INTRODUCTION TO MULTIPLE DIGIT RECONSTRUCTION
The reconstruction of a severely mutilated hand remains one of the most formidable challenges in orthopedic and plastic microsurgery. While great toe transplantation, the wraparound procedure, and other traditional osteoplastic techniques are highly effective for isolated thumb reconstruction, a hand that has sustained the loss of the thumb alongside multiple digits—or a hand where only the thumb remains intact—is profoundly impaired. Such catastrophic injuries require a comprehensive reconstructive strategy that extends beyond simple thumb restoration.
To restore functional opposition, pinch, and broad grip strength, the transplantation of multiple toes has proven to be an invaluable surgical intervention. Depending on the specific anatomical deficits of the recipient hand, surgeons may utilize the second toe from one foot, the second toes from both feet, or an en bloc transfer of the second and third toes from a single foot. The latter can be harvested and transferred as a single neurovascular transplant, significantly reducing the number of required microvascular anastomoses while maximizing functional restoration.
INDICATIONS AND PATIENT SELECTION
Patient selection is paramount in microsurgical toe-to-hand transfers. The primary indication for second and third toe transplantation is the traumatic amputation or congenital absence of multiple digits where local reconstructive options (e.g., pollicization, local flaps) are insufficient to restore a functional tripod pinch or power grip.
Leung’s Classification of Thumb Loss
Leung developed a highly practical classification system for thumb loss that guides the reconstructive microsurgeon in selecting the most appropriate procedure. Leung specifically preferred the second toe over the great toe for certain categories of thumb and multi-digit loss due to its favorable pedicle geometry and reduced donor site morbidity.
The classification is divided into four distinct types based on the anatomical level of amputation:
Type I: Amputation distal to the interphalangeal (IP) joint. Reconstruction here often requires minimal bone but demands excellent sensate skin coverage.

Type II: Amputation proximal to the IP joint but distal to the metacarpophalangeal (MCP) joint. This level requires restoration of length and a stable joint for pinch kinematics.

Type III: Amputation proximal to the MCP joint. This represents a significant loss of the thumb ray, requiring robust osteocutaneous reconstruction to restore the first web space.
Type IV: Complete loss of the thumb ray, including the carpometacarpal (CMC) joint. This catastrophic loss often necessitates a composite flap, sometimes incorporating a dorsalis pedis skin flap with the toe transfer to reconstruct the entire first web space and thenar eminence.
BIOMECHANICS AND FUNCTIONAL OUTCOMES
The biomechanical goal of multiple toe transplantation is to provide a stable, sensate post against which remaining digits (or other transplanted toes) can articulate.
Gordon et al. conducted a landmark evaluation of 16 patients who underwent 38 digit reconstructions utilizing double toe transplantation from opposite feet. Their findings underscore the profound functional benefits of this procedure:
* Pinch and Grip: When only one or two digits remained on the hand, toe transplantation dramatically improved both function and aesthetic appearance. It provided a broader, stronger surface area for both precision pinch and power grip.
* Range of Motion: The reconstructed digits achieved a highly functional range of motion, allowing patients to perform activities of daily living (ADLs) that were previously impossible.
* Simultaneous vs. Sequential Procedures: Gordon et al. compared sequential double toe transplantations with simultaneous double toe transplantations. They concluded that simultaneous transplantation (usually harvesting one toe from each foot) resulted in an overall reduction in operating time, decreased hospital stay, and lower overall healthcare costs.
* Donor Site Morbidity: Postoperative foot morbidity was minimal provided a strict non-weightbearing routine was adhered to. Crucially, the risk of impaired ambulation is significantly lower when single toes are harvested from each foot compared to the en bloc removal of two toes (and portions of their metatarsals) from a single foot.
Surgical Warning: Harvesting multiple toes from a single foot, especially if it includes wide metatarsal resections, can severely disrupt the transverse metatarsal arch, leading to chronic metatarsalgia and altered gait mechanics. Bilateral single-toe harvest is generally preferred for minimizing donor site morbidity.
PREOPERATIVE PREPARATION AND VASCULAR MAPPING
Meticulous preoperative planning is the cornerstone of successful microsurgery. The vascular anatomy of the foot is notoriously variable, particularly regarding the dominance of the first dorsal metatarsal artery (FDMA) versus the plantar arterial system.
Vascular Assessment
- Arteriography: High-resolution, two-plane arteriography (or modern CT Angiography) is mandatory. It delineates the arterial tree of the donor foot, confirming the presence, caliber, and course of the dorsalis pedis artery and the FDMA.
- Doppler Ultrasound: Handheld Doppler probes are used to map the superficial venous system (saphenous tributaries) and confirm arterial perforators clinically.
- Recipient Site Evaluation: The vascular status of the injured hand must be assessed (e.g., Allen test, angiography) to identify suitable recipient vessels (usually the radial artery, ulnar artery, or their major branches, alongside the cephalic venous system).
Templating and Team Setup
- 3D Templating: Buncke recommended using clay models of the digits applied directly to the hand to visualize the final reconstruction. Alternatively, plaster models created from alginate impressions of the patient’s toes provide an exact volumetric template.
- Donor Site Restrictions: The selected toe may be contraindicated by acquired deformities (e.g., severe scarring, hammertoes), congenital anomalies, or peripheral vascular disease.
- Surgical Teams: Efficiency is critical to minimize ischemia time. If a single toe is transplanted, two surgical teams are required (one for the foot, one for the hand). If two toes are transplanted simultaneously from separate feet, three teams are highly recommended—two to harvest the toes and one to prepare the recipient hand.
Patient Positioning
Position the patient supine on a well-padded operating table. Place a heating and cooling blanket beneath the patient to maintain strict normothermia, as hypothermia induces peripheral vasospasm, which can be fatal to a microvascular free flap. Monitor core body temperature with an esophageal or rectal thermometer, and track fluid balance via an indwelling urinary catheter. Ensure both feet and the affected hand are prepped and draped to allow simultaneous, unhindered access.
SURGICAL TECHNIQUE: FOOT DISSECTION
The dissection of the second (and third) toe requires a bloodless field and meticulous handling of the delicate neurovascular structures.

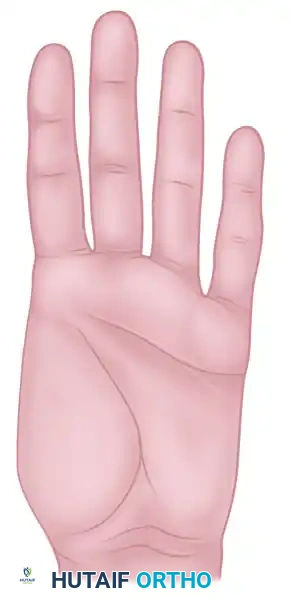
Figure A: Dorsal incisions outlined for the removal of the second toe. The dorsal foot incision allows extensive access to the neurovascular structures.

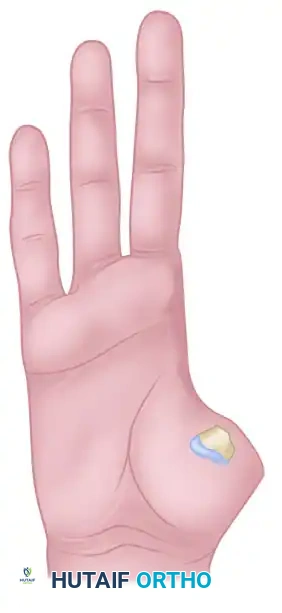
Figure B: Plantar incision designed for toe removal, allowing access to the plantar digital nerves and arterial contributions.
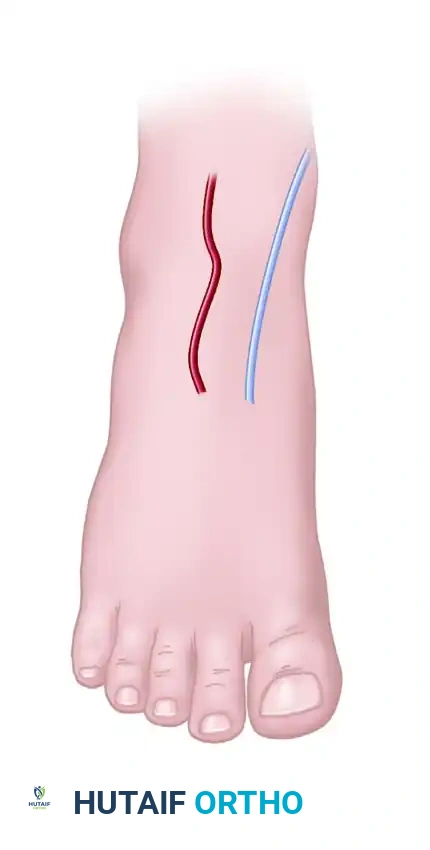
Figure C: Outline of a dorsal foot flap. This is utilized if the recipient hand requires additional vascularized skin coverage.
Step-by-Step Donor Harvest
- Skin Flap Design: Outline the skin flaps on the foot based on the specific coverage requirements of the hand. If reconstruction is at or distal to the thumb MCP joint, additional skin is rarely needed. However, for CMC level reconstructions (Type IV thumb loss), a dorsalis pedis skin flap may be incorporated. If toes are used for finger reconstruction, adjacent hand skin is usually sufficient.
- Venous Mapping: Before exsanguination, allow the dorsal veins to engorge by hanging the foot over the edge of the operating table. Use a surgical marker to outline the tributaries of the greater and lesser saphenous venous systems.
- Tourniquet Application: Exsanguinate the leg using an elastic wrap or strict elevation, and inflate the pneumatic tourniquet to the appropriate pressure.
- Dorsal Dissection: Elevate the dorsal skin flaps to identify and mobilize the saphenous venous tributaries. Carefully dissect and develop a robust venous pedicle.
- Nerve Identification: Locate the superficial peroneal nerve and meticulously dissect its branches that supply the dorsal aspect of the toe. Include these branches with the graft.
- Tendon Transection: Through the same dorsal incision, identify the extensor digitorum longus (EDL) and extensor digitorum brevis (EDB) tendons. Transect them proximally near the ankle joint to ensure sufficient length for tendon weaving in the hand.
- Arterial Dissection: Identify the dorsalis pedis artery. Mobilize it carefully, leaving its lateral branches (passing toward the second metatarsal) intact. Divide the branches supplying the great toe at the level of the first web space.
- Plantar Dissection: The arterial supply to the second (and third) toes may arise from the dorsalis pedis via the FDMA, or through a communicating artery to the plantar metatarsal arteries. Use the planned plantar incision to trace and protect these plantar digital arteries.
Clinical Pearl: The anatomical dominance of the arterial supply to the second toe can vary (Gilbert's classification). Always dissect the dorsal system first. If the FDMA is hypoplastic or absent, you must be prepared to trace the arterial pedicle into the plantar system to harvest a dominant plantar metatarsal artery.
SURGICAL TECHNIQUE: RECIPIENT HAND PREPARATION AND ANASTOMOSIS
Once the toe is isolated on its neurovascular pedicle, the tourniquet is deflated to confirm perfusion before final pedicle division. The hand team concurrently prepares the recipient site.
Osteosynthesis and Tendon Repair
- Bone Fixation: Transfer the toe to the hand. Perform rigid osteosynthesis between the toe phalanx/metatarsal and the recipient hand bone (metatarsal or carpal bone). This is typically achieved using crossed Kirschner wires (K-wires), intraosseous wiring, or miniature titanium plates and screws.
- Tendon Coaptation: Repair the extensor and flexor tendons. The toe EDL is woven into the recipient extensor (e.g., Extensor Pollicis Longus), and the toe Flexor Digitorum Longus (FDL) is repaired to the recipient Flexor Pollicis Longus (FPL) or deep finger flexors using a Pulvertaft weave to ensure early tensile strength.
Microsurgical Anastomosis
- Venous Anastomosis: Anastomose the saphenous venous system of the toe to the cephalic venous system of the hand. Generally, one robust arterial and one large venous anastomosis are sufficient, though a second vein may be anastomosed to provide a safety margin against venous congestion.
- Arterial Anastomosis: Anastomose the dorsalis pedis artery (or dominant plantar artery) to the radial artery (often end-to-side) or a major branch (end-to-end) using 9-0 or 10-0 nylon under the operating microscope.
- Nerve Repair: Perform meticulous epineurial or perineurial repairs. Suture the lateral plantar digital nerve of the toe to the ulnar digital nerve of the thumb, and the medial plantar digital nerve to the radial digital nerve. If available, coapt the superficial radial nerve branches of the hand to the deep peroneal nerve branches of the toe to maximize sensory recovery.
Closure
Loosely close the wounds to prevent any compression on the vascular pedicle. Drain the surgical sites as needed with small, thin rubber drains. Apply split-thickness skin grafts to any areas of tension; never close skin tightly over a microvascular pedicle.
POSTOPERATIVE CARE AND REHABILITATION
The success of a toe-to-hand transfer relies heavily on flawless postoperative management to prevent vasospasm and thrombosis.
Immediate Postoperative Protocol
- Dressing: Apply a bulky, non-constricting, non-compressing bandage. Support the thumb, hand, and wrist with a well-padded volar plaster splint.
- Positioning: The patient is kept on strict bed rest in a quiet, warm room. Both the reconstructed hand and the donor foot must be elevated to promote venous drainage and reduce edema.
- Anticoagulation: Postoperative anticoagulant therapy is highly surgeon-dependent but universally critical. Various authors recommend Low-Molecular-Weight Dextran (LMWD) or intravenous Heparin for the first 3 to 5 days. Aspirin (81mg) is often continued for several weeks.
- Monitoring: Continuous monitoring of the flap is mandatory. Clinical observation (color, capillary refill, tissue turgor) is supplemented by mechanical devices such as implantable Doppler probes or surface temperature monitors. A temperature drop of >2°C compared to an adjacent normal digit is an early warning sign of vascular compromise.
- Systemic Parameters: Monitor urinary output, serum hemoglobin, and hematocrit closely for the first 3 to 5 days until hemodynamic stability is assured.
Donor Site Management
Donor site morbidity is minimized by strict adherence to a non-weightbearing protocol on the involved foot for 2 to 4 weeks.
* Initially, the foot is wrapped with a soft elastic bandage.
* Following suture removal (typically at 14-21 days), an elastic support stocking is prescribed to control dependent edema.
* If only one foot was operated on, the patient may mobilize using a walker or crutches; however, extreme caution must be exercised to prevent accidental trauma to the newly reconstructed hand during ambulation.
Rehabilitation Timeline
- Days 0-7: Absolute immobilization of the hand. Bandage changes are delayed for 5 to 7 days unless vascular compromise or infection is suspected, to avoid inducing vasospasm through manipulation.
- Weeks 3-4: The thumb remains protected in a splint. Gentle, protected, therapist-guided active range of motion (ROM) is initiated to prevent tendon adhesions.
- Weeks 10-12: As bony union is confirmed radiographically, the patient graduates to more aggressive strengthening and ROM activities.
- Long-term: The most strenuous activities and heavy lifting are delayed until there is objective evidence of sensory return (advancing Tinel's sign), which protects the insensate digit from inadvertent injury.
