Peripheral Nerve Injury: Classification & Clinical Evaluation

Key Takeaway
Peripheral nerve injuries require meticulous clinical evaluation and a profound understanding of the Seddon and Sunderland classification systems. Accurate assessment of motor function, sensibility—including two-point discrimination—and sudomotor activity dictates surgical decision-making. This guide details the pathophysiology, diagnostic testing, anatomic variations, and operative management of nerve lesions to optimize functional recovery in orthopedic practice.
Introduction to Peripheral Nerve Injuries
The management of peripheral nerve injuries remains one of the most technically demanding and prognostically unpredictable domains within operative orthopedics and hand surgery. A profound understanding of nerve microanatomy, pathophysiology, and precise clinical evaluation is mandatory for the orthopedic surgeon. The decision to observe, explore, or reconstruct a nerve lesion hinges entirely on an accurate initial assessment and a thorough grasp of the established classification systems.
This comprehensive guide delineates the foundational principles of peripheral nerve injury classification, rigorous clinical evaluation protocols—with a specific focus on the radial nerve—and the surgical tenets required to optimize functional recovery.
Pathophysiology and Classification Systems
The structural integrity of a peripheral nerve is maintained by its connective tissue layers: the endoneurium (surrounding individual axons), the perineurium (bundling axons into fascicles), and the epineurium (enveloping the entire nerve). The severity of a nerve injury is defined by which of these layers are breached. The two most universally accepted classification systems are those proposed by Seddon and Sunderland.
The Seddon Classification
Sir Herbert Seddon introduced a tripartite classification system based on the macroscopic and microscopic continuity of the nerve fibers:
- Neurapraxia: A localized conduction block without structural axonal disruption. It is typically caused by mild traction or compression. Wallerian degeneration does not occur. Recovery is spontaneous and complete, usually within days to 12 weeks.
- Axonotmesis: Disruption of the axon and myelin sheath, but preservation of the surrounding connective tissue framework (endoneurium, perineurium, epineurium). Wallerian degeneration occurs distal to the injury. Because the endoneurial tubes remain intact, regenerating axons are guided directly to their target end-organs. Recovery is typically excellent but occurs at a rate of approximately 1 mm per day.
- Neurotmesis: Complete transection or severe disorganization of the entire nerve trunk, including all connective tissue layers. Spontaneous recovery is impossible without surgical intervention.
The Sunderland Classification
Sir Sydney Sunderland expanded Seddon’s classification into five distinct degrees, offering a more granular prognostic framework based on the specific connective tissue layers involved. Later, Susan Mackinnon introduced a sixth degree to describe complex, mixed-pattern injuries.
- First Degree (Sunderland I): Equivalent to Seddon’s Neurapraxia. Localized conduction block; no Wallerian degeneration.
- Second Degree (Sunderland II): Equivalent to Seddon’s Axonotmesis. Axonal disruption with intact endoneurium.
- Third Degree (Sunderland III): Disruption of the axon and endoneurium, but the perineurium remains intact. Intrafascicular scarring occurs, which can misdirect regenerating axons. Recovery is unpredictable and often incomplete.
- Fourth Degree (Sunderland IV): Disruption of the axon, endoneurium, and perineurium. Only the epineurium remains intact. The nerve is in continuity macroscopically, but a dense neuroma-in-continuity forms. Surgical excision and repair or grafting are required.
- Fifth Degree (Sunderland V): Equivalent to Seddon’s Neurotmesis. Complete transection of the nerve trunk.
- Sixth Degree (Sunderland VI): A combination of any of Sunderland I-V within the same nerve trunk. Different fascicles sustain varying degrees of injury. This is common in severe crush or traction injuries and complicates both clinical evaluation and surgical decision-making.
Clinical Pearl: Differentiating between a Sunderland II and Sunderland III injury clinically is impossible in the acute setting. Both present with complete distal motor and sensory loss. The distinction only becomes apparent retrospectively based on the quality of spontaneous recovery, or intraoperatively via nerve action potential (NAP) monitoring.
Comprehensive Clinical Evaluation
The clinical evaluation of a peripheral nerve injury must be systematic, reproducible, and meticulously documented. The basic minimum tests recommended for evaluation encompass sensibility, motor function, and sudomotor activity.
Sensibility Evaluation
Sensibility testing evaluates the functional integrity of the sensory axons and their cortical representation. The basic minimum tests recommended for sensibility evaluation are stationary two-point discrimination (Weber test) and moving two-point discrimination (Dellon test).
- Stationary Two-Point Discrimination: Evaluates the density of slowly adapting fibers (Merkel cell complexes). Using a standardized instrument (e.g., Disk-Criminator), the prongs are applied longitudinally to the digit without blanching the skin. Normal stationary two-point discrimination is less than 6 mm at the fingertips.
- Moving Two-Point Discrimination: Evaluates the density of quickly adapting fibers (Meissner corpuscles). The prongs are moved longitudinally from proximal to distal. Moving two-point discrimination typically recovers before stationary discrimination and is normally 2 to 3 mm at the fingertips.
Surgical Warning: When performing two-point discrimination, ensure the patient's eyes are closed and that the pressure applied does not cause skin blanching, which can stimulate deeper pressure receptors and yield false-positive results.
Motor Function and Biomechanical Assessment
Motor evaluation requires a profound understanding of nerve anatomy, the order of muscle innervation, and the biomechanics of the hand and upper extremity. The radial nerve serves as an excellent model for complex motor evaluation.
Radial Nerve Innervation Sequence
Proximal muscles innervated by the radial nerve (before or within the spiral groove) include:
* Triceps brachii: Extension of the elbow.
* Anconeus: Assists in elbow extension.
* Brachioradialis: Flexion of the elbow in neutral rotation.
* Supinator: Supination of the forearm.
The radially innervated muscles having a direct influence on the hand and wrist are innervated sequentially from proximal to distal:
* Extensor Carpi Radialis Longus (ECRL) and Brevis (ECRB): Wrist dorsiflexion and radial deviation.
* Extensor Carpi Ulnaris (ECU): Wrist dorsiflexion and ulnar deviation.
* Extensor Digitorum Communis (EDC): Extension of the metacarpophalangeal (MCP) joints.
* Extensor Digiti Minimi (EDM): Independent extension of the small finger MCP joint.
* Extensor Indicis Proprius (EIP): Independent extension of the index finger MCP joint.
* Abductor Pollicis Longus (APL): Abduction of the thumb at the carpometacarpal joint.
* Extensor Pollicis Brevis (EPB): Extension of the thumb MCP joint.
* Extensor Pollicis Longus (EPL): Extension of the thumb interphalangeal (IP) joint.
Clinical Testing and Pitfalls
The motions that must be examined to evaluate radial nerve integrity include wrist dorsiflexion, radial and ulnar deviation, and thumb abduction and extension.
Pitfall: Metacarpophalangeal (MCP) extension, mediated by the radial nerve via the EDC, must be evaluated carefully. The examiner must not be confused by the extension of the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints of the fingers. PIP and DIP extension is controlled by the intrinsic muscles (lumbricals and interossei), which are innervated by the median and ulnar nerves, not the radial nerve. To isolate radial nerve function, the examiner must specifically test active extension at the MCP joint while the PIP and DIP joints are relaxed.
Anatomic Variations in Innervation
Orthopedic surgeons must be acutely aware of anatomic variations that can confound clinical examination. Standard innervation patterns are not absolute.
For example, while the intrinsic muscles of the hand are classically innervated by the ulnar and median nerves, anomalous innervation by the radial nerve occurs in about 10% of hands. In these variant cases, the posterior interosseous nerve (PIN) or superficial branches of the radial nerve may supply the first dorsal interosseous and the second and third dorsal interosseous muscles. Failure to recognize this anomaly may lead the surgeon to incorrectly assume the ulnar nerve is intact despite a high ulnar nerve laceration.
Sudomotor Function
Sudomotor function refers to the autonomic control of sweat glands, mediated by sympathetic postganglionic fibers that travel within the peripheral nerves. Because these sympathetic fibers do not undergo Wallerian degeneration in the same manner as somatic fibers, sudomotor testing is a highly reliable indicator of complete nerve transection.
Usually, a denervated area shows no sweating within about 30 minutes after a nerve injury. The loss of sympathetic tone results in anhidrosis (dry skin) and a loss of normal skin wrinkling when submerged in water (O'Riain wrinkle test).
Clinically, it is highly helpful to compare the normal and suspected injured areas by palpation with a dry fingertip. The denervated skin will feel smooth and lack the slight friction or "drag" normally provided by microscopic sweat droplets. More formal testing can be performed using the Ninhydrin test, which detects amino acids in sweat, turning purple upon exposure.
Surgical Management of Peripheral Nerve Lesions
When clinical evaluation indicates a Sunderland IV or V lesion, or when a Sunderland III lesion fails to demonstrate clinical or electrodiagnostic recovery within 3 to 6 months, surgical intervention is mandated.
Indications and Timing
- Primary Repair (Acute): Indicated for sharp, clean lacerations (e.g., glass or knife wounds). Repair should be performed within 72 hours.
- Delayed Primary Repair: Indicated for blunt trauma, avulsions, or contaminated wounds. The nerve ends are tagged to adjacent fascia to prevent retraction, and definitive repair is performed at 2 to 3 weeks once the zone of injury has demarcated.
- Secondary Repair / Grafting: Performed months after the injury when a neuroma-in-continuity is excised, or when primary repair is impossible due to a massive defect.
Patient Positioning and Preparation
The patient is positioned supine. A pneumatic tourniquet is applied to provide a bloodless field, though it should be deflated prior to final closure to ensure meticulous hemostasis, preventing postoperative hematoma which can compress the repair. High-resolution surgical loupes (minimum 3.5x to 4.5x) or an operating microscope are absolute requirements.
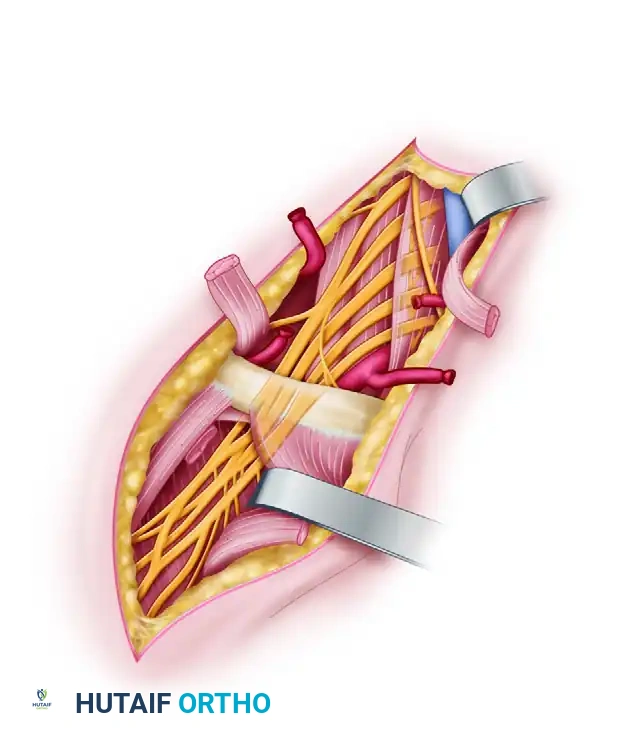
Surgical Approach and Technique
- Exposure: The incision must be extensile. The nerve should always be identified in virgin, uninjured tissue proximally and distally before tracing it into the zone of injury.
- Preparation of Nerve Stumps: In delayed repairs, the neuroma at the proximal stump and the glioma at the distal stump must be resected back to healthy, bleeding fascicles. The "mushrooming" of axoplasm from the cut end indicates healthy tissue.
- Alignment: Proper rotational alignment is critical. The surgeon must match the surface vascular patterns (vasa nervorum) and the cross-sectional fascicular topography.
- Neurorrhaphy: A tension-free repair is the most critical factor in nerve surgery. If the nerve ends cannot be coapted with an 8-0 nylon suture without tension, a nerve graft is required.
- Epineurial Repair: Sutures are placed through the epineurium. This is standard for most digital and mixed nerves.
- Group Fascicular Repair: Sutures are placed through the perineurium of matching fascicular groups. Indicated when distinct motor and sensory fascicles can be identified (e.g., the median nerve at the wrist).
- Nerve Grafting: If a gap exists, autologous nerve grafting is the gold standard. The sural nerve is the most common donor. The grafts are reversed to prevent regenerating axons from escaping through branching points.
Postoperative Assessment and Rehabilitation
The success of a peripheral nerve repair relies heavily on the postoperative protocol. In evaluating the progress of peripheral nerve injury and repair, sensibility testing, motor testing, subjective evaluation, and sudomotor function are all critically important.
Immobilization Phase
Postoperatively, the extremity is immobilized in a custom orthosis to remove all tension from the repair site. For example, following a volar wrist nerve repair, the wrist is splinted in 20 to 30 degrees of flexion for 3 to 4 weeks.
Rehabilitation and Monitoring Recovery
Following the immobilization phase, a carefully guided range of motion protocol is initiated to prevent joint contractures and promote nerve gliding.
Clinical monitoring of recovery includes:
* Tinel's Sign: An advancing Tinel's sign (a tingling sensation radiating into the nerve's distribution when tapped) indicates the leading edge of regenerating axons. It should advance approximately 1 mm per day (1 inch per month).
* Motor Recovery: Muscles are reinnervated in a strict proximal-to-distal sequence. Electromyography (EMG) can detect nascent motor unit potentials weeks before clinical contraction is visible.
* Sensory Re-education: Once protective sensation (deep pressure) returns, formal sensory re-education programs are initiated to help the brain reinterpret the altered afferent signals, improving functional tactile gnosis.
* Sudomotor Recovery: The return of sweating and normal skin texture is an excellent objective marker of autonomic reinnervation.
By adhering to these rigorous principles of classification, clinical evaluation, and meticulous surgical technique, the orthopedic surgeon can maximize the potential for functional restoration following severe peripheral nerve trauma.
📚 Medical References
- peripheral nerve injury, Am J Sports Med 11:420, 1983.
- Jabaley ME: Peripheral nerve injuries. In Evarts CM, ed: Surgery of the musculoskeletal system, New York, 1983, Churchill Livingstone. Kankaanpää U, Bakalim G: Peripheral nerve injuries of the upper extremity. Sensory return of 137 neurorrhaphies, Acta Orthop Scand 47:41, 1976.
- Leonard MH: Return of skin sensation in children without repair of nerves, Clin Orthop Relat Res 95:273, 1973.
- Luce EA, Griffi n WO: Shotgun injuries of the upper extremity, J Trauma 18:487, 1978.
- Lundborg G: A 25-year perspective of
You Might Also Like