Second or Third Toe Transplantation: Advanced Microsurgical Reconstruction

Key Takeaway
Second or third toe-to-hand transplantation is a highly specialized microsurgical procedure utilized for thumb or digital reconstruction following traumatic loss or congenital absence. This complex free tissue transfer restores critical pinch, grip, and tactile sensation. Success relies on meticulous preoperative planning, precise osteotomies, and flawless microvascular anastomoses of the dorsalis pedis or plantar arterial systems to the recipient hand vessels.
INTRODUCTION TO TOE-TO-HAND TRANSPLANTATION
The evolution of microvascular surgery has revolutionized the reconstruction of the severely traumatized or congenitally deficient hand. While the great toe wrap-around procedure remains the gold standard for aesthetic and functional thumb reconstruction, second or third toe transplantation offers a highly versatile alternative. This technique is particularly advantageous when reconstructing fingers distal to the metacarpophalangeal (MCP) joint, when multiple digits are required, or when the patient explicitly refuses great toe harvest due to concerns regarding donor site morbidity or foot aesthetics.
The primary objective of this complex free tissue transfer is the restoration of a sensate, mobile, and biomechanically stable digit capable of functional pinch and grip. By transferring a composite block of tissue—encompassing bone, joints, tendons, nerves, and a robust vascular pedicle—the orthopedic microsurgeon can reconstruct devastating hand injuries with tissue that closely mimics the native digit.
INDICATIONS AND PATIENT SELECTION
Patient selection is the cornerstone of successful microsurgical reconstruction. The procedure is technically demanding and requires profound patient compliance during the protracted postoperative rehabilitation phase.
Primary Indications
- Traumatic Amputations: Reconstruction of the thumb or multiple digits following crush injuries, avulsions, or explosive trauma where local reconstructive options are exhausted.
- Congenital Anomalies: Symbrachydactyly, amniotic band syndrome, or transverse deficiencies where functional pinch is absent.
- Metacarpal Loss: Composite defects requiring simultaneous bone and soft tissue coverage, utilizing a toe transfer combined with a vascularized metatarsal segment.
Clinical presentation of an amputated thumb and index finger following a severe explosion injury, representing a classic indication for delayed toe-to-hand reconstruction.
Contraindications
- Absolute: Active smoking or nicotine use. Nicotine-induced vasospasm is a primary catalyst for microvascular thrombosis and catastrophic flap failure. Severe peripheral vascular disease affecting the donor foot.
- Relative: Advanced age, severe systemic comorbidities (e.g., uncontrolled diabetes mellitus), or profound psychiatric instability precluding postoperative compliance.
Surgical Warning: Strict adherence to a zero-tolerance smoking policy for both the patient and visitors is mandatory. The physiological effects of nicotine can persist for weeks, and exposure during the perioperative period significantly elevates the risk of pedicle thrombosis.
PREOPERATIVE PLANNING AND VASCULAR ANATOMY
Thorough preoperative assessment of both the donor foot and recipient hand is critical. The vascular anatomy of the foot is notoriously variable, particularly regarding the dominance of the dorsal versus plantar arterial systems.
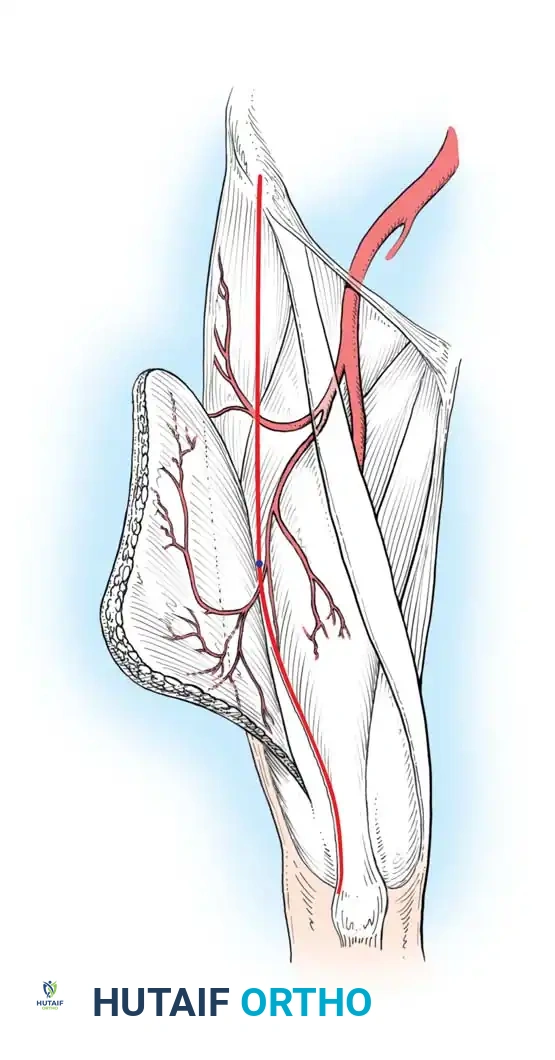
Vascular Anatomy of the Donor Site
The arterial supply to the second and third toes is derived from a dual system:
1. Dorsal System: The dorsalis pedis artery continues as the first dorsal metatarsal artery (FDMA), which bifurcates to supply the adjacent sides of the first and second toes. The anatomical course of the FDMA (Gilbert's classification) dictates the ease of dorsal dissection.
2. Plantar System: The plantar metatarsal arteries arise from the deep plantar arch. In approximately 20% of patients, the dorsal system is hypoplastic, and the plantar system is the dominant arterial supply to the toes.
Preoperative angiography or high-resolution Computed Tomography Angiography (CTA) is strongly recommended to delineate the arterial dominance and map the vascular tree, ensuring a safe and predictable harvest.
SURGICAL TECHNIQUE: DONOR FOOT DISSECTION
The procedure is ideally performed using a two-team approach to minimize ischemia time and overall operative duration. One team harvests the toe while the second team prepares the recipient site on the hand.
Incision and Exposure
- Outline the skin incisions based on the required skin paddle and the planned level of bone resection.
- Exsanguinate the lower extremity and inflate the pneumatic tourniquet.
- Begin with a dorsal incision over the first web space, extending proximally toward the dorsum of the foot. Carefully identify and preserve the dorsal venous network, tracing the tributaries proximally to the greater saphenous vein to ensure adequate venous drainage.
Plantar Dissection and Osteotomy
- Identify and dissect the plantar digital nerves, the flexor digitorum longus (FDL), and flexor digitorum brevis (FDB) tendons.
- Skeletonize the plantar digital arteries and the distal portions of the plantar metatarsal arteries.
- Osteotomy Considerations: Although dissection of the plantar structures is possible through a purely dorsal incision, a metatarsal osteotomy is frequently required to allow adequate exposure of the deep plantar structures. Attempting a dorsal approach to the plantar structures without osteotomy is technically demanding and increases the risk of iatrogenic vascular injury.
- Level of Resection:
- If the thumb or digital reconstruction is to be performed at the metacarpophalangeal (MCP) joint or more distally, disarticulate and remove the toe at the metatarsophalangeal (MTP) joint.
- If the recipient defect is more proximal, the distal metatarsal may be osteotomized at an appropriate length to replace the missing metacarpal segment in the hand.
Vascular Isolation
- Complete the soft tissue dissection, leaving the vascular pedicles (artery and vein) completely intact. Do not section the pedicle until the hand is fully prepared to receive the transplanted digit.
- Deflate the tourniquet to ensure robust perfusion of the toes by the isolated arterial pedicle.
- Use micro-vascular Acland clamps to sequentially occlude the dorsalis pedis arterial system and the plantar metatarsal arteries. This critical step determines which arterial system provides the dominant, most reliable flow to the toe.
- Once the hand team confirms readiness, ligate the non-dominant arteries and veins, section the primary vessels, and transfer the digit.
- Close the foot wounds loosely over small, thin drains as needed. Apply a bulky, nonconstricting compression bandage to the foot to prevent hematoma formation.
SURGICAL TECHNIQUE: RECIPIENT HAND DISSECTION
The preparation of the hand must be meticulous, ensuring healthy, unscarred vessels and nerves are available outside the zone of injury.
Approach for Thumb Reconstruction
- If the thumb is to be reconstructed, at least two incisions are required (similar to the great toe wrap-around procedure). Outline the planned skin incisions.
- Exsanguinate the upper limb and inflate the pneumatic tourniquet.
- Dorsal Dissection: Make a curved dorsal incision extending from the anatomical snuffbox to the remnant of the thumb. Expose the dorsal veins (cephalic system), the extensor pollicis longus/brevis tendons, the radial artery (and its first metacarpal branch), and the branches of the superficial radial nerve.
- Palmar Dissection: Make a palmar incision parallel with the thenar crease. Dissect the digital nerves, the flexor pollicis longus (FPL) tendon, and any available healthy arterial branches (e.g., princeps pollicis).
Approach for Finger or Metacarpal Reconstruction
- Distal Finger Transfer: If the toe is to be transplanted to a finger distal to the MCP joint, develop dorsal and palmar skin flaps. Expose the dorsal digital veins, the extensor digitorum communis (EDC) tendon, the volar digital arteries and nerves, and the flexor tendons.
- Proximal/Metacarpal Transfer: If the toe is transplanted with a portion of the metatarsal to replace a lost metacarpal, make a dorsal curved incision to expose the dorsal venous tributaries, extensor tendons, and the bony remnant of the metacarpal. On the palmar surface, make an oblique incision crossing the palmar creases to expose the common digital arteries, common/proper digital nerves, and flexor tendons.
- Deflate the tourniquet, achieve meticulous hemostasis using bipolar electrocautery, and prepare for the transfer.
TRANSPLANTATION AND MICROVASCULAR RECONSTRUCTION
Once the toe is transferred to the hand, the sequence of repair generally follows: Bone, Tendons, Arteries, Veins, and Nerves.
Osteosynthesis and Tendon Repair
- Bone Fixation: Rigid osteosynthesis is critical. While longitudinal Kirschner wires (K-wires) are the easiest and most common method, combinations of K-wires with 90-90 intraosseous wire sutures, or miniature titanium plates and screws, provide superior biomechanical stability and allow for earlier mobilization.
- Tendon Coaptation: Join the flexor and extensor tendons in the palm or near the wrist. Adjust tension carefully to establish a functional resting cascade. The FDL of the toe is typically woven into the FPL or FDP of the hand using a Pulvertaft weave.
Microvascular Anastomosis
Clinical Pearl: Before beginning any arterial anastomosis, it is imperative to demonstrate forceful, pulsatile flow (the "spurt test") from the cut end of the recipient artery. Anastomosing to a vessel in spasm or within the zone of injury guarantees failure.
- Arterial Repair: The arterial anastomoses usually connect the dorsalis pedis or the first dorsal metatarsal artery to the radial artery or first metacarpal artery. Alternatively, the plantar metatarsal arteries or plantar digital arteries may be anastomosed to the common or proper digital arteries of the fingers. Perform the anastomosis under the operating microscope using 9-0 or 10-0 nylon sutures.
- Venous Repair: Once arterial flow is established, return bleeding through the dorsal veins of the toe should be unequivocal and brisk. Anastomose one or two dominant dorsal veins to the cephalic vein tributaries or dorsal metacarpal veins.
Nerve Repair and Closure
- Nerve Coaptation: Suture the plantar digital nerves of the toes to the digital nerves of the fingers or thumb. Where available, suture the dorsal cutaneous branches of the radial or ulnar nerves to the branches of the superficial or deep peroneal nerves accompanying the transplanted toe.
- Wound Closure: Close the skin loosely. Tension over the vascular pedicle is a primary cause of venous congestion. Use small, thin rubber drains if needed.
- Skin Grafting: Supplemental split-thickness or full-thickness skin grafting is frequently necessary to achieve tension-free closure over the pedicle.

Intraoperative view demonstrating delayed reconstruction with a second toe-to-thumb free transfer. Note the tension-free closure achieved with supplemental skin grafting over the vascular pedicle.
- Apply a bulky, nonconstricting bandage incorporating a plaster splint on the palmar side to protect the repairs while allowing for postoperative swelling.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative environment must be strictly controlled to prevent vasospasm and ensure flap survival.
Ward Management and Monitoring
- Environment: The patient's room must be kept warm (ambient temperature > 75°F / 24°C). The patient should be sufficiently sedated or provided with adequate analgesia to avoid pain-induced sympathetic responses or emotional outbursts, which can trigger severe vasospasm.
- Positioning: Both the reconstructed hand and the donor foot are kept strictly elevated to promote venous drainage and minimize edema.
- Monitoring: The circulation to the transplanted digit is monitored continuously for the first 1 to 3 days. Modalities include clinical assessment (color, capillary refill, turgor), surface temperature probes, or implantable Doppler probes.
- Surgical Re-exploration: If any evidence of circulatory compromise (arterial insufficiency or venous congestion) develops, the patient must be returned to the surgical suite immediately for exploration and salvage of the anastomoses. Time is tissue.
Donor Site Management
- A compression dressing is worn on the foot for 2 or more weeks.
- This is followed by a custom-fitted elastic stocking for 2 to 4 months to control dependent edema.
- To minimize morbidity associated with second toe removal (or bilateral second toe removal), the foot should be elevated for at least 2 weeks.
- If both feet have been donors, Gordon et al. stress the importance of using a wheelchair for an additional 2 weeks. Protected weight-bearing is then initiated with crutches or a walker until the patient can ambulate easily with minimal pain.
Hand Rehabilitation
- The hand is immobilized in the protective splint for 3 to 4 weeks to allow for bony union and tendon healing.
- Following immobilization, a graduated, therapist-directed program of active mobilization is initiated.
- Full use of the transplanted digit is delayed until satisfactory motion and protective sensation return, which may take several months as nerve regeneration progresses at approximately 1 mm per day.
CLINICAL OUTCOMES AND PEDIATRIC CONSIDERATIONS
The functional and aesthetic outcomes of second and third toe transfers are highly dependent on the level of the transfer and the patient's age.

Clinical outcome at 6 months post-surgery, demonstrating restoration of useful pinch mechanics and highly acceptable aesthetic appearance.

Functional assessment revealing excellent active interphalangeal joint extension, highlighting the success of the extensor tendon coaptation and joint preservation.
Joint Transfer Kinematics
In a small but pivotal series, Singer et al. concluded that a vascularized transfer of the toe metatarsophalangeal (MTP) joint to the finger metacarpophalangeal (MCP) joint can provide painless, functional, and stable motion. Crucially, in pediatric patients, these transfers demonstrate nearly normal physeal growth potential, allowing the reconstructed digit to grow synchronously with the child.
Conversely, transfers of the toe proximal interphalangeal (PIP) joint to the finger PIP joint have historically been less rewarding. The primary challenge lies in regaining functional arc of motion and maintaining growth potential. Foo, Malata, and Kay reported on three free joint transfers and one double joint transfer; while the joints remained stable and maintained their growth potential, the range of motion of the reconstructed PIP joint was frequently limited to approximately 30 degrees.
Although this type of composite transplantation shows immense promise as a definitive solution for several difficult pediatric and traumatic surgical problems, authors caution that meticulous surgical execution and prolonged, dedicated rehabilitation are absolute prerequisites for success.
You Might Also Like