Introduction & Epidemiology
Tears involving the infraspinatus and teres minor, while less common in isolation than supraspinatus tears, represent a critical component of posterior rotator cuff pathology. These muscles are indispensable for glenohumeral external rotation and posteriordynamic stability, and their dysfunction significantly impairs shoulder kinematics and overall upper extremity function. As academic orthopedic surgeons, it is imperative to understand the nuances of these specific tears, given their distinct anatomical considerations, biomechanical implications, and often challenging reconstructive demands.
Epidemiologically, the vast majority of rotator cuff tears involve the supraspinatus, either in isolation or as part of a multi-tendon tear. Isolated infraspinatus tears are rare, accounting for only a small percentage (e.g., 2-10%) of all rotator cuff pathology. Teres minor tears are even less frequent as an isolated entity, typically occurring in the setting of massive posterosuperior rotator cuff tears, particularly those involving the infraspinatus. When present, infraspinatus and teres minor tears are often degenerative in origin, associated with chronic impingement, age-related tendon degeneration, or overuse. Traumatic tears, while less common, can occur with forceful external rotation against resistance or direct posterior impact, especially in younger, active individuals. These traumatic tears warrant timely evaluation and intervention due to the potential for retraction and fatty infiltration if treatment is delayed. The recognition and understanding of these specific posterior cuff tears are vital for optimizing diagnostic accuracy, surgical planning, and post-operative outcomes.
Surgical Anatomy & Biomechanics
Anatomy
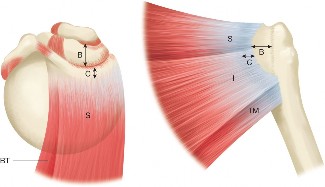
The infraspinatus and teres minor muscles constitute the posterior components of the rotator cuff, playing crucial roles in glenohumeral stability and external rotation.
-
Infraspinatus:
- Origin: The infraspinous fossa of the scapula. This broad origin extends from the base of the scapular spine inferiorly to the posterior glenoid rim laterally.
- Insertion: The middle facet of the greater tuberosity of the humerus. The tendon is broad and contributes significantly to the posterior cuff footprint.
- Innervation: The suprascapular nerve (C5, C6), a branch of the upper trunk of the brachial plexus. The nerve courses through the spinoglenoid notch to supply the infraspinatus. Injury to the suprascapular nerve, particularly at the spinoglenoid notch, can lead to isolated infraspinatus atrophy and weakness, mimicking a tear.
- Vascular Supply: Primarily from the suprascapular artery and circumflex scapular artery.
- Function: Primary external rotator of the humerus, assists in stabilizing the humeral head against the glenoid.
-
Teres Minor:
- Origin: The lateral border of the scapula, specifically the upper two-thirds of the posterior aspect of the lateral border.
- Insertion: The inferior facet of the greater tuberosity of the humerus, immediately inferior to the infraspinatus insertion.
- Innervation: The posterior division of the axillary nerve (C5, C6). The axillary nerve, after exiting the quadrangular space, wraps around the surgical neck of the humerus and provides branches to the teres minor.
- Vascular Supply: Circumflex scapular artery and posterior circumflex humeral artery.
- Function: Assists the infraspinatus in external rotation, and is a key stabilizer of the humeral head, particularly preventing posterior-inferior subluxation. It is often referred to as the "sister muscle" to the deltoid due to its shared innervation from the axillary nerve.
The anatomical relationship between these tendons and the surrounding structures is critical during surgical repair. The infraspinatus tendon often blends with the posterior capsule, and tears can extend into the capsular complex. The critical zone for posterior cuff repair lies in proximity to the articular cartilage of the humeral head and the neurovascular structures. The interval between the infraspinatus and teres minor, though less commonly discussed as an interval for approach, must be respected to avoid iatrogenic injury.
The posterior greater tuberosity is the primary footprint for these tendons. Understanding the specific facets—supraspinatus to the superior facet, infraspinatus to the middle facet, and teres minor to the inferior facet—is paramount for anatomical reduction and fixation.
Biomechanics
The infraspinatus and teres minor are integral to the dynamic stability and coordinated movement of the glenohumeral joint.
*
External Rotation:
Together, they are the primary external rotators of the shoulder. A deficiency in either, particularly the infraspinatus, leads to significant weakness in external rotation, manifesting as an external rotation lag sign or the "Hornblower's sign" for significant teres minor involvement.
*
Glenohumeral Stability:
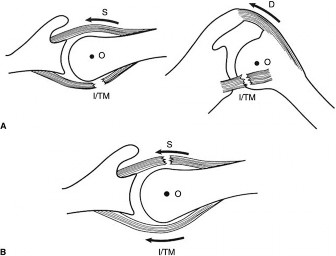
These muscles, along with the other rotator cuff muscles, form a force couple that depresses and centers the humeral head within the glenoid fossa during arm elevation. This prevents superior migration of the humeral head during deltoid contraction. In cases of posterior cuff tears, particularly massive ones, this centering effect is compromised, potentially leading to posterior-superior humeral head migration and glenohumeral arthritis (cuff tear arthropathy).
*
Posterior Stability:
The teres minor, due to its inferior insertion and innervation by the axillary nerve, plays a unique role in preventing posterior and inferior subluxation of the humeral head. Its integrity is particularly important in conditions involving posterior instability or deficiency.
*
Muscle Atrophy and Fatty Infiltration:
Chronic tears, especially those with significant retraction, are prone to muscle atrophy and fatty infiltration (assessed by Goutallier classification on MRI). This irreversible process significantly impacts muscle quality, tendon mobility, and the long-term success of repairs, often leading to higher re-tear rates and poorer functional outcomes. Understanding these biomechanical consequences underscores the importance of timely diagnosis and appropriate surgical intervention for symptomatic tears.
Indications & Contraindications
The decision to proceed with operative versus non-operative management for infraspinatus and teres minor tears is multifactorial, balancing patient factors, tear characteristics, and functional demands.
Operative Indications
- Acute, traumatic full-thickness tears: Especially in active, younger patients (<60 years), with a clear traumatic event and significant functional deficit (e.g., severe external rotation weakness, inability to actively externally rotate). Repair within 3-6 weeks is often recommended to prevent retraction and fatty infiltration.
- Symptomatic full-thickness tears unresponsive to non-operative management: Persistent pain, weakness, and functional limitations despite a dedicated 3-6 month course of conservative treatment (e.g., physical therapy, NSAIDs, injections).
- Partial-thickness articular-sided tears (>50% thickness) with persistent symptoms: While less common for posterior cuff, significant partial tears can be debrided and repaired or augmented.
- Significant functional impairment: Objective weakness in external rotation, positive external rotation lag sign, or Hornblower's sign, impacting daily activities or sport.
- Retracted tears with reasonable tissue quality: If the tendon is mobile and can be advanced to the footprint without excessive tension, even moderately retracted tears (Patte classification Stage 2, Sugaya Type II/III) may be considered for repair.
- Associated lesions requiring surgical address: Concomitant biceps pathology, labral tears, or significant impingement that necessitates surgical intervention, allowing for simultaneous cuff repair.
Non-Operative Indications
- Asymptomatic tears: Tears discovered incidentally on imaging in patients without pain or functional deficit.
- Partial-thickness tears (<50% thickness) with mild symptoms: Initial trial of physical therapy, activity modification, and pain management.
- Degenerative tears in low-demand or elderly patients: Individuals with low functional requirements, good compensatory mechanisms, or significant comorbidities precluding surgery.
- Patients unwilling or medically unfit for surgery: Co-morbidities such as severe cardiovascular disease, uncontrolled diabetes, or high anesthetic risk.
- Massive, irreparable tears: Tears with severe retraction, extensive fatty infiltration (Goutallier stage >3), or significant muscle atrophy that are deemed irrecoverable. These patients may be candidates for alternative treatments like reverse total shoulder arthroplasty, superior capsule reconstruction, or palliative debridement, but direct repair is not indicated.
Contraindications
- Active infection: Local or systemic infection.
- Uncontrolled medical comorbidities: Conditions that significantly increase surgical or anesthetic risk.
- Irreparable tears: Severe fatty infiltration (Goutallier stage 3 or 4), muscle atrophy, severe retraction (to the glenoid rim or beyond), and poor tissue quality. Attempting direct repair in these cases is futile and associated with high re-tear rates.
- Established cuff tear arthropathy: Advanced glenohumeral arthritis secondary to chronic rotator cuff deficiency. These cases often require arthroplasty (e.g., reverse total shoulder arthroplasty).
- Patient refusal or unrealistic expectations.
Operative vs. Non-Operative Indications for Infraspinatus and Teres Minor Tears
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Acute Traumatic Tears | Younger, active patients with full-thickness tears, significant weakness, minimal retraction. Prompt repair (within 6 weeks) ideal. | Elderly, low-demand patients, or those with significant comorbidities. Very small partial tears without significant functional deficit. |
| Chronic Symptomatic Tears | Persistent pain and weakness (>3-6 months) despite adequate conservative therapy. Full-thickness or significant partial (>50%) tears. Good tendon mobility and tissue quality. | Mild symptoms, good compensatory function, or small partial-thickness tears (<50%). Patients with significant comorbidities or low functional demands. |
| Functional Deficit | Objective external rotation weakness, positive external rotation lag sign, or Hornblower's sign interfering with ADLs/work/sport. | Acceptable functional status despite imaging findings. |
| Tear Characteristics | Full-thickness or significant partial tears. Minimal-to-moderate retraction (Patte Stage 1-2, Sugaya Type I-III). Good muscle belly quality (Goutallier Stage 0-2). | Small partial-thickness tears. Irreparable tears (severe retraction, Goutallier Stage 3-4, severe atrophy). Established cuff tear arthropathy. |
| Associated Pathology | Concomitant pathology (e.g., biceps, labrum) requiring surgical intervention. | No other surgical indications, or comorbidities outweighing benefits of surgery. |
| Patient Factors | Active, motivated patient with good general health, realistic expectations. | Elderly, sedentary patient, high surgical risk, patient refusal. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical for successful arthroscopic repair of infraspinatus and teres minor tears.
Pre-Operative Planning
-
Clinical Assessment:
- History: Detailed history of injury mechanism (traumatic vs. insidious), duration of symptoms, previous treatments, pain characteristics, and functional limitations. Special attention to external rotation weakness, overhead activities, and sleep disturbance.
-
Physical Examination:
- Inspection: Atrophy of the infraspinous fossa (suggestive of chronic infraspinatus or suprascapular nerve pathology).
- Palpation: Tenderness over the posterior aspect of the greater tuberosity.
- Range of Motion (ROM): Active and passive forward flexion, abduction, internal and external rotation. Note any loss of external rotation.
- Strength Testing: Assess deltoid, supraspinatus (Jobe's test), infraspinatus (resisted external rotation in neutral and 90° abduction), and teres minor (Hornblower's sign - resisted external rotation in 90° abduction and 90° external rotation). The external rotation lag sign (for infraspinatus) and drop sign (for teres minor) are highly specific for full-thickness tears.
- Special Tests: Impingement signs, stability tests.
-
Imaging Studies:
- Plain Radiographs: AP, scapular Y, and axillary views. Assess for acromial morphology (e.g., Type II or III acromion), acromioclavicular joint arthritis, glenohumeral arthritis (especially superior migration of the humeral head), and bone spurs.
-
Magnetic Resonance Imaging (MRI):
The gold standard for soft tissue evaluation. Assess:
- Tear location, size, and pattern: Full-thickness vs. partial, L-shaped, crescentic.
- Tendon retraction: Measured in millimeters from the footprint or relative to the glenoid (Patte classification).
- Muscle belly quality: Fatty infiltration (Goutallier classification I-IV) and muscle atrophy. These are crucial prognostic indicators.
- Associated pathology: Labral tears, biceps pathology, glenohumeral chondral lesions, and suprascapular nerve compression (e.g., paralabral cysts in the spinoglenoid notch).
- CT Arthrogram: Useful in complex cases, especially re-revisions, or when MRI is contraindicated. Provides excellent bone detail and visualization of the articular cartilage, as well as indirect visualization of cuff tears.
- Anesthesia Consultation: Evaluate patient comorbidities, discuss anesthetic plan (general anesthesia with regional nerve block—interscalene block—for post-operative pain control).
- Informed Consent: Thorough discussion of surgical risks (re-tear, stiffness, infection, nerve injury), benefits, and expected recovery. Highlight the often-prolonged rehabilitation for posterior cuff repairs.
Patient Positioning
The choice between the lateral decubitus and beach chair position depends on surgeon preference, familiarity, and specific tear characteristics. Each position has distinct advantages and disadvantages.
-
Lateral Decubitus Position:
-
Advantages:
- Excellent visualization of the posterior cuff, glenoid, and posterior labrum.
- Gravity-assisted distraction of the glenohumeral joint, often simplifying instrument passage.
- Improved working space for posterior portals.
- Allows for robust traction, which can aid in cuff mobilization and reduction.
-
Disadvantages:
- Requires more extensive patient setup with traction tower and counter-traction.
- Potential for brachial plexus stretch injury from traction if not carefully monitored.
- Risk of skin pressure injuries.
- Cervical spine considerations.
- Setup: Patient positioned on the non-operative side. Torso angled approximately 30-45 degrees posteriorly. Axillary roll placed to protect the neurovascular bundle. All bony prominences (e.g., iliac crest, malleoli) are well-padded. The arm is suspended in approximately 30-45 degrees of abduction and 15 degrees of forward flexion using a traction device, with 10-15 lbs of traction. The head and neck are neutral, secured in a supportive cushion.
-
Image Integration Opportunity:
This would be a good place for an image illustrating patient positioning or portal placement related to the posterior cuff.
-
Advantages:
-
Beach Chair Position:
-
Advantages:
- More physiological position, akin to upright activities.
- Easier conversion to an open procedure if necessary.
- Excellent for anterior and superior cuff access.
- Allows for easy manipulation of the arm during surgery.
-
Disadvantages:
- Potential for cerebral hypoperfusion ("beach chair hypotension") if blood pressure is not carefully managed.
- Less natural distraction of the glenohumeral joint, making instrument passage and visualization more challenging for posterior structures.
- Access to the posterior greater tuberosity can be more difficult than in lateral decubitus, particularly for lower posterior tears (teres minor).
- Setup: Patient seated at 60-70 degrees. Head secured in a headrest, ensuring neutral cervical alignment. Torso may be slightly elevated. Non-operative arm is tucked. Operative arm is draped free or supported on an arm holder, allowing full range of motion. Blood pressure monitoring at the brain level is crucial.
-
Advantages:
Regardless of the chosen position, diligent padding of all pressure points and careful attention to neurovascular protection are paramount.
Detailed Surgical Approach / Technique
The goal of infraspinatus and teres minor repair is to anatomically reattach the torn tendon(s) to their footprint on the greater tuberosity, achieving a stable, tension-free repair that can heal. While open and mini-open techniques exist, the arthroscopic approach has become the gold standard due to reduced morbidity, improved visualization, and comparable outcomes.
Arthroscopic Technique
-
Portal Placement:
- Posterior Portal (Standard): Approximately 2 cm medial and 2 cm inferior to the posterolateral corner of the acromion. Used for initial diagnostic arthroscopy and subsequent posterior instrumentation.
- Anteroinferior Portal: Created under direct visualization, inferior to the middle glenohumeral ligament, for glenohumeral inspection and instrument access.
- Anterosuperior Portal: Often used as a working portal, superior to the subscapularis, providing access to the anterior glenohumeral joint and cuff footprint.
- Lateral Working Portal(s): Typically 2-3 cm distal to the lateral acromion edge, in line with the tear. Essential for anchor placement and suture management for the infraspinatus and teres minor. A posterolateral portal, often slightly more posterior than a standard lateral portal, is particularly useful for teres minor repairs.
- Posterolateral Portal (Accessory): This portal is often critical for the repair of the infraspinatus and especially the teres minor. It's usually placed 3-4 cm distal to the posterolateral corner of the acromion, providing a direct trajectory to the posterior-inferior greater tuberosity footprint.
-
Diagnostic Arthroscopy (Glenohumeral Joint):
- Systematic inspection of the glenohumeral joint (biceps tendon, labrum, glenoid and humeral head cartilage, anterior/posterior capsule).
- Evaluate the articular side of the rotator cuff for partial tears (PASTA lesions) or extension of the full-thickness tear.
- Assess suprascapular nerve health by visualizing the nerve and vasculature at the spinoglenoid notch, looking for paralabral cysts or compression.
-
Subacromial Space Preparation:
- Move the arthroscope to the subacromial space. Perform a thorough bursectomy to clear visualization.
- Assess the undersurface of the acromion for impingement, and perform an acromioplasty if indicated (Type II or III acromion with symptomatic impingement). Ensure sufficient decompression for the repaired cuff to glide freely.
-
Tear Assessment and Mobilization:
- Tear Pattern Identification: Clearly define the tear geometry. Infraspinatus tears can be crescent-shaped, L-shaped (extending into the supraspinatus), or U-shaped. Teres minor tears are often part of a more extensive posterior-inferior cuff tear.
- Cuff Mobilization: The most critical step. Aggressively release adhesions from the undersurface of the deltoid, posterior capsule, and surrounding tissues. This allows for tension-free advancement of the tendon. Release of the posterior capsule may be necessary, especially for chronic, retracted tears. Utilize an arthroscopic shaver, radiofrequency probe, and blunt dissectors. Ensure the tendon can reach its anatomical footprint without excessive tension.
-
Footprint Preparation:
- Decorticate the greater tuberosity in the area corresponding to the infraspinatus and teres minor insertions. This promotes a bleeding bone bed for healing. Use a shaver or burr, being careful not to over-resect bone. Remove residual soft tissue and calcifications.
-
Suture Anchor Placement and Repair Technique:
- The aim is to recreate the anatomical footprint and achieve a robust compression of the tendon to bone. The double-row repair technique is generally preferred for larger tears, providing superior initial fixation strength and broader footprint coverage compared to single-row.
-
Medial Row Anchors:
Placed 6-10 mm medial to the articular margin, along the posterior aspect of the greater tuberosity.
- For infraspinatus tears, anchors are typically placed on the middle facet.
- For teres minor tears, anchors are placed on the inferior facet, potentially requiring a more inferior or posterolateral portal trajectory.
- Usually 2-3 anchors are placed, depending on tear size. Knotless anchors are often used here.
- Suture Management: Pass sutures through the mobilized tendon edge. Various suture passing devices (e.g., BirdBeak, Scorpion, arthroscopic suture lassos) are used. The specific pattern (e.g., simple, mattress, modified Mason-Allen) depends on surgeon preference and tear morphology. For posterior cuff tears, precise suture placement to capture adequate tendon tissue is crucial for maintaining external rotation strength.
-
Lateral Row Anchors:
Placed at the lateral cortical edge of the greater tuberosity. These anchors compress the medial row sutures and the tendon to the bone, maximizing contact pressure.
- Usually 2-3 anchors are placed. Knotted or knotless anchors can be used.
- For infraspinatus , these anchors are placed more superiorly on the lateral facet.
- For teres minor , these anchors are placed more inferiorly and posteriorly.
- Double-Row Suture Bridge Configuration: A common and effective technique involves using medial row anchors (e.g., with tape or multiple sutures) to pull the tendon medially, and then using lateral row anchors to create a compression "bridge" over the tendon, pressing it onto the footprint.
- Isolated Teres Minor Repair: If primarily a teres minor tear, focus on anchors directly at its inferior facet footprint and a distinct repair. Often, it's a component of a massive posterosuperior tear, requiring a comprehensive approach.
-
Assessment of Repair:
- Carefully inspect the repair construct for tension, coverage, and stability.
- Perform gentle range of motion (AROM, PROM) to ensure the repair is stable and not under excessive tension, especially with external rotation.
- Debride any remaining unstable tissue.
-
Closure:
- Close portals with absorbable sutures or sterile strips.
- Apply a sterile dressing and place the arm in a sling with an abduction pillow, often restricting external rotation based on the repair tension and tear size.
Open / Mini-Open Technique
- Indications: Reserved for massive, retracted tears where arthroscopic mobilization is difficult, complex revision cases, or surgeons less familiar with advanced arthroscopic techniques.
-
Approach:
Typically a posterior or posterolateral skin incision.
- Deltoid Split: A common approach for posterior cuff access involves splitting the deltoid fibers (usually 3-5 cm from the acromion) to expose the infraspinatus. Care must be taken to avoid injury to the axillary nerve, which runs approximately 5-7 cm distal to the acromion.
- Deltoid Detachment (Rarely needed): In extreme cases, a portion of the deltoid may be detached and repaired, but this carries a higher risk of deltoid dysfunction.
- Exposure: After deltoid exposure, the infraspinatus and teres minor tendons are identified. The bursectomy and mobilization are performed openly.
- Repair: Similar principles of footprint preparation and suture anchor placement are employed, but with direct visualization. The tension and coverage of the repair are manually assessed.
- Closure: Meticulous repair of the deltoid (if detached or extensively split) and layered closure of the wound.
Complications & Management
Despite advancements in surgical technique, complications can occur following infraspinatus and teres minor rotator cuff repair. A thorough understanding of potential complications, their incidence, and appropriate management strategies is essential.
Common Complications
-
Re-tear: The most common complication, with reported rates varying widely (5-30%) depending on tear size, patient age, tissue quality, and follow-up duration. Tears of the posterior cuff, especially large, retracted tears, can have higher re-tear rates.
- Incidence: Varies, but generally higher in massive, chronic, or revision repairs. Factors include poor tissue quality (fatty infiltration), patient non-compliance with rehab, and technical failure.
-
Salvage Strategies:
- Conservative management: For asymptomatic or mildly symptomatic re-tears, especially in older, lower-demand patients.
- Revision repair: For symptomatic re-tears in active patients with good tissue quality, provided the tendon is mobilizable and not excessively retracted. May involve augmentation with patches (allograft, xenograft) or superior capsule reconstruction (SCR) for massive defects.
- Reverse Total Shoulder Arthroplasty (rTSA): For failed repairs in older patients with cuff tear arthropathy, severe deltoid dysfunction, or irreparable massive tears.
- Palliative debridement: For irreparable tears with severe pain but contraindications to arthroplasty.
-
Stiffness (Arthrofibrosis): Post-operative shoulder stiffness, or "frozen shoulder," is a significant concern, particularly in patients with pre-existing stiffness, diabetes, or in whom aggressive early immobilization was employed.
- Incidence: ~5-15%. Higher in diabetic patients and those with prolonged immobilization.
-
Salvage Strategies:
- Aggressive physical therapy: Intensive stretching, mobilization, and modalities.
- Corticosteroid injections: Intra-articular injections can help reduce inflammation and pain to facilitate therapy.
- Manipulation Under Anesthesia (MUA): If conservative measures fail, MUA can be performed to release adhesions.
- Arthroscopic Capsular Release: For recalcitrant cases of severe stiffness not responding to MUA.
-
Infection: Superficial or deep surgical site infection, though relatively rare in arthroscopic shoulder surgery.
- Incidence: <1% for deep infection. Higher in immunocompromised patients or prolonged cases.
-
Salvage Strategies:
- Superficial infection: Oral antibiotics, local wound care.
- Deep infection: Surgical debridement and irrigation, IV antibiotics (culture-directed). Retained hardware may need to be removed if infection persists.
-
Neurovascular Injury:
- Axillary Nerve: Risk of injury during deltoid split (open approach) or with excessive lateral portal placement/instrumentation. Leads to deltoid weakness and teres minor weakness, sensory loss over the lateral shoulder.
- Suprascapular Nerve: Risk of injury in the spinoglenoid notch during extensive posterior capsular release or excessive thermal energy use. Leads to infraspinatus (and supraspinatus) weakness and atrophy.
- Brachial Plexus: Traction neurapraxia in lateral decubitus position.
- Incidence: Rare (<1%).
-
Salvage Strategies:
- Observation: Many neurapraxias resolve spontaneously.
- Nerve conduction studies/EMG: To assess severity and prognosis.
- Nerve repair/grafting: For confirmed transection, though very rare.
- Tendon transfers: For persistent functional deficits.
-
Anchor Pull-out/Failure: Technical failure where the anchor dislodges from the bone or suture pulls out of the anchor.
- Incidence: Low, often related to poor bone quality (osteoporosis) or improper insertion technique.
- Salvage Strategies: Revision anchor placement, often using different anchor types or positions. May require augmentation in cases of poor bone stock.
-
Pain: Persistent post-operative pain despite a successful repair.
- Incidence: Variable, can be due to residual impingement, nerve irritation, or non-cuff pathology.
- Salvage Strategies: Diagnostic workup (MRI, nerve studies), physical therapy, injections, targeted nerve blocks, or revision surgery if an identifiable cause is found.
-
Deltoid Detachment (Open Repairs): Partial or complete detachment of the deltoid origin from the acromion, most common in open repairs with extensive deltoid mobilization.
- Incidence: Low, specific to open approaches.
- Salvage Strategies: Surgical reattachment of the deltoid, often with heavy sutures. Prolonged immobilization.
Complications and Management Strategies
| Complication | Incidence (Approximate) | Salvage Strategies |
|---|---|---|
| Re-tear | 5-30% | Conservative management (asymptomatic/mildly symptomatic), Revision repair (with/without augmentation/SCR), Reverse TSA (for cuff tear arthropathy), Palliative debridement. |
| Stiffness | 5-15% | Aggressive physical therapy, Corticosteroid injections, Manipulation Under Anesthesia (MUA), Arthroscopic capsular release. |
| Infection | <1% (deep) | Oral antibiotics (superficial), Surgical debridement & IV antibiotics (deep), Hardware removal if persistent. |
| Neurovascular Injury | <1% (Axillary/Suprascapular nerve) | Observation, Nerve conduction studies/EMG, Nerve repair/graft (rare), Tendon transfers for persistent deficit. |
| Anchor Pull-out | Low | Revision anchor placement, consideration of alternative fixation techniques or augmentation. |
| Persistent Pain | Variable | Diagnostic workup (MRI, nerve studies), Physical therapy, Injections, Targeted nerve blocks, Revision surgery for identifiable pathology. |
| Deltoid Detachment | Low (Open repairs only) | Surgical reattachment of deltoid, prolonged immobilization. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as crucial as the surgical technique for achieving successful outcomes after infraspinatus and teres minor repair. The protocol aims to protect the repair, restore range of motion, regain strength, and facilitate return to function. Protocols are typically individualized based on tear size, repair quality, patient age, and activity level. Close communication between the surgeon and physical therapist is paramount.
Phase I: Protection & Passive Motion (0-6 Weeks)
- Goals: Protect the healing repair, minimize pain, prevent stiffness, begin passive range of motion.
-
Immobilization:
- Sling with an abduction pillow/splint worn continuously (except for hygiene and exercises).
- Duration of immobilization varies from 4 to 6 weeks, often longer for larger, more challenging repairs or if the repair was under significant tension.
- Crucially, avoid active external rotation to protect the infraspinatus/teres minor repair.
-
Passive Range of Motion (PROM):
- Initiated early, typically within the first week, often performed by a therapist or with the uninvolved arm.
- Forward Flexion: To 90-120 degrees, depending on comfort and repair stability.
- Abduction: Limited to 90 degrees.
- External Rotation: Limited to neutral (0 degrees) or slightly beyond, avoiding any pain or tension at the repair site. This is critical for infraspinatus/teres minor protection. Often, an external rotation block is incorporated into the abduction sling.
- Internal Rotation: Hand-behind-back to lumbar spine, avoiding capsular stretch.
- Scapular Mobility: Passive scapular exercises (elevation, depression, protraction, retraction) to prevent stiffness and improve scapulothoracic rhythm.
- Elbow, Wrist, Hand: Active ROM and strengthening exercises to prevent stiffness and maintain upper extremity function.
- Pain Management: NSAIDs, analgesics, cryotherapy.
Phase II: Controlled Active Motion & Light Strengthening (6-12 Weeks)
- Goals: Gradually restore full non-painful passive and active-assisted range of motion, initiate active range of motion, begin light isometric strengthening.
- Immobilization: Discontinue sling as tolerated, usually around 6 weeks, but still avoid strenuous activities.
- Active-Assisted Range of Motion (AAROM): Progress from PROM to AAROM (e.g., pulley exercises, wand exercises).
-
Active Range of Motion (AROM):
Gradually introduce AROM as tolerated, ensuring no pain or compensation.
- Focus on achieving full forward flexion, abduction, and internal rotation.
- External Rotation: Active external rotation is introduced cautiously, usually after 8-10 weeks, starting with gravity-eliminated positions.
-
Isometric Strengthening:
- Begin light isometric exercises for the deltoid, rotator cuff (internal rotation, gentle external rotation against resistance), and scapular stabilizers.
- Progress very gradually.
- Proprioception: Begin light proprioceptive exercises (e.g., small ball rolls on a wall).
Phase III: Progressive Strengthening (12-24 Weeks)
- Goals: Restore full strength, endurance, and neuromuscular control. Progress to functional activities.
-
Strengthening:
- Progressive resistive exercises with elastic bands, light weights, and bodyweight.
- Focus on rotator cuff strengthening (internal and external rotators, especially the repaired infraspinatus/teres minor), deltoid, and scapular stabilizers (serratus anterior, rhomboids, trapezius).
- Open and closed kinetic chain exercises.
- Eccentric strengthening.
- Endurance: Incorporate exercises to improve muscular endurance.
- Advanced Proprioception: Introduce exercises challenging balance and coordination.
- Functional Training: Begin sport-specific or work-specific exercises as appropriate.
Phase IV: Return to Activity (24+ Weeks)
- Goals: Gradual, safe return to full activities, including sports and heavy labor.
- Sport-Specific/Work-Specific Drills: Progressively increase intensity, duration, and complexity of activities.
- Plyometrics: For athletes, introduce plyometric exercises if appropriate.
- Return to Play/Work: Typically not before 6 months post-surgery, and only when strength, endurance, and range of motion are near normal, and the patient demonstrates good control and no pain with functional movements. Full return to overhead sports may take 9-12 months.
- Maintenance: Continue a home exercise program indefinitely to maintain strength and flexibility and reduce the risk of re-injury.
Key Principles for Posterior Cuff Rehabilitation:
*
Protect External Rotation:
This is the most critical aspect in the early phases for infraspinatus and teres minor repairs.
*
Individualization:
Each patient's progress is unique. The protocol must be flexible and adapted based on pain, ROM, and strength progression.
*
Pain-Free Movement:
Exercises should not cause significant pain.
*
Scapular Control:
Maintaining optimal scapulothoracic mechanics is vital for rotator cuff function.
Summary of Key Literature / Guidelines
The body of literature regarding infraspinatus and teres minor rotator cuff tears, while less extensive than for supraspinatus tears, highlights several key themes and guidelines for optimal management.
-
Diagnosis and Imaging: MRI remains the gold standard for diagnosing posterior cuff tears, allowing assessment of tear size, retraction, and crucial prognostic indicators like muscle atrophy and fatty infiltration (Goutallier classification). Studies consistently show that severe fatty infiltration (Goutallier stage >3) and significant muscle atrophy are strong predictors of re-tear and poorer functional outcomes, irrespective of repair technique. The presence of an external rotation lag sign and Hornblower's sign are highly indicative of infraspinatus and teres minor tears, respectively.
-
Surgical vs. Non-Surgical Management: Current guidelines generally advocate for an initial trial of non-operative management (physical therapy, NSAIDs, activity modification) for chronic, degenerative, or partial-thickness tears without significant functional deficit. However, for acute, traumatic full-thickness tears in active patients, especially those under 60 years of age, early surgical repair is often recommended to prevent muscle atrophy and retraction, which are detrimental to repairability and outcomes. Systematic reviews emphasize that non-operative treatment for full-thickness tears results in functional deficits, particularly external rotation weakness, reinforcing the indication for surgical intervention in symptomatic cases.
-
Surgical Technique (Arthroscopic vs. Open, Single vs. Double Row):
- Arthroscopic Approach: The overwhelming majority of literature supports the arthroscopic approach as the preferred technique due to lower morbidity, improved visualization of the entire cuff, and comparable clinical outcomes to open repair.
- Double-Row vs. Single-Row: For medium to large full-thickness tears of the rotator cuff, including the infraspinatus, many studies demonstrate superior biomechanical properties and potentially lower re-tear rates with double-row repair techniques (e.g., suture bridge) compared to single-row. However, meta-analyses often show no significant difference in long-term clinical outcomes between single-row and double-row repairs for all rotator cuff tears, suggesting that tear characteristics, tissue quality, and surgeon experience may be more influential than the specific construct in some cases. For smaller tears, a single-row repair may suffice. For posterior cuff tears specifically, restoring the anatomical footprint and achieving robust fixation is paramount to maintaining external rotation strength.
- Teres Minor Repair: Given its anatomical position and function, the teres minor tear, often occurring in conjunction with massive posterosuperior tears, presents unique challenges. Its repair is critical for restoring posterior stability and external rotation. Techniques often involve direct repair to the inferior facet of the greater tuberosity, sometimes requiring a dedicated posterolateral portal.
-
Augmentation and Biologics: For massive, irreparable tears, or tears with poor tissue quality, various augmentation strategies have been explored. Biologic scaffolds (e.g., dermal allografts, xenografts) and synthetic patches aim to enhance tendon healing or provide structural support. Superior Capsule Reconstruction (SCR) using dermal allograft or fascia lata autograft has emerged as a viable option for irreparable superior and posterior cuff tears, particularly in younger patients, to restore superior stability and improve function, though long-term outcomes are still evolving.
-
Post-Operative Rehabilitation: The literature consistently stresses the importance of a structured, progressive rehabilitation program. Early protected passive range of motion, particularly for the posterior cuff, is crucial to prevent stiffness while protecting the repair. Gradual introduction of active motion and strengthening, with careful attention to avoiding active external rotation for the first 6-8 weeks post-op, is a common theme across protocols. Patient compliance with rehabilitation is a significant factor in overall success.
-
Prognostic Factors: Key factors influencing outcomes include patient age (younger patients generally have better healing potential), tear size and retraction (smaller tears heal better), fatty infiltration (higher Goutallier stages correlate with higher re-tear rates), and the presence of associated pathology (e.g., biceps, glenohumeral arthritis). The ability to achieve a tension-free repair is paramount.
In summary, the management of infraspinatus and teres minor rotator cuff tears necessitates a comprehensive approach, integrating clinical findings with advanced imaging. While arthroscopic repair, often employing a double-row construct, is the preferred method for symptomatic, repairable tears, judicious patient selection, meticulous surgical technique, and dedicated post-operative rehabilitation are all critical determinants of successful long-term outcomes. Continued research on biologics and augmentation strategies holds promise for improving results in challenging, irreparable cases.
