exceeding 20% often warrants bony augmentation.
- Engaging Hill-Sachs Lesion: The Hill-Sachs lesion, approximately 2.5 cm wide and 0.8 cm deep, was identified as engaging with the anterior glenoid rim in positions of apprehension. The "engaging" nature is crucial; a non-engaging Hill-Sachs may not require direct management, but an engaging lesion dramatically increases the risk of re-dislocation.
- Glenoid Track Concept: The combination of significant glenoid bone loss and an engaging Hill-Sachs lesion falls into the "off-track" category according to the glenoid track concept, signifying a high risk of recurrent instability that is unlikely to be adequately addressed by isolated soft tissue repair. The glenoid track refers to the contact zone between the posterior-superior humeral head and the anterior glenoid when the arm is abducted and externally rotated. If the Hill-Sachs lesion extends medial to the glenoid track (i.e., "off-track"), it is considered an engaging lesion.
Classification Systems Guiding Decision-Making:
- Instability Severity Index Score (ISIS Score by Balg and Boileau): This score considers factors like patient age (<20 years), sport (contact/overhead), hyperlaxity, engaging Hill-Sachs, and glenoid bone loss (>25%). Our patient scores points for age, sport, engaging Hill-Sachs, and glenoid bone loss, placing him in a high-risk category for recurrence after arthroscopic Bankart repair, strongly favoring bony augmentation.
- Glenoid Track Classification: As noted, the combination of >20% glenoid bone loss and an engaging Hill-Sachs puts the lesion "off-track," requiring bony augmentation of the glenoid and/or an arthroscopic Remplissage to address the Hill-Sachs.
- Hill-Sachs Lesion Classification (e.g., based on size, depth, and engaging potential): While formal classification systems for Hill-Sachs are less commonly used for surgical decision-making than the glenoid track concept, the size and depth of this lesion (2.5 cm wide, 0.8 cm deep) are significant, further supporting the need for direct management of the defect.
Based on these considerations, an isolated arthroscopic Bankart repair was deemed insufficient due to the high risk of failure. A combined approach was indicated:
1.
Anterior Glenoid Augmentation:
To address the significant anterior glenoid bone loss, restoring the anterior stability of the glenoid.
2.
Addressing the Engaging Hill-Sachs Lesion:
To prevent the humeral head defect from engaging the augmented or repaired glenoid rim, thereby preventing recurrent dislocations.
The chosen surgical strategy was an arthroscopic Latarjet procedure for glenoid augmentation combined with an arthroscopic Remplissage for the engaging Hill-Sachs lesion. This approach provides robust bony and soft tissue stability, particularly important for a young, active athlete.
Surgical Technique / Intervention
The patient underwent a combined arthroscopic Latarjet and Remplissage procedure under general anesthesia.
Patient Positioning and Setup
- The patient was positioned in a "beach-chair" position on a standard operating table, allowing for easy manipulation of the arm and access to both anterior and posterior aspects of the shoulder.
- The ipsilateral arm was prepped and draped free to allow for full range of motion.
- The use of a sterile arm holder or traction tower was considered but often avoided for Latarjet to allow more dynamic arm positioning.
- Standard diagnostic arthroscopy was performed first to confirm all pathologies.
Diagnostic Arthroscopy
- Posterior portal entry for initial diagnostic arthroscopy.
- Confirmation of the significant anterior-inferior labral tear and osseous Bankart lesion.
- Visualization and probing of the Hill-Sachs lesion on the posterosuperior humeral head to assess its size, depth, and engaging potential.
- Evaluation of the rotator cuff and biceps tendon, which were found to be intact.
- Assessment of capsular laxity.
Arthroscopic Latarjet Procedure
The arthroscopic Latarjet procedure involved the transfer of the coracoid process, with its attached conjoint tendon, to the anterior-inferior aspect of the glenoid.
-
Portal Placement:
- Posterior Portal: For diagnostic and posterior viewing.
- Anterolateral Portal (Working): Main working portal for glenoid preparation.
- Anterior Inferior Portal: For dissection and placement of guidewires/screws for the coracoid transfer.
- Anterior-Superior Portal: For viewing during coracoid osteotomy and preparation.
-
Coracoid Dissection and Osteotomy:
- An initial superficial incision was made to identify the deltopectoral interval.
- Through the anterior-superior portal, the coracoid process was identified. The pectoralis minor insertion was released.
- A subscapularis split was carefully created to access the anterior glenoid neck.
- Using an arthroscopic burr or oscillating saw, a precise osteotomy of the coracoid was performed at its base, ensuring the conjoint tendon remained attached.
- The undersurface of the coracoid was decorticated to promote bony union.
-
Glenoid Preparation:
- The anterior-inferior glenoid rim was debrided, and the remaining Bankart fragment was removed.
- The anterior glenoid neck was decorticated to provide a bleeding bone bed for coracoid integration.
- A guidewire was drilled from anterior to posterior through the glenoid neck, creating pilot holes for screw placement.
-
Coracoid Transfer and Fixation:
- The osteotomized coracoid process, maintaining its soft tissue attachments (conjoint tendon), was carefully translated through the subscapularis split and positioned flush against the prepared anterior glenoid neck.
- The pre-drilled guidewires were used to guide two 3.5 mm cortical screws (partially threaded, cannulated) for compression and stabilization of the coracoid graft to the glenoid.
- The screws were fully tightened, ensuring firm fixation of the coracoid to the glenoid, providing a bony buttress and an additional dynamic sling effect from the conjoint tendon.
-
The capsule and remaining labral tissue were then repaired or plicated over the coracoid graft, creating an anatomical reconstruction and further stabilizing the joint.
Arthroscopic view during the Latarjet procedure, showing the coracoid graft secured to the anterior glenoid with screws.
Arthroscopic Remplissage Procedure
Following the Latarjet, attention was turned to the Hill-Sachs lesion to address its engaging potential.
- Portal Placement: Typically a separate posterior-inferior accessory portal is used for the Remplissage, or the standard posterior portal can be adjusted. An anterior-superior portal is used for viewing.
- Lesion Identification: The Hill-Sachs lesion on the posterosuperior humeral head was clearly visualized through the anterior portal.
-
Capsulotenodesis:
- The posterior capsule and the infraspinatus tendon were identified adjacent to the Hill-Sachs defect.
- Through the posterior working portal, the lesion bed was gently debrided to expose cancellous bone.
- One or two suture anchors (e.g., 2.9 mm biocomposite or PEEK anchors) were placed into the cancellous bone within the Hill-Sachs defect.
- The sutures from these anchors were then passed through the posterior capsule and the infraspinatus tendon, capturing them firmly.
- Upon tying the sutures, the posterior capsule and infraspinatus tendon were pulled into the Hill-Sachs defect, effectively "filling" the lesion. This procedure converts the engaging defect into a non-engaging one and also provides additional posterior capsular plication, limiting excessive external rotation.
Closure
- All portals were closed with subcutaneous sutures and skin adhesive.
- A sterile dressing was applied, and the arm was placed in a shoulder immobilizer sling with a neutral rotation pillow.
Post-Operative Protocol & Rehabilitation
The post-operative protocol for a combined Latarjet and Remplissage procedure is structured and progressive, focusing on protecting the repairs while gradually restoring motion and strength.
Phase 1: Immobilization & Protection (Weeks 0-4)
- Immobilization: Arm maintained in a shoulder immobilizer sling with a neutral rotation pillow continuously, except for hygiene and specific exercises.
- Goals: Protect graft healing, prevent uncontrolled external rotation, minimize pain and swelling.
-
Activities:
- Elbow, wrist, and hand active range of motion (AROM) exercises (e.g., flexion/extension, pronation/supination, grip strengthening).
- Pendulum exercises for shoulder (passive).
- Scapular stabilization exercises (e.g., scapular squeezes) without active glenohumeral motion.
- Ice application for pain and swelling.
-
Restrictions:
- NO active shoulder flexion, abduction, or external rotation.
- NO passive shoulder external rotation beyond neutral.
- NO lifting, pushing, or pulling with the affected arm.
- Avoid reaching behind the back.
Phase 2: Early Motion & Gentle Strengthening (Weeks 4-12)
- Goals: Gradual restoration of passive and active-assisted range of motion, initiation of isometric strengthening.
-
Activities:
-
Week 4-6:
- Initiate passive ROM (PROM) for flexion (up to 90 degrees), abduction (up to 90 degrees), and internal rotation (hand to belly).
- Gentle external rotation PROM to tolerance (typically not exceeding 30 degrees from neutral initially).
- Isometric rotator cuff strengthening (submaximal, in neutral rotation).
- Continuation of scapular stabilization exercises.
-
Week 6-12:
- Progress to active-assisted ROM (AAROM) and then AROM as tolerated, gradually increasing flexion and abduction.
- Continue to limit external rotation, gradually increasing to 45-60 degrees by week 12, protecting the Remplissage.
- Introduce light resistance exercises for rotator cuff and deltoid, always within pain-free limits.
- Proprioceptive exercises (e.g., wall slides, rhythmic stabilization).
-
Week 4-6:
-
Restrictions:
- Avoid forceful external rotation, especially with abduction.
- No overhead activities or heavy lifting.
- No sudden movements or ballistic activities.
Phase 3: Intermediate Strengthening & Advanced Motion (Weeks 12-24)
- Goals: Restore full non-painful range of motion, significantly increase strength and endurance, prepare for sport-specific activities.
-
Activities:
- Progressive strengthening exercises for all shoulder girdle muscles (rotator cuff, deltoid, scapular stabilizers) with increasing resistance (bands, light weights).
- Continue to increase ROM, aiming for near-normal by 6 months, with specific attention to external rotation limits from the Remplissage.
- Initiate light plyometric and sport-specific drills (e.g., throwing mechanics, simulated movements) if appropriate for the patient's sport.
- Advanced proprioception and neuromuscular control exercises.
-
Restrictions:
- Avoid contact sports or high-impact activities.
- Continue to be cautious with extreme abduction/external rotation combinations.
Phase 4: Return to Sport / Activity (Months 6-12+)
- Goals: Full return to previous activity level, including contact sports, with optimal strength, endurance, and stability.
-
Activities:
- Gradual progression to full sport-specific training.
- High-intensity plyometric and power exercises.
- Continued strengthening and maintenance program.
- Dynamic stability drills.
-
Criteria for Return to Sport:
- Full, pain-free range of motion (within Remplissage limitations).
- Strength at least 90% of the contralateral limb (isokinetic testing often recommended).
- No apprehension with sport-specific movements.
- Clearance from the orthopedic surgeon and physical therapist.
- Note: Return to contact sports typically not before 6-9 months, and often up to 12 months, depending on individual progress and sport demands. The Remplissage restricts some external rotation, which may alter throwing mechanics slightly for overhead athletes, but often provides the necessary stability for contact sports.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls
- Comprehensive Pre-operative Assessment: Never underestimate the importance of meticulous clinical and imaging assessment. The combination of X-rays, CT (for bone loss), and MRI (for soft tissue) is crucial for accurate diagnosis and surgical planning, especially in recurrent instability.
- Identify Bipolar Bone Loss: Always suspect and quantify both glenoid bone loss (osseous Bankart) and humeral head impression defects (Hill-Sachs). Use the glenoid track concept to determine if the Hill-Sachs is "engaging" or "off-track," as this directly dictates the need for bony augmentation or Remplissage.
- ISIS Score Application: Utilize prognostic scoring systems like the Instability Severity Index Score (ISIS) to stratify patient risk for recurrence and guide the choice between soft tissue repair (Bankart) and bony augmentation (Latarjet). High ISIS scores (>3-4) typically warrant bony procedures.
-
Latarjet Principles:
- Conjoint Tendon Integrity: Ensure the conjoint tendon remains attached to the coracoid process, as it contributes a dynamic sling effect.
- Coracoid Positioning: The coracoid graft should be flush with the glenoid face (medialized) and inferior to the equator of the glenoid. Proper positioning prevents anterior impingement and ensures optimal buttressing.
- Rigid Fixation: Two strong screws are essential for stable fixation, promoting timely bony union.
- Remplissage for Engaging Lesions: Arthroscopic Remplissage (capsulotenodesis of the posterior capsule and infraspinatus tendon into the Hill-Sachs defect) is an effective adjunct for engaging Hill-Sachs lesions. It converts the lesion into a non-engaging one and limits excessive external rotation.
- Rehabilitation Tailoring: Recognize that a combined Latarjet and Remplissage has specific rehabilitation considerations. The Remplissage will inherently limit terminal external rotation, which is protective but needs to be managed in rehab expectations. Protect the Latarjet graft by limiting early active elevation and excessive force.
- Patient Expectations: Clearly discuss the potential for slightly altered range of motion (especially external rotation) post-Remplissage and the necessary prolonged rehabilitation period with the patient.
Pitfalls
- Underestimating Bone Loss: Failing to accurately quantify glenoid bone loss or overlooking a critical Hill-Sachs lesion is a leading cause of recurrent instability after primary arthroscopic repair. Plain X-rays are often insufficient.
- Isolated Soft Tissue Repair for Bipolar Bone Loss: Performing only an arthroscopic Bankart repair in the presence of significant glenoid bone loss (>20%) and/or an engaging Hill-Sachs lesion leads to unacceptably high re-dislocation rates. This is a common exam scenario for identifying a flawed surgical plan.
-
Neurovascular Injury during Latarjet:
- Axillary Nerve: Susceptible to injury during dissection of the anterior capsule and inferior glenoid neck. Careful identification and protection are paramount.
- Musculocutaneous Nerve: Can be damaged if the conjoint tendon is dissected too extensively or if instruments are advanced too far medially during coracoid osteotomy.
- Vessels: Subscapular artery/vein can be at risk during the subscapularis split.
-
Poor Coracoid Placement/Fixation (Latarjet):
- Lateralization: If the coracoid is placed too laterally, it may impinge, restrict motion, or fail to provide adequate buttressing.
- Malrotation: Incorrect rotation can lead to improper contact with the glenoid.
- Insufficient Fixation: Inadequate or poorly placed screws can lead to non-union or graft failure.
- Over-Tensioning Remplissage: Aggressive capsulotenodesis during Remplissage can significantly limit external rotation and potentially cause stiffness or functional impairment. The goal is to fill the defect, not to rigidly restrict all external rotation.
- Premature Return to Activity: Allowing the patient to return to high-demand activities, especially contact sports, too early can compromise healing and lead to re-injury. Adherence to a structured, phased rehabilitation protocol is critical.
- Inadequate Post-operative Imaging: Not confirming adequate graft position and healing (Latarjet) or assessing for persistent engaging lesion post-Remplissage can miss early signs of failure. A post-op CT may be warranted to confirm graft integration.
Clinical & Radiographic Imaging