Introduction & Epidemiology
Proximal humerus fractures (PHFs) represent a significant orthopaedic challenge, ranking as the third most common fracture in the elderly population, trailing only hip and distal radius fractures. Their incidence is rising globally, largely attributed to an aging demographic and the increasing prevalence of osteoporosis. These fractures account for approximately 5-6% of all fractures and are particularly common in post-menopausal women, often resulting from low-energy falls. In younger, more active individuals, PHFs typically occur due to high-energy trauma.
The anatomical complexity of the proximal humerus, coupled with its critical role in shoulder function and the intricate vascular supply to the humeral head, makes the management of these fractures highly nuanced. Treatment strategies range from conservative management to a spectrum of surgical interventions, including open reduction and internal fixation (ORIF) with plates or intramedullary nails, hemiarthroplasty, and reverse shoulder arthroplasty (RSA). The choice of treatment is dictated by numerous factors, including fracture pattern (as classified by Neer or AO/OTA), patient age, bone quality, functional demands, and surgeon experience.
Despite advancements in surgical techniques and implant design, the rates of unsatisfactory outcomes and complications following surgery for PHFs remain notable. The sequelae can significantly impair shoulder function, leading to pain, stiffness, and long-term disability. Understanding, classifying, and managing these complications is paramount for orthopaedic surgeons. The Boileau classification, introduced by Boileau et al. in 2001, provides a valuable framework for categorizing the most common and clinically relevant sequelae of surgical management for PHFs, allowing for a more standardized approach to their recognition and subsequent salvage. This comprehensive review aims to provide a high-yield academic reference on the surgical management of proximal humerus fractures and the subsequent complications as categorized by Boileau's classification.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the proximal humerus is fundamental to successful management and complication avoidance in PHFs.
Gross Anatomy
The proximal humerus comprises four key segments (as per Neer's classification):
*
Humeral Head:
The articular portion, articulating with the glenoid. It has an average inclination of 130-140 degrees relative to the humeral shaft and approximately 30 degrees of retroversion relative to the epicondylar axis. Maintaining these parameters is crucial for optimal shoulder kinematics.
*
Greater Tuberosity (GT):
The most superior and lateral prominence, serving as the insertion site for the supraspinatus, infraspinatus, and teres minor tendons (external rotators and abductors). Displacement of the GT significantly compromises rotator cuff function.
*
Lesser Tuberosity (LT):
The anterior prominence, providing insertion for the subscapularis tendon (internal rotator). Displacement here also impacts rotator cuff integrity.
*
Humeral Shaft:
The diaphysis, extending distally from the surgical neck.
The surgical neck is the common fracture site between the tuberosities and the shaft. The anatomical neck lies between the articular surface and the tuberosities.
Vascular Supply
The vascularity of the humeral head is critical, as its disruption is a primary determinant of avascular necrosis (AVN). The main blood supply is derived from the ascending branch of the anterior humeral circumflex artery (AHCA) and the posterior humeral circumflex artery (PHCA).
* The
AHCA
typically gives rise to the
arcuate artery (or anterolateral ascending artery)
, which penetrates the bicipital groove and supplies the superior and anterior aspects of the humeral head.
* The
PHCA
contributes to the inferomedial aspect.
* Additional contributions come from the periosteal plexus, particularly from the rotator cuff insertions.
Fracture patterns that significantly disrupt the AHCA and PHCA, such as 4-part fractures, anatomical neck fractures, and valgus-impacted fractures with disruption of the medial calcar, carry a higher risk of AVN. Neer's criteria for AVN risk include displacement of the articular segment, disruption of the medial calcar, and the size of the metaphyseal extension attached to the head.
Neurological Structures
Several nerves are at risk during surgical approaches:
*
Axillary Nerve:
Most commonly injured. It courses posteriorly, inferior to the humeral head, through the quadrangular space, then wraps around the surgical neck laterally, supplying the deltoid and teres minor. Injury can result in deltoid paralysis and a sensory deficit over the lateral shoulder.
*
Musculocutaneous Nerve:
Located more medially, supplying the biceps and coracobrachialis.
*
Radial Nerve:
Distal to the surgical neck, particularly at risk during distal shaft fixation or if extending the approach.
Biomechanics and Deforming Forces
Fracture patterns in the proximal humerus are largely influenced by the pull of various muscle groups:
*
Supraspinatus:
Tends to pull the greater tuberosity superiorly and posteriorly.
*
Subscapularis:
Tends to pull the lesser tuberosity medially.
*
Pectoralis Major, Latissimus Dorsi, Teres Major:
Tend to adduct and internally rotate the humeral shaft, displacing it medially and anteriorly relative to the head.
*
Deltoid:
Can contribute to abduction and superior migration of the shaft if there is extensive soft tissue stripping.
Understanding these deforming forces is essential for achieving and maintaining an anatomical reduction. Poor reduction, particularly of the tuberosities, directly impairs rotator cuff function and contributes to pain, weakness, and altered shoulder kinematics.
Indications & Contraindications
The decision-making process for managing proximal humerus fractures is complex, weighing fracture morphology, patient factors, and functional goals.
Non-Operative Indications
Conservative management is typically reserved for fractures with minimal displacement or those in patients with significant comorbidities precluding surgery.
*
Minimally displaced fractures:
Displacement of the articular segment typically <1 cm and angulation <45 degrees, particularly in 2-part surgical neck fractures.
*
Stable 2-part fractures:
Non-displaced or minimally displaced surgical neck fractures, stable greater tuberosity avulsions with minimal displacement (<3-5mm).
*
Elderly patients with low functional demands:
Where the risks of surgery outweigh the potential benefits, or in cases of severe osteoporosis where stable fixation is unlikely.
*
Patients with significant medical comorbidities:
Uncontrolled diabetes, severe cardiac or pulmonary disease, or other conditions that contraindicate general anesthesia or prolonged rehabilitation.
*
Non-compliant patients:
Those unlikely to adhere to post-operative rehabilitation protocols.
Operative Indications
Surgical intervention is generally indicated for displaced or unstable fractures in patients with reasonable bone quality and functional expectations.
*
Displaced 2-part surgical neck fractures:
Angulation >45 degrees or displacement >1 cm, especially in younger, active patients.
*
Displaced 2-part greater tuberosity fractures:
Displacement >5 mm (or >3mm in younger patients) for superior or posterior retraction, leading to rotator cuff dysfunction.
*
Displaced 2-part lesser tuberosity fractures:
Displacement >10 mm, which can block internal rotation.
*
3-part fractures:
Surgical neck fracture with displacement of one tuberosity.
*
4-part fractures:
Surgical neck fracture with displacement of both tuberosities, often associated with a high risk of AVN.
*
Fracture-dislocations:
Any proximal humerus fracture associated with glenohumeral dislocation, especially if irreducible or locked.
*
Open fractures:
Require emergent débridement and fixation.
*
Polytrauma patients:
Often prioritized for early stabilization.
*
Young, active patients:
With significant displacement, aiming for anatomical reduction and restoration of function.
*
Vascular or neurological compromise:
Rarely, these fractures can compromise the neurovascular bundle requiring urgent exploration and repair.
Contraindications
-
Absolute Contraindications:
- Active infection in the surgical field.
- Severe soft tissue compromise (e.g., extensive skin necrosis, open fracture with gross contamination).
- Uncontrolled systemic medical conditions that make anesthesia or surgery exceedingly dangerous.
-
Relative Contraindications:
- Severe osteoporosis precluding stable implant fixation, which may favor arthroplasty options (hemiarthroplasty or RSA) acutely.
- Extremely comminuted fractures with irreparable articular damage, particularly in older patients, where primary arthroplasty may be a more predictable option.
- Non-compliant patients who will not engage in the necessary post-operative rehabilitation.
Table: Operative vs. Non-Operative Indications for Proximal Humerus Fractures
| Indication Category | Non-Operative Treatment | Operative Treatment |
|---|---|---|
| Fracture Pattern |
- Minimally displaced 2-part fractures (surgical neck <45° angulation, <1cm displacement; GT <3-5mm displacement)
- Stable valgus-impacted fractures - Select 3-part fractures in elderly, low-demand patients |
- Displaced 2-part surgical neck fractures (>45° angulation or >1cm displacement)
- Displaced 2-part tuberosity fractures (GT >5mm or LT >10mm displacement) - All 3-part and 4-part fractures in active patients - Fracture-dislocations (irreducible/locked) - Anatomical neck fractures in younger patients |
| Patient Factors |
- Elderly, low functional demand
- Significant medical comorbidities precluding surgery - Severe osteoporosis (where fixation is tenuous) - Non-compliant patient |
- Young, active patients
- Good bone quality - High functional demands - Absence of absolute medical contraindications |
| Specific Scenarios | - Impending skin compromise due to fracture in highly comorbid patients (consider external fixation) |
- Open fractures
- Associated neurovascular injury - Bilateral proximal humerus fractures (often favor early stabilization) - Polytrauma patients (often prioritized for early stabilization) |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is critical for optimizing outcomes and anticipating challenges in PHF surgery.
Diagnostic Imaging
- Plain Radiographs: Standard anteroposterior (AP), scapular Y, and axillary lateral views are the initial imaging modalities. These provide basic information on fracture pattern, displacement, and glenohumeral alignment.
-
Computed Tomography (CT) Scan:
Essential for complex fractures, particularly 3- and 4-part patterns, fracture-dislocations, and those involving the articular surface. CT provides detailed information on:
- Degree of comminution, especially of the metaphysis and tuberosities.
- Articular involvement, step-off, or impaction.
- Accurate assessment of tuberosity displacement and rotation, crucial for rotator cuff repair.
- Glenoid rim fractures or impaction.
- 3D CT reconstructions are invaluable for visualizing fracture morphology and planning reduction strategies.
- Magnetic Resonance Imaging (MRI): Less commonly used in the acute setting due to motion artifact and time constraints. May be considered if there is suspicion of pre-existing rotator cuff pathology or significant soft tissue injury not apparent on CT.
Patient Assessment and Medical Optimization
- Medical Comorbidities: A thorough medical evaluation is necessary to optimize any underlying conditions (e.g., cardiac disease, diabetes, pulmonary issues) to minimize perioperative risks. Consultation with internal medicine or anesthesia may be required.
- Bone Quality: Clinical assessment and review of imaging (osteopenia evident on X-ray, low Hounsfield units on CT) guide implant selection. DEXA scans may be considered for pre-existing osteoporosis.
- Functional Demands: Understanding the patient's pre-injury activity level, occupation, and recreational goals helps in setting realistic expectations and tailoring the treatment plan.
- Patient Education and Expectations: Discussing potential outcomes, expected recovery timeline, and common complications (e.g., stiffness, pain, risk of reoperation) is vital for informed consent and patient satisfaction.
Implant Selection
The choice of implant depends on fracture pattern, bone quality, surgeon preference, and patient factors.
*
Locking Plate and Screw Systems:
Currently the most prevalent for ORIF of most displaced PHFs (2-, 3-, and select 4-part fractures). Modern locking plates offer angular stability, important in osteoporotic bone.
*
Intramedullary Nailing:
Less common for complex PHFs due to potential for humeral head perforation, but can be useful for certain 2-part surgical neck fractures, particularly in younger patients.
*
Hemiarthroplasty (HA):
Considered for irreparable 4-part fractures, anatomical neck fractures, or fracture-dislocations with a high risk of AVN, especially in older patients. Requires an intact and repairable rotator cuff.
*
Reverse Shoulder Arthroplasty (RSA):
Increasingly utilized for irreparable 4-part fractures, especially in older, low-demand patients with existing rotator cuff deficiency or poor bone quality, offering more predictable pain relief and functional outcomes than HA in this specific demographic.
Patient Positioning and Anesthesia
- Anesthesia: General anesthesia is standard. An interscalene nerve block is frequently used adjunctively to provide excellent post-operative pain control and muscle relaxation, facilitating reduction.
-
Positioning:
- Beach Chair Position: Preferred by many surgeons. The patient is placed in a semi-sitting position, allowing for easy access to the shoulder, improved visualization of the proximal humerus, and gravity-assisted retraction. The head is stabilized. The affected arm is prepped free to allow for full range of motion.
- Supine Position with a Bolster: An alternative where a bolster is placed under the ipsilateral scapula to elevate the shoulder. This provides a stable base and allows for easier C-arm access but may offer less direct visualization compared to beach chair.
- Fluoroscopy: A C-arm fluoroscope is essential for intraoperative assessment of reduction and implant placement. Ensure clear AP and axillary views can be obtained without repositioning.
- Tourniquet: While not routinely used for deltopectoral approaches due to the extensive vascularity, it may be considered for anterolateral approaches or if extensive soft tissue dissection is anticipated, though its use is debated due to potential for increased complications.
Detailed Surgical Approach / Technique
The deltopectoral approach is the most common and versatile for managing proximal humerus fractures, offering excellent exposure of the proximal humerus while respecting neurovascular structures.
Deltopectoral Approach
- Incision: A curvilinear incision is made, beginning just medial to the coracoid process, extending distally along the deltopectoral groove for approximately 8-12 cm, ending at the mid-shaft of the humerus.
- Superficial Dissection: The subcutaneous tissue and fascia are incised. Careful attention is paid to identifying and protecting the cephalic vein , which typically lies within the deltopectoral groove. It is usually retracted laterally with the deltoid, though some surgeons prefer medial retraction with the pectoralis major.
- Deltopectoral Interval: The interval between the deltoid muscle (laterally) and the pectoralis major muscle (medially) is developed. This is a relatively avascular plane.
-
Deep Dissection:
- The clavipectoral fascia is incised deep to the pectoralis major.
- The conjoint tendon (biceps short head and coracobrachialis) is identified and retracted medially. The musculocutaneous nerve enters the coracobrachialis muscle about 5-8 cm distal to the coracoid and should be protected.
- The underlying subdeltoid bursa and adhesions are released, exposing the fracture site.
- Axillary Nerve Protection: This is paramount. The axillary nerve, often accompanied by the posterior humeral circumflex artery, courses inferiorly to the humeral head and wraps around the surgical neck. It is approximately 5-7 cm distal to the acromion. During exposure, avoid excessive retraction of the deltoid and ensure the inferior margin of the wound is protected, typically by careful blunt dissection and the use of a broad, smooth retractor (e.g., Hohmann).
Fracture Reduction
- Debridement: Hematoma and any interposed soft tissues are meticulously removed from the fracture site to facilitate reduction and visualize fracture fragments.
- Initial Traction and Manipulation: Gentle longitudinal traction is applied to the arm, often combined with manual manipulation, to disengage impacted fragments and restore length.
-
Fragment Identification and Provisional Fixation:
- The humeral head fragment is typically identified first.
- Joy-sticks (K-wires or small screws) can be placed into the head fragment and the shaft to gain control and facilitate manipulation.
- The medial calcar buttress is a critical anatomical landmark for restoring humeral length and alignment. Restoration of the medial cortical continuity is vital for load sharing and preventing varus collapse.
- Tuberosity fragments are identified. Often, rotator cuff sutures (e.g., FiberWire) are placed through the tuberosity fragments early to aid in their reduction and later for reattachment.
- Reduction is performed under fluoroscopic guidance, confirming restoration of the articular-shaft angle (130-140 degrees) and retroversion (approximately 30 degrees).
- Provisional Stabilization: Once anatomical or near-anatomical reduction is achieved, it is temporarily held with K-wires. These wires should be placed to avoid interfering with subsequent plate and screw placement.
Plate Fixation (Locking Plate Technique)
-
Plate Selection and Positioning:
- A pre-contoured locking plate (e.g., Philos plate, Peri-Loc plate) is selected, matching the size and contour of the proximal humerus.
- The plate is positioned on the lateral aspect of the humerus, typically 5-8 mm distal to the superior edge of the greater tuberosity. This placement is critical to avoid impingement on the subacromial space and the rotator cuff during abduction and rotation.
- Ensuring adequate space for the rotator cuff insertion is paramount.
-
Distal Fixation:
- The plate is initially secured to the humeral shaft with one or two cortical screws or non-locking screws through the elongated plate holes to allow for minor adjustments in height and rotation. Compression may be applied if a transverse fracture component is present.
-
Proximal Fixation (Humeral Head):
- Locking head screws are then directed into the humeral head fragment. These screws provide angular stability and do not rely on compression for fixation, which is advantageous in osteoporotic bone.
- Aim for 5-7 locking screws in the humeral head, strategically placed to maximize purchase, avoiding penetration of the articular cartilage. Screw trajectories should be divergent and subchondral.
- Calcar Screws: At least two locking screws are typically directed inferomedially to engage the dense bone of the calcar (medial column). These provide crucial medial support against varus collapse, a common failure mode.
-
Tuberosity Fixation and Suture Augmentation:
- The reduced greater and lesser tuberosities are often secured to the plate through dedicated suture eyelets or holes using strong non-absorbable sutures (e.g., FiberWire). These sutures are passed through the rotator cuff insertions and secured to the plate, providing additional rotational stability and preventing tuberosity pull-out or displacement.
- This suture augmentation is vital for maintaining tuberosity reduction and facilitating rotator cuff healing.
-
Final Checks:
- Fluoroscopic images in multiple planes (AP, axillary, Y-view) are obtained to confirm anatomical reduction, correct plate position, appropriate screw length, and absence of articular penetration.
- The shoulder is put through a gentle range of motion to ensure no impingement of the plate or screws and to assess stability.
- Wound Closure: The wound is irrigated. If appropriate, a drain may be placed. The deltopectoral interval is loosely approximated. Subcutaneous tissue and skin are closed in layers.
Alternative Techniques (Briefly)
- Anterolateral (Delta-split) Approach: Less common for ORIF due to greater risk to the axillary nerve, but can provide direct access to the greater tuberosity for isolated avulsion fractures.
- Intramedullary Nailing: Preferred for certain diaphyseal-proximal junction fractures or select 2-part surgical neck fractures, particularly in younger patients. Requires careful entry portal placement to avoid rotator cuff damage.
- Arthroplasty: For irreparable fractures (4-part, anatomical neck), especially in the elderly. Hemiarthroplasty involves replacing the humeral head, requiring intact tuberosities for rotator cuff reattachment. Reverse Shoulder Arthroplasty replaces both humeral and glenoid components, often preferred when the rotator cuff is deficient or irreparable.
Complications & Management
Despite meticulous surgical technique, sequelae following PHF surgery are not uncommon. Boileau et al. (2001) provided a foundational classification for these complications, enabling a standardized approach to diagnosis and salvage.
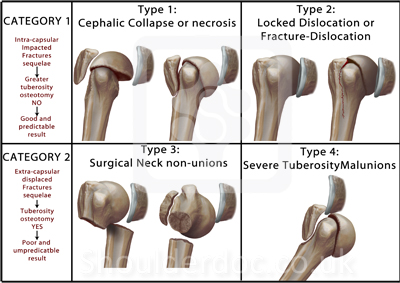
Boileau's Classification of Sequelae of Surgery for Proximal Humerus Fractures:
*
Type 1: Humeral head collapse or necrosis, minimal tuberosity malunion
*
Type 2: Locked dislocations of fracture dislocations
*
Type 3: Surgical neck non-union
*
Type 4: Severe tuberosity malunion
This classification highlights the most clinically significant issues affecting long-term outcomes.
Type 1: Humeral Head Collapse or Necrosis, Minimal Tuberosity Malunion
-
Etiology:
- Avascular Necrosis (AVN): Primary cause is disruption of the humeral head vascular supply, particularly the ascending branch of the AHCA. Risk factors include fracture type (4-part, anatomical neck), degree of displacement, extensive soft tissue stripping during surgery, and iatrogenic devascularization.
- Collapse: Often a consequence of AVN, but can also occur due to poor bone quality (osteoporosis) with inadequate medial support (absence of calcar screws or medial comminution).
- Incidence: Varies significantly depending on the fracture type and initial fixation, ranging from 5% to over 30% for high-risk fractures (e.g., 4-part).
- Presentation: Persistent, deep shoulder pain; progressive loss of motion, particularly external rotation and elevation; crepitus. Imaging (X-ray, CT) reveals characteristic changes: sclerosis, cystic changes, flattening, and eventually collapse of the articular surface.
-
Management:
- Early/Mild AVN/Collapse: Limited activity, pain management. If the collapse is minor and tuberosities are well-healed, symptoms may be manageable.
-
Progressive or Severe Collapse/Necrosis:
- Debridement and Refixation with Bone Graft: In specific cases of early collapse with a viable remaining head fragment, particularly in younger patients, debridement of necrotic bone and revision fixation with structural bone grafting may be attempted.
-
Arthroplasty:
The most common salvage procedure.
- Hemiarthroplasty (HA): If the rotator cuff and glenoid are relatively healthy. Outcomes are variable, often limited by tuberosity healing.
- Reverse Shoulder Arthroplasty (RSA): Preferred for older patients, especially if the rotator cuff is compromised (e.g., non-union of tuberosities, rotator cuff tear) or if the glenoid is also significantly affected. RSA offers more predictable pain relief and functional elevation in this setting.
Type 2: Locked Dislocations of Fracture Dislocations
- Etiology: Occur when an initial fracture-dislocation is either not adequately reduced during primary surgery or redislocates post-operatively, becoming "locked" due to impaction or interposition of soft tissues (e.g., biceps tendon, rotator cuff) or bony fragments.
- Incidence: Less common but highly debilitating.
- Presentation: Severe pain, gross deformity, profound loss of active and passive range of motion, often with the arm held in a specific position. Imaging confirms persistent dislocation.
-
Management:
- Acute/Early Locked Dislocation: Aggressive open reduction and stable fixation of the fracture fragments. Release of any interposed soft tissues.
-
Chronic Locked Dislocation:
Management is more challenging.
- Open Reduction with Osteotomy: May be necessary to release the humeral head. This is complex and carries high risks.
-
Arthroplasty:
Often the most predictable solution for chronic locked dislocations, particularly in older patients.
- Hemiarthroplasty or Reverse Shoulder Arthroplasty: The choice depends on rotator cuff integrity, glenoid status, and patient factors. RSA is often favored due to better stability and functional outcomes in the setting of chronic muscle contractures and compromised soft tissues.
Type 3: Surgical Neck Non-Union
-
Etiology:
Failure of the surgical neck fracture fragments to heal within an expected timeframe (typically 6 months). Contributing factors include:
- Inadequate reduction (gap at fracture site).
- Unstable fixation (improper plate length, insufficient screws, poor bone purchase).
- Excessive soft tissue stripping devitalizing fragments.
- Interposition of soft tissue at the fracture site.
- Systemic factors: Smoking, diabetes, malnutrition, NSAID use.
- Local biology: Poor vascularity, significant comminution.
- Incidence: Ranges from 5% to 15%, depending on fracture complexity and patient population.
- Presentation: Persistent pain at the fracture site, tenderness, palpable motion (pseudarthrosis), crepitus, weakness, and often hardware failure (screw breakage, plate bending) on imaging. X-rays show lack of bridging callus, lucency at the fracture site.
-
Management:
-
Revision Osteosynthesis with Bone Grafting:
The most common approach. Requires removal of failed hardware, meticulous debridement of the non-union site, fresh fracture surfaces are created, anatomical reduction, and more robust fixation.
- Bone Grafting: Autograft (iliac crest) or allograft (cancellous chips, structural strut) is essential to provide osteogenic, osteoinductive, and osteoconductive properties.
- Plate Augmentation: A stronger plate, longer plate, or double plating may be used.
- Intramedullary Nailing: Can be considered for specific patterns of surgical neck non-unions, offering central stability.
-
Conversion to Arthroplasty:
If revision osteosynthesis is deemed unlikely to succeed due to severe comminution, poor bone quality, extensive bone loss, or failed previous attempts.
- Hemiarthroplasty or Reverse Shoulder Arthroplasty: Choice depends on tuberosity and rotator cuff status. RSA is increasingly preferred for non-unions with significant bone loss or compromised cuff.
-
Revision Osteosynthesis with Bone Grafting:
The most common approach. Requires removal of failed hardware, meticulous debridement of the non-union site, fresh fracture surfaces are created, anatomical reduction, and more robust fixation.
Type 4: Severe Tuberosity Malunion
-
Etiology:
Failure to adequately reduce or maintain reduction of the greater or lesser tuberosities, leading to their healing in an abnormal position.
- Greater Tuberosity (GT) Malunion: Most common, typically displaced superiorly, anteriorly, or posteriorly. Leads to subacromial impingement, rotator cuff dysfunction, and restricted motion.
- Lesser Tuberosity (LT) Malunion: Less common, usually displaced medially. Can block internal rotation.
- Incidence: High if tuberosity fixation is not adequately secured or if there is significant osteoporosis at the insertion sites.
- Presentation: Persistent pain (especially with overhead activities or specific rotations), impingement symptoms, weakness of specific rotator cuff movements, severely limited active range of motion, but often preserved passive range of motion. Imaging (CT scan is best) reveals malposition of the tuberosities.
-
Management:
- Non-Operative: For mild symptoms, pain management, and physiotherapy.
-
Surgical Revision (Osteotomy and Refixation):
- Early/Symptomatic Malunion: An osteotomy to mobilize the malunited tuberosity, re-reduction, and stable re-fixation with strong sutures (transosseous) and/or small plates. This is technically demanding and carries risks of devascularization. Bone grafting may be required.
- Rotator Cuff Repair/Augmentation: Often, the malunion is associated with rotator cuff tendinopathy or tears, requiring concurrent repair.
-
Arthroplasty:
For severe, intractable symptoms, particularly in older patients where osteotomy is too risky or unlikely to yield good results, or if the rotator cuff is irreparably damaged.
- Reverse Shoulder Arthroplasty (RSA): Increasingly utilized for severe tuberosity malunions, especially those with associated rotator cuff dysfunction, as it bypasses the need for a functional rotator cuff and provides reliable pain relief and functional elevation.
Other General Complications
- Infection: Superficial or deep. Management involves antibiotics, débridement, and potentially hardware removal.
- Nerve Injury: Axillary nerve most common (deltoid weakness, sensory deficit). Managed with observation, EMG, and possibly neurolysis if no recovery.
- Hardware Impingement/Failure: Pain and restricted motion. May require hardware removal after fracture union, or revision if associated with non-union.
- Rotator Cuff Tears: Can be pre-existing or iatrogenic. Managed with repair if identifiable and feasible.
- Stiffness: Common post-operative complication. Managed with aggressive physical therapy, manipulation under anesthesia, or arthroscopic capsular release.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Boileau Type | Incidence Range (approx.) | Presentation | Salvage Strategy |
|---|---|---|---|---|
| Humeral Head AVN/Collapse | Type 1 | 5-30% | Persistent pain, progressive loss of motion, crepitus; sclerosis, collapse on imaging |
Non-operative for mild cases.
Revision ORIF with bone graft (rare). Hemiarthroplasty or Reverse Shoulder Arthroplasty. |
| Locked Dislocation | Type 2 | Rare, but severe | Severe pain, gross deformity, profound loss of motion, arm held in fixed position |
Early: Open reduction & stable ORIF.
Chronic: Open reduction with osteotomy (complex), Hemiarthroplasty or Reverse Shoulder Arthroplasty. |
| Surgical Neck Non-Union | Type 3 | 5-15% | Persistent pain, palpable motion, weakness, hardware failure; lucency at fracture site on imaging |
Revision ORIF with bone grafting
(autograft/allograft).
Plate augmentation or IM nailing. Conversion to Hemiarthroplasty or Reverse Shoulder Arthroplasty. |
| Severe Tuberosity Malunion | Type 4 | Variable, high if initial fixation poor | Pain (impingement), weakness, restricted active motion (especially specific rotations) |
Non-operative for mild cases.
Surgical osteotomy & re-fixation (challenging). Rotator cuff repair/augmentation. Reverse Shoulder Arthroplasty. |
| Infection | N/A | 1-5% | Pain, swelling, erythema, warmth, fever, purulent drainage | Surgical débridement, antibiotics, possible hardware removal. |
| Nerve Injury (Axillary) | N/A | 2-10% | Deltoid weakness/paralysis, sensory loss over lateral shoulder | Observation, EMG, rarely neurolysis/repair. |
| Hardware Impingement/Failure | N/A | Common (if not removed post-union) | Pain, restricted motion. Failure with non-union. |
Hardware removal (after union).
Revision fixation (if non-union). |
| Rotator Cuff Tear (iatrogenic/exacerbated) | N/A | Variable | Pain, weakness, impaired active motion | Repair (if feasible), or manage as per primary tear. |
| Stiffness | N/A | Common | Restricted active and passive range of motion |
Aggressive physiotherapy.
Manipulation under anesthesia. Arthroscopic capsular release. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as critical as the surgery itself for optimizing functional outcomes and preventing stiffness or further complications. Protocols are phased and tailored to the fracture stability, implant type, bone quality, and patient compliance. Communication between the surgeon and the physical therapist is paramount.
Phase I: Protection and Early Motion (0-6 Weeks Post-Op)
Goal:
Protect the healing fracture and soft tissue repairs, control pain and inflammation, prevent stiffness.
*
Immobilization:
The arm is typically immobilized in a sling or abduction brace for the initial 4-6 weeks, depending on fracture stability and tuberosity repair integrity. The sling is removed for hygiene and specific exercises only.
*
Pain Management:
Pharmacological intervention (NSAIDs, opioids, muscle relaxants) and cryotherapy.
*
Early Passive Range of Motion (PROM):
Initiated carefully and within pain tolerance.
*
Pendulum Exercises:
Gentle, gravity-assisted swings of the arm while leaning forward.
*
Supine External Rotation:
With the elbow flexed to 90 degrees, using the contralateral hand or a stick to gently externally rotate the arm, limited to 0-30 degrees as tolerated and based on stability.
*
Supine Forward Flexion:
Gentle elevation of the arm (e.g., table slides or rope and pulley system), typically limited to 90-120 degrees, avoiding active muscle contraction.
*
Scapular Mobilization:
Gentle scapular retraction and protraction exercises.
*
Elbow, Wrist, Hand Exercises:
Active range of motion for distal joints to prevent stiffness and maintain circulation.
*
Restrictions:
*
NO active shoulder motion.
*
NO lifting, pushing, or pulling.
*
Avoid sudden movements.
*
Avoid weight-bearing through the arm.
Phase II: Progressive Active Motion (6-12 Weeks Post-Op)
Goal:
Gradually restore active range of motion, initiate gentle strengthening, improve neuromuscular control.
*
Discontinuation of Sling:
As pain decreases and fracture healing progresses (confirmed radiographically).
*
Active-Assisted Range of Motion (AAROM):
Transition from PROM to AAROM, then to Active Range of Motion (AROM) as tolerated.
*
Self-assisted Pulleys:
For forward flexion and abduction.
*
Wall Climbs/Finger Walks:
For elevation.
*
Stick Exercises:
For internal and external rotation, and elevation.
*
Gentle Isometric Strengthening:
*
Rotator Cuff Isometrics:
Against a wall for internal/external rotation, abduction, and adduction. Emphasis on pain-free contraction.
*
Deltoid Isometrics:
Carefully initiated.
*
Scapular Stabilization:
Continue and progress exercises for scapular control and positioning.
*
Restrictions:
*
Avoid heavy lifting or carrying.
*
No sudden, ballistic movements.
*
Avoid overhead activities with resistance.
Phase III: Strengthening and Return to Activity (12+ Weeks Post-Op)
Goal:
Restore full strength, endurance, and proprioception. Gradual return to functional activities, including sport.
*
Progressive Resistive Exercises:
*
TheraBand Exercises:
For all planes of shoulder motion, gradually increasing resistance.
*
Light Weights:
Progress from bodyweight to light dumbbells for rotator cuff and deltoid strengthening.
*
Plyometrics:
For high-demand athletes, introduced carefully.
*
Endurance Training:
Repetitive low-load exercises.
*
Proprioceptive Training:
Balance and coordination exercises for the shoulder joint.
*
Functional Training:
Tailored to the patient's occupational or recreational demands.
*
Return to Activity:
Gradual progression to overhead activities, lifting, and sport-specific drills. Return to contact sports or heavy labor usually not before 6 months and requires full strength, range of motion, and radiographic healing.
*
Continued Monitoring:
Regular follow-up appointments with the surgeon to assess radiographic healing and clinical progress.
Key Considerations for Rehabilitation:
*
Bone Quality:
Poorer bone quality may necessitate a more conservative and prolonged protection phase.
*
Tuberosity Repair:
The integrity and healing of tuberosity repairs are paramount. Aggressive active motion too early can lead to pull-out or malunion.
*
Rotator Cuff Status:
If there was a pre-existing rotator cuff tear or significant damage, the protocol will be modified to prioritize cuff healing.
*
Patient Compliance:
Success heavily relies on the patient's adherence to the rehabilitation program.
*
Individualization:
Each patient's progress is unique; protocols serve as guidelines, not rigid prescriptions. Adjustments must be made based on pain, swelling, and clinical assessment.
Summary of Key Literature / Guidelines
The landscape of proximal humerus fracture management has evolved considerably, driven by technological advancements and a deeper understanding of fracture biology and biomechanics.
Early literature, notably Neer's seminal work in the 1970s, established the classification system that remains widely used and recognized the high incidence of AVN in complex fractures. Initial treatment paradigms often favored conservative management or basic internal fixation, leading to considerable rates of malunion, non-union, and stiffness.
The advent of locking plate technology in the early 2000s marked a significant shift. Studies by Hintermann et al. (2000) and subsequent investigations demonstrated that locking plates offered improved angular stability, particularly in osteoporotic bone, compared to conventional plating. This led to a surge in ORIF for displaced PHFs, with initial enthusiasm for improved outcomes. However, concurrent with this increased surgical activity, the recognition of specific complications also grew, prompting the development of classifications like Boileau's (2001) to systematically categorize the sequelae.
Studies comparing different ORIF techniques, such as Schiuma et al. (2018) , have explored optimal screw configurations and plate placement to reduce complications like head collapse and screw cut-out. The importance of medial column support (e.g., with calcar screws or bone grafting) to prevent varus collapse and subsequent head necrosis has been emphasized in numerous biomechanical and clinical studies (e.g., Gardner et al., 2007 ).
For complex 3- and 4-part fractures, particularly in the elderly, the debate between ORIF and primary arthroplasty (hemiarthroplasty vs. reverse shoulder arthroplasty) continues.
*
Hemiarthroplasty
gained traction for irreparable head fractures, but long-term outcomes have been inconsistent, often limited by unpredictable tuberosity healing and subsequent pain or pseudarthrosis. Reviews by
Sperling et al. (2006)
highlighted the challenges with tuberosity union.
*
Reverse Shoulder Arthroplasty (RSA)
has emerged as a compelling alternative, especially in older patients with comminuted fractures, poor bone quality, or pre-existing rotator cuff deficiency. Studies by
Gallagher et al. (2011)
and meta-analyses (e.g.,
Antuna et al., 2017
) suggest RSA provides more predictable pain relief and improved functional elevation compared to hemiarthroplasty for these complex fracture patterns, primarily because it bypasses the need for rotator cuff integrity. Current trends favor RSA for 4-part PHFs in patients over 70.
The management of complications, as classified by Boileau, is a significant area of research.
*
AVN (Boileau Type 1):
While primary prevention through careful surgical technique and fixation is key, salvage often involves arthroplasty, with RSA increasingly preferred for symptomatic, collapsed heads, particularly if tuberosities are not salvageable.
*
Non-Union (Boileau Type 3):
Management protocols typically involve revision ORIF with aggressive bone grafting. The work of
Robinson et al. (2008)
provided insights into the outcomes of surgical treatment for failed osteosynthesis. In cases of persistent non-union or significant bone loss, conversion to arthroplasty is often considered.
*
Tuberosity Malunion (Boileau Type 4):
This remains a challenging complication. While osteotomy and re-fixation can be attempted, the technical difficulty and variable outcomes often lead surgeons to consider arthroplasty, particularly RSA, for severe symptomatic malunions that compromise rotator cuff function.
Current guidelines emphasize the need for individualized treatment plans, meticulous surgical technique, and aggressive, yet protected, post-operative rehabilitation. Shared decision-making with the patient, considering their functional demands, comorbidities, and realistic expectations, is paramount. The ongoing debate surrounding the optimal initial management for certain fracture types, especially 4-part fractures in the elderly, underscores the complexity and the need for continued research to refine treatment algorithms and improve patient outcomes. The Boileau classification remains a valuable tool for understanding and communicating the specific failures encountered in the surgical management of proximal humerus fractures, guiding both treatment and future research efforts.
