Revision THA: Acetabular Impaction Grafting for Severe Bone Loss
Introduction & Epidemiology
Revision total hip arthroplasty (THA) for severe acetabular bone loss remains one of the most challenging procedures in reconstructive orthopedic surgery. The increasing lifespan of patients, expanding indications for primary THA, and improved long-term survival of implants have led to a proportional rise in the incidence of revision surgeries. Acetabular bone loss can result from various etiologies, including aseptic loosening, periprosthetic osteolysis (often polyethylene wear-induced), infection, trauma, or tumor resection. The restoration of bone stock, the hip center of rotation, and the integrity of the pelvic acetabular columns is paramount for long-term implant stability and function.
Acetabular impaction grafting (AIG) with morselized allograft bone is a well-established biological reconstruction technique aimed at restoring deficient acetabular bone stock. Developed in the 1980s by Ling and Gie, AIG relies on the principles of osteoconduction and osteointegration, whereby morselized cancellous allograft bone is impacted firmly into the bone defect to create a stable, biologically active bed for subsequent cemented or uncemented cup fixation. This technique offers the advantage of biological reconstruction, allowing for potential remodeling and restoration of host bone stock, particularly in contained defects. While initially conceived for contained defects, advancements in technique and adjunctive devices like reinforcement cages have expanded its application to more complex, uncontained defects and those with discontinuity. The judicious application of AIG requires a thorough understanding of acetabular anatomy, meticulous surgical technique, and comprehensive pre-operative planning.
Surgical Anatomy & Biomechanics
A profound understanding of acetabular surgical anatomy and biomechanics is critical for successful revision THA, especially when dealing with significant bone loss. The acetabulum, a hemispherical cavity, is formed by the ischium, ilium, and pubis, converging at the triradiate cartilage.
Bony Anatomy and Columns
The acetabulum is commonly conceptualized using the Judet and Letournel two-column model:
*
Anterior Column:
Comprises the anterior iliac wing, anterior superior iliac spine, anterior inferior iliac spine, anterior half of the acetabulum, and the superior pubic ramus.
*
Posterior Column:
Consists of the ischial tuberosity, posterior half of the acetabulum, and a portion of the ilium extending to the greater sciatic notch.
The dome of the acetabulum, the primary weight-bearing area, is crucial. Defects here compromise load transmission and often necessitate robust reconstruction. The medial wall of the acetabulum is thin and borders the true pelvis; breaches here risk intrapelvic migration and neurovascular injury.
Neurovascular Structures at Risk
Several critical neurovascular structures are in close proximity to the acetabulum and are particularly vulnerable during revision surgery:
*
Sciatic Nerve:
Exits the pelvis via the greater sciatic notch, lying posterior to the acetabulum. At risk during posterior approaches, retraction, or excessive lengthening.
*
Femoral Nerve:
Courses under the inguinal ligament, anterior to the acetabulum. At risk during anterior approaches or extensive anterior dissection.
*
Obturator Nerve:
Passes through the obturator foramen. Vulnerable with extensive medial acetabular wall reconstruction or cement extravasation.
*
Superior Gluteal Nerve and Vessels:
Emerge through the greater sciatic notch above the piriformis, supplying the gluteus medius and minimus. At risk during excessive superior dissection or retraction in posterior approaches.
*
External Iliac Vessels:
Anterior and superior to the acetabulum. Potential for injury with medial wall penetration.
Biomechanics of the Acetabulum
The acetabulum acts as a socket for the femoral head, transferring forces from the lower limb to the axial skeleton.
*
Weight Bearing:
The superior and posterosuperior aspects of the acetabulum (the dome) bear the majority of axial load. Bone loss in this region dramatically impairs stability and load-bearing capacity.
*
Center of Rotation:
Restoring the anatomical hip center of rotation (COR) is critical for optimal hip biomechanics, abductor muscle function, and minimizing joint reaction forces. Superior or medial migration of the COR alters lever arms, increases muscle fatigue, and can lead to early loosening.
*
Bone Stock:
Adequate bone stock is essential for primary stability and long-term biological fixation. Severe bone loss compromises host bone for implant integration, leading to micromotion and aseptic loosening. AIG aims to reconstruct this lost bone stock, providing a foundation for graft incorporation and eventual implant support. The impacted graft serves as a biological scaffold that is gradually incorporated by creeping substitution, restoring structural integrity.
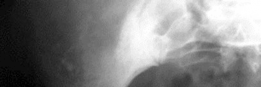
Illustration depicting the bony anatomy of the pelvis and acetabulum, highlighting key structural components relevant to surgical planning.
Indications & Contraindications
Acetabular impaction grafting is a powerful tool in the armamentarium for revision THA, but its appropriate application depends on careful patient selection and defect characterization. The Paprosky classification system for acetabular bone loss is widely used to guide reconstructive strategies.
Indications for Acetabular Impaction Grafting
AIG is primarily indicated for patients with significant acetabular bone loss, particularly those with contained defects where the host bone can provide a scaffold for graft compaction and subsequent osteointegration.
-
Aseptic Loosening with Contained Bone Defects:
- Paprosky Type IIA/IIB/IIC Defects: These represent cavitary or segmental defects with an intact rim, where morselized graft can be securely impacted. Type IIA involves minimal superior migration, IIB involves more superior migration, and IIC involves medial migration.
- AAOS Type 2/3 Defects: Cavitary defects, often associated with osteolysis.
- Goal: Restore host bone stock, reconstruct the acetabular dome, normalize the hip center of rotation, and provide a stable bed for definitive cup fixation.
-
Uncontained Defects with Reinforcement:
- Paprosky Type III Defects: These involve significant rim deficiency or pelvic discontinuity. While primarily uncontained, AIG can be used in conjunction with a reconstruction cage or plate to create a contained environment for the graft.
- Pelvic Discontinuity: In cases where pelvic discontinuity is stable or can be stabilized with plates, AIG can be used to fill the remaining defects before cage placement.
- Periprosthetic Acetabular Fracture: After appropriate fixation of the fracture, AIG can be used to address any associated bone loss.
- Revision for Infection (after staged exchange): In a second-stage procedure, AIG can be used to reconstruct bone defects once the infection has been eradicated.
- Younger Patients: Due to its biological nature and potential for long-term bone stock restoration, AIG may be favored in younger, active patients requiring revision THA, especially in the context of contained defects.
Contraindications for Acetabular Impaction Grafting
While versatile, AIG is not suitable for all cases of acetabular bone loss.
- Active Periprosthetic Joint Infection (PJI): Impaction grafting with allograft in the presence of active infection significantly increases the risk of graft failure, non-union, and persistent infection. A staged approach is mandatory, with infection eradication prior to bone grafting.
- Extensive Uncontained Defects without Adequate Containment Options: If there is insufficient host bone to contain the graft, and a reconstruction cage or plate cannot adequately bridge the defect and provide stability, AIG alone will likely fail. Large segmental defects without a supporting rim may be better managed with custom triflange components or other structural allografts.
- Severely Comorbid Patients: Patients with severe medical comorbidities precluding a lengthy and complex revision procedure may not be candidates.
- Poor Bone Quality: Extremely osteoporotic bone may not provide a sufficient foundation for graft impaction or subsequent osteointegration, increasing the risk of mechanical failure.
- Acute Periprosthetic Fracture Requiring Immediate Weight Bearing: Impaction grafting requires time for osteointegration. If immediate full weight-bearing is essential, alternative fixation strategies might be preferred.
Operative vs. Non-Operative Indications
| Indication Type | Operative Management (Revision THA with AIG) | Non-Operative Management (Conservative) |
|---|---|---|
| Aseptic Loosening | Symptomatic loosening, progressive osteolysis, significant bone loss (Paprosky II/III) | Asymptomatic loosening, stable fibrous ingrowth, minimal bone loss, high risk patient |
| Periprosthetic Infection | Two-stage exchange with AIG in the second stage (after infection eradication) | Active infection (first stage of exchange, long-term suppression in frail patients) |
| Periprosthetic Fracture | Displaced or unstable acetabular fractures with bone loss requiring reconstruction | Stable, non-displaced fractures in non-ambulatory or high-risk patients |
| Bone Loss (General) | Progressive bone loss, structural compromise, pain, functional limitation | Stable, non-progressive bone loss, asymptomatic, high surgical risk |
| Implant Failure | Mechanical failure, component migration, recurrent dislocation with bone loss | Well-functioning implant despite minor radiographic changes, high surgical risk |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is the cornerstone of a successful acetabular impaction grafting procedure. Given the complexity of revision THA with bone loss, anticipating challenges and preparing for contingencies are paramount.
Pre-Operative Assessment
-
Clinical Evaluation:
- Thorough history: Previous surgeries, complications (infection, dislocation), current symptoms (pain, instability, mechanical symptoms).
- Physical examination: Gait, range of motion, neurovascular status, abductor function, limb length discrepancy.
-
Imaging Studies:
- Standard Radiographs: Anteroposterior (AP) pelvis and true lateral views (e.g., cross-table lateral). Obtain templated AP pelvis view to assess hip center of rotation, offset, and potential component sizes. Look for implant loosening, osteolysis, fracture, component migration.
- Computed Tomography (CT) Scan: Essential for comprehensive assessment of bone loss. Use a metal-artifact reduction protocol. CT allows for detailed 3D visualization of the acetabular defects, assessment of medial wall integrity, identification of pelvic discontinuity, and quantification of remaining host bone. It helps to classify bone defects (e.g., Paprosky system).
- Magnetic Resonance Imaging (MRI): May be useful in selected cases to assess soft tissue pathology or identify occult infection, though often limited by metal artifact.
- Bone Scan: Can help differentiate between aseptic loosening and infection, or identify occult fractures.
-
Infection Work-up:
- Essential for all revision cases. Includes erythrocyte sedimentation rate (ESR), C-reactive protein (CRP).
- If suspicion of infection is high, joint aspiration with synovial fluid analysis (cell count with differential, microbiology culture) should be performed pre-operatively. If positive, a staged procedure is required.
-
Templating:
- Use digital templating software with calibrated radiographs or CT data.
- Determine the intended size and position of the new acetabular component.
- Plan for restoration of the anatomical hip center of rotation and leg length.
- Anticipate the amount and size of morselized graft required.
-
Consider adjunctive devices (reinforcement cages, anti-protrusio cages, plates) if uncontained defects or pelvic discontinuity are present.

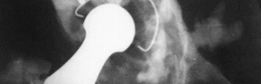
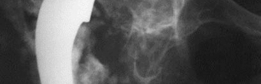
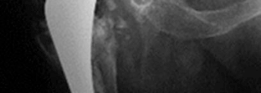
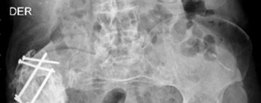
Pre-operative anteroposterior radiograph demonstrating significant acetabular bone loss, superior migration, and protrusio, indicative of a severe Paprosky Type III defect.
Axial CT image revealing extensive medial acetabular wall destruction and intrapelvic migration of the cup, underscoring the complexity of bone loss.

Coronal CT reconstruction highlighting superior and medial bone loss, necessitating robust reconstruction of the acetabular dome and medial wall.

Sagittal CT view showing the depth and extent of the acetabular defect, crucial for determining the volume of graft required and the appropriate implant size.
Graft Material Selection
- Morselized Cancellous Allograft: The most common choice. Typically derived from femoral heads. Processed to a uniform size (e.g., 3-10 mm) to facilitate impaction and vascularization. Deep-frozen or freeze-dried.
- Autograft: Can be harvested from the ipsilateral femoral head (if available and suitable) or iliac crest. Offers superior osteoinductive properties but limited quantity.
- Synthetic Bone Graft Substitutes: Rarely used alone for structural defects but can be mixed with allograft for osteoinductivity.
Patient Positioning
-
Lateral Decubitus Position:
The most common position for posterior or direct lateral approaches.
- Setup: Patient is positioned directly lateral with the operative hip superior. Pelvis is stabilized with anterior and posterior posts to prevent rotation.
- Advantages: Excellent exposure of the acetabulum and proximal femur. Allows for easy access to the greater trochanter for osteotomy if required.
- Considerations: Care must be taken to pad all pressure points (e.g., fibular head, greater trochanter of the dependent hip) to prevent nerve palsies. Ensure the torso is aligned with the spine to avoid sacral pressure.
-
Supine Position:
Used for anterior or anterolateral approaches.
- Setup: Patient supine on the operating table, often with a bump under the ipsilateral buttock to facilitate internal rotation.
- Advantages: Allows for intraoperative fluoroscopy in both AP and lateral planes without repositioning. Easier for anesthetic access and patient monitoring.
- Considerations: May limit exposure in very complex posterior defects or for extensive femoral revision.
- Draping: Standard sterile draping of the entire lower extremity to allow for free manipulation and assessment of limb length and stability.
Detailed Surgical Approach / Technique
The success of acetabular impaction grafting hinges on meticulous surgical technique, careful preparation of the graft bed, precise impaction, and appropriate fixation of the new acetabular component.
Surgical Approach
The choice of surgical approach depends on surgeon preference, the nature of the previous scar, the extent of bone loss, and whether femoral revision is also planned.
*
Posterolateral Approach:
(Kocher-Langenbeck)
*
Internervous Plane:
Between the gluteus maximus (innervated by inferior gluteal nerve) and the gluteus medius/minimus (innervated by superior gluteal nerve).
*
Advantages:
Excellent exposure of the posterior acetabulum, allows for trochanteric osteotomy if needed for femoral revision or challenging exposure. Minimizes abductor disruption.
*
Disadvantages:
Higher risk of dislocation if posterior soft tissue repair is inadequate; potential for sciatic nerve injury.
*
Direct Lateral Approach:
(Hardinge or transgluteal)
*
Internervous Plane:
Splits the gluteus medius (both parts innervated by superior gluteal nerve), detaching a portion from the greater trochanter.
*
Advantages:
Good anterior and superior acetabular exposure, allows for good abductor repair, theoretically lower dislocation rate.
*
Disadvantages:
Potential for abductor weakness, heterotopic ossification, or injury to the superior gluteal nerve.
*
Anterolateral Approach:
(Modified Watson-Jones)
*
Internervous Plane:
Between tensor fascia lata (superior gluteal nerve) and gluteus medius (superior gluteal nerve).
*
Advantages:
Allows for good anterior access.
*
Disadvantages:
Limited posterior exposure.
Step-by-Step Surgical Technique for Acetabular Impaction Grafting
-
Exposure and Component Removal:
- Incise skin and subcutaneous tissues according to the chosen approach.
- Carefully dissect through scar tissue, protecting vital neurovascular structures.
- Perform a capsulotomy and dislocate the femoral head.
-
Remove the loose or failed acetabular component and any associated cement or osteolytic membranes. This can be challenging in severely osteolytic cases.
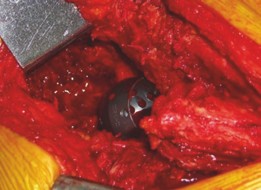
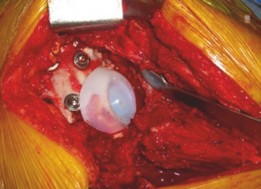
Intraoperative view after removal of the failed acetabular component, showing extensive bone loss and absence of a significant acetabular rim.
-
Debridement and Defect Preparation:
- Thoroughly debride all fibrous tissue, granuloma, necrotic bone, and remaining cement. Use curettes, osteotomes, and high-speed burrs.
- Bleeding cancellous bone should be exposed around the defect to maximize the potential for graft incorporation.
- Identify the extent and type of bone defect (e.g., Paprosky classification).
-
Containment of the Defect:
This is a crucial step.
- For contained cavitary defects (Paprosky II), the intact acetabular rim provides natural containment.
-
For uncontained segmental defects or those with significant rim loss (Paprosky III), external containment must be created. This can be achieved with:
- Antiprotruse Mesh/Wire Mesh: To reconstruct the medial wall if it is perforated or severely deficient, preventing graft migration into the pelvis.
- Reconstruction Plates: Bridge segmental defects or pelvic discontinuity.
-
Acetabular Reinforcement Rings or Cages:
(e.g., Burch-Schneider, Kerboull cages) provide structural support for large defects, especially in cases of medial wall protrusion or superior migration. They act as a scaffold to contain the graft and bear load.
An intraoperative image demonstrating the large acetabular defect following component removal and debridement, ready for impaction grafting.
-
Graft Preparation:
- Use thawed morselized cancellous allograft (typically femoral heads) processed to 3-10 mm particles. Smaller fragments may wash out, larger fragments may not compact well.
-
Ensure the graft is well-vascularized by allowing it to warm to body temperature and potentially rinsing it gently to remove cryopreservatives, though this is debated.

Morselized cancellous allograft, prepared and ready for impaction. Note the uniform size of the graft particles.
-
Impaction Grafting Technique:
- Start impaction from the periphery of the defect and work centrally.
- Use progressively larger impactors/tampers, starting with small spherical tampers and moving to hemispherical ones designed to recreate the acetabular contour.
- Layer-by-Layer Impaction: Apply small quantities of graft (e.g., 5-10 mL) and firmly impact each layer. Each layer should be compacted until no further movement of the tamper is observed.
- Restore Anatomy: The goal is to restore the normal acetabular contour, recreate the hip center of rotation, and provide a firm, stable bed for the new component.
-
Firmness Assessment:
The graft bed should feel as hard as cortical bone. A firm "thud" should be heard when impacting the final layers.

Initial stages of impaction grafting. A small tamper is used to carefully pack morselized allograft into the periphery of the defect, establishing a stable base.

Progression of impaction, demonstrating the build-up of the graft bed using larger, hemispherical tampers to reconstruct the acetabular dome and medial wall.
Final appearance of the impacted graft bed. It should be dense, smooth, and accurately recreate the anatomical contour and desired hip center of rotation.
-
Reconstruction Ring/Cage (if indicated):
- If a cage or ring is used, it is typically inserted after the initial impaction of morselized graft has established a foundational bed, but before the final impaction.
- The cage provides primary mechanical stability and containment for the graft. It should be positioned to bridge the defect and secured to healthy host bone with screws.
-
Once the cage is secured, further impaction grafting is performed around and through the cage fenestrations to fill any remaining voids and create a firm bed for the cemented polyethylene liner.

Placement of an acetabular reinforcement cage, secured with screws, providing structural integrity for a large defect. Morselized graft will be impacted within and around this cage.
-
Component Insertion:
- Cemented Polyethylene Liner: The standard approach with AIG is to cement a conventional polyethylene liner into the reconstructed graft bed. This provides a uniform load distribution across the graft.
- Cement Technique: Use contemporary cementing techniques, including pulsatile lavage, drying of the graft bed, and retrograde cement filling. A cement restrictor or plug is often used to prevent extravasation into the pelvis.
- Apply cement to both the graft bed and the exterior of the polyethylene liner.
- Impact the liner firmly into place, ensuring correct orientation and version. Remove excess cement.
-
Alternative: Uncemented Cup:
While less common with true impaction grafting, some surgeons use a large uncemented cup directly against a very robustly impacted graft, especially in Paprosky Type II defects where excellent peripheral host bone fixation can be achieved. However, the cemented liner is generally preferred for its proven track record in this technique.

The acetabular reinforcement cage is now in situ, secured with multiple screws to healthy host bone, creating a stable framework for the subsequent impaction of graft.

Following impaction of graft within and around the cage, cement is applied to the prepared bed, ensuring adequate interdigitation for the polyethylene liner.

The cemented polyethylene liner is now seated within the reinforced and grafted acetabulum, restoring the articular surface and hip center of rotation.
-
Trial Reduction and Stability Assessment:
- Perform a trial reduction with appropriate femoral components.
- Assess range of motion, stability in all planes (flexion, extension, rotation), and limb length.
- Ensure the femoral head is centered in the acetabulum and there is no impingement.
-
Definitive Femoral Component:
- If femoral revision is not required, ream and insert the definitive femoral stem.
- Perform final reduction.
-
Closure:
- Copiously irrigate the wound.
- Perform a meticulous repair of the capsule and external rotators (if a posterior approach was used) or abductor mechanism (if a direct lateral approach was used).
- Close fascial and subcutaneous layers.
- Place a drain if excessive bleeding is anticipated.
-
Close the skin.

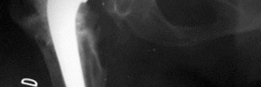
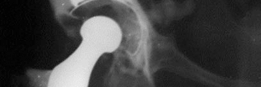
Post-operative anteroposterior radiograph demonstrating the well-fixed acetabular cage and cemented liner, with restoration of the hip center of rotation and leg length.
Lateral post-operative radiograph confirming satisfactory position and fixation of the acetabular components following impaction grafting and cage placement.
Complications & Management
Despite meticulous technique, revision THA with acetabular impaction grafting is associated with a specific set of complications, some unique to the technique. Proactive management and a clear salvage strategy are essential.
Intraoperative Complications
-
Periprosthetic Fracture:
- Incidence: Varies, especially common during component removal or aggressive reaming in osteoporotic bone.
- Management: Stable fractures can often be managed with cerclage wires or plates. If the fracture compromises component stability or graft containment, it must be addressed prior to or concurrently with impaction grafting. Consider a larger cage or structural allograft.
-
Neurovascular Injury:
- Incidence: Rare but devastating. Sciatic nerve (posterior approach), femoral nerve (anterior/anterolateral), obturator nerve (medial wall penetration).
- Management: Immediate recognition, exploration, and repair by a vascular or nerve specialist. Preventative measures include careful dissection, avoidance of excessive retraction, and cautious medial acetabular preparation.
-
Cement Extravasation:
- Incidence: Can occur with medial wall defects or through unsealed screw holes of a cage.
- Management: Carefully remove any extruded cement from the pelvis to prevent neurovascular irritation or compression. Ensure meticulous sealing of medial defects and screw holes during impaction.
-
Inadequate Graft Compaction/Unstable Graft Bed:
- Incidence: Technical error.
- Management: Re-impact the graft until a firm, stable bed is achieved. If unable to achieve stability, consider a larger or more robust reinforcement cage, or conversion to a structural allograft or custom component.
Early Post-Operative Complications
-
Periprosthetic Joint Infection (PJI):
- Incidence: 1-5% in revision THA, higher than primary.
- Management: Diagnosis via aspiration and cultures. Acute infections may be treated with debridement and implant retention (DAIR) in highly selected cases. Chronic infections typically require a two-stage exchange, with complete removal of all implants and graft, debridement, antibiotic spacer, and then revision with AIG in a second stage after infection eradication.
-
Dislocation:
- Incidence: Higher than primary THA (5-10%), due to compromised soft tissues, altered hip mechanics, and patient factors.
- Management: Closed reduction. For recurrent dislocations, consider component malposition (revision of acetabular or femoral component), soft tissue insufficiency (constrain liner, trochanteric advancement), or underlying neurological deficit.
-
Wound Complications:
- Incidence: Hematoma, seroma, dehiscence.
- Management: Aspiration or surgical drainage for hematoma/seroma. Debridement and re-closure for dehiscence.
-
Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE):
- Incidence: Varies with prophylaxis.
- Management: Anticoagulation. Prevention with mechanical and pharmacological prophylaxis.
Late Post-Operative Complications
-
Aseptic Loosening of the Acetabular Component:
- Incidence: The most common long-term failure mode for AIG, occurring in 5-15% at 10 years. Failure of graft incorporation, subsidence, or osteolysis can lead to loosening.
- Management: Revision THA. May require repeat AIG, structural allograft, or a custom component.
-
Graft Resorption / Osteolysis:
- Incidence: Can occur over time, especially with polyethylene wear or in areas of stress shielding.
- Management: Monitoring. If significant and symptomatic, may require revision.
-
Non-Union of Reconstruction Cage (if used):
- Incidence: Rare, but can occur with inadequate fixation or poor host bone quality.
- Management: Revision of the cage, often with supplemental plate fixation or a larger, custom implant.
-
Heterotopic Ossification (HO):
- Incidence: Common after revision THA, especially with extensive soft tissue dissection.
- Management: Prophylaxis with NSAIDs or radiation in high-risk patients. Symptomatic HO may require excision.
-
Fatigue Fracture of Acetabular Cage:
- Incidence: Rare, typically occurs in cases of persistent non-union or failure of graft incorporation, leading to excessive stress on the cage.
- Management: Revision of the cage, often with a more robust implant or structural allograft.
Complications and Management Table
| Complication | Incidence (Approximate) | Salvage Strategy / Management |
|---|---|---|
| Intraoperative | ||
| Periprosthetic Fracture (Acetabular) | 1-5% | Cerclage wiring, supplemental plate fixation, conversion to larger cage/structural allograft; if severe, consider custom triflange component. |
| Neurovascular Injury | <1% | Immediate recognition, surgical exploration, primary repair by specialist; meticulous dissection and retraction. |
| Cement Extravasation | 1-2% | Removal of extruded cement; careful defect sealing, cement restrictor, low-viscosity cement application. |
| Inadequate Graft Compaction | Technical | Re-impaction; consider adjunctive cage/plate; if persistently unstable, consider structural allograft or custom component. |
| Early Post-Operative | ||
| Periprosthetic Joint Infection (PJI) | 1-5% | Two-stage exchange (removal of all implants/graft, debridement, antibiotic spacer, then re-implantation with AIG in second stage); DAIR for acute infections in highly selected cases. |
| Dislocation | 5-10% | Closed reduction; if recurrent, assess component position (anteversion, inclination), offset, abductor function; consider revision of malpositioned components, constrained liner, or trochanteric advancement. |
| Wound Complications | 2-8% | Drainage of hematoma/seroma; debridement, re-closure for dehiscence; ensure meticulous hemostasis and wound closure. |
| DVT/PE | Variable | Anticoagulation (treatment dose); prevention with mechanical and pharmacological prophylaxis; early mobilization. |
| Late Post-Operative | ||
| Aseptic Loosening (Acetabular) | 5-15% (at 10 yrs) | Revision THA; repeat AIG, structural allograft, or custom component depending on bone loss pattern. |
| Graft Resorption / Osteolysis | 5-10% | Monitoring; if progressive and symptomatic, consider revision; address underlying cause (e.g., polyethylene wear). |
| Non-Union of Reconstruction Cage | <5% | Revision of cage, often with supplemental plate fixation or larger custom implant; ensure meticulous cage fixation to host bone initially. |
| Heterotopic Ossification (HO) | 10-30% | Prophylaxis with NSAIDs or radiation for high-risk patients; surgical excision for symptomatic, mature HO. |
| Fatigue Fracture of Acetabular Cage | <1% | Revision of the cage, often with a more robust design or conversion to a structural allograft; ensure robust initial fixation and graft incorporation. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following revision THA with acetabular impaction grafting is critical for successful graft incorporation, long-term implant survival, and functional recovery. The protocols are often more cautious than primary THA due to the biological nature of the graft and the inherent instability of bone loss.
General Principles
- Protection of Graft Healing: The primary goal in the early phase is to protect the impacted allograft bone while it undergoes revascularization and creeping substitution. This typically necessitates protected weight-bearing.
- Progressive Mobilization: Gradually increase activity levels to promote graft integration and muscle strengthening without overloading the construct.
- Range of Motion (ROM): Restore functional ROM while adhering to any necessary precautions to prevent dislocation.
- Pain Management: Effective analgesia is crucial for early mobilization and patient compliance.
Phased Rehabilitation Protocol
Phase 1: Immediate Post-Operative (Day 0 - Week 6)
*
Weight Bearing (WB):
*
Protected Weight Bearing (PWB):
Typically toe-touch weight bearing (TTWB) or 10-20% body weight for 6-12 weeks. This is crucial when a significant amount of graft was used or if a cage/ring was employed.
*
Rationale:
To allow graft compaction and primary mechanical stability to consolidate, promoting initial revascularization without excessive shear forces.
*
Assistive Devices:
Walker or crutches.
*
Range of Motion:
*
Precautions:
Adhere to standard hip precautions (e.g., no hip flexion > 90 degrees, no adduction past midline, no internal rotation for posterior approach; no external rotation for anterior approach) if a conventional liner is used.
*
Exercises:
Gentle ankle pumps, gluteal sets, quadriceps sets. Passive and active-assisted hip ROM within precautions.
*
Strengthening:
* Gentle isometric exercises (quads, glutes).
* Maintain core strength.
*
Functional Activities:
* Transfers, bed mobility, sit-to-stand training, gait training with protected WB.
*
Wound Care:
Monitor incision, drain removal.
*
DVT Prophylaxis:
Continue pharmacological and mechanical prophylaxis per institutional guidelines.
Phase 2: Intermediate (Week 6 - Week 12)
*
Weight Bearing:
*
Gradual Progression:
Advance from PWB to partial weight bearing (PWB 25-50% BW) as pain allows and radiographic signs of graft consolidation become evident.
*
Assistive Devices:
Progress from two crutches to one crutch or cane.
*
Range of Motion:
* Continue active and active-assisted ROM, respecting precautions.
* Gentle stretching of hip flexors and extensors.
*
Strengthening:
* Initiate isotonic strengthening exercises for hip abductors, adductors, flexors, and extensors (e.g., side-lying abduction, clam shells, knee bends, hip extension).
* Begin closed-chain exercises (mini-squats, weight shifts).
*
Functional Activities:
* Continue gait training, stair climbing practice.
* Begin light functional activities.
Phase 3: Advanced (Week 12 - Month 6)
*
Weight Bearing:
*
Full Weight Bearing (FWB):
Typically achieved around 12 weeks, provided radiographic signs of graft incorporation are satisfactory and the patient has good muscular control.
*
Assistive Devices:
Discontinue all assistive devices.
*
Range of Motion:
* Progress to full, pain-free ROM.
* Discontinue hip precautions if joint stability is confirmed and patient risk factors are low.
*
Strengthening:
* Progress to more challenging strengthening exercises for all hip muscle groups.
* Incorporate proprioceptive and balance training.
* Initiate light impact activities (e.g., fast walking, low-impact cardio) as appropriate.
*
Functional Activities:
* Return to light recreational activities.
* Focus on optimizing gait mechanics and endurance.
Phase 4: Return to Activity (Month 6 onwards)
*
Weight Bearing:
Full, unrestricted.
*
Strengthening:
Continue advanced strengthening and conditioning.
*
Return to Sport/High-Impact Activities:
* Gradual return to desired activities, typically low-impact (swimming, cycling, walking, golf).
* High-impact sports are generally discouraged due to increased risk of implant loosening and wear.
*
Long-Term Follow-up:
Regular clinical and radiographic follow-up to monitor graft integration, component stability, and detect any signs of loosening or osteolysis.

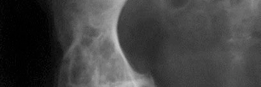
Radiographic follow-up at 6 months post-operatively showing progressive graft consolidation and early osteointegration around the cemented acetabular liner.

One-year post-operative radiograph indicating excellent graft incorporation with clear signs of host bone remodeling and persistent stable fixation of the acetabular components.
Two-year follow-up radiograph demonstrating continued bone remodeling and graft maturity, maintaining optimal position of the acetabular components.
Specific Considerations
- Radiographic Assessment: Serial radiographs are essential to monitor graft incorporation, subsidence, and any signs of impending failure. This often dictates the progression of weight-bearing.
- Patient Compliance: Patient education regarding the protected nature of the graft and the importance of adhering to weight-bearing restrictions is paramount.
- Pain: Pain levels guide activity progression. Unexplained or increasing pain warrants investigation for complications.
Summary of Key Literature / Guidelines
Acetabular impaction grafting has a rich history and a robust body of literature supporting its efficacy in managing severe acetabular bone loss in revision THA. It stands as a valuable biological reconstruction technique, especially for contained defects.
Landmark Studies and Historical Context
- Ling and Gie (Exeter group): Pioneered and popularized the modern technique of impaction grafting in the 1980s. Their initial work demonstrated the potential for biological reconstruction of acetabular defects using morselized allograft and cemented cups, showing promising long-term results. Their early series highlighted the importance of a firm graft bed and meticulous technique.
- Early Successes: Initial reports showed good to excellent results with survivorship rates of 80-90% at 10 years for Paprosky Type II defects, challenging the notion that bone loss required permanent structural prosthetic augmentation.
Outcomes and Survivorship
-
Contained Defects (Paprosky Type II):
Studies consistently report high long-term survivorship (80-90% at 10 years, 70-80% at 15 years) for revision THA using AIG for contained cavitary defects. These results are comparable to, and often superior to, those achieved with traditional uncemented cup revision for similar bone loss patterns, due to the bone stock restoration.
Long-term follow-up image (5 years) showing excellent graft integration and stability of the cemented acetabular cup, indicative of successful biological reconstruction. -
Uncontained Defects (Paprosky Type III, with Cages):
The use of AIG in conjunction with reinforcement rings or cages for more extensive, uncontained defects or pelvic discontinuity (Paprosky Type IIIA/IIIB) has also shown reasonable long-term results, although often with lower survivorship compared to contained defects (60-75% at 10 years). The cage provides immediate mechanical stability while the graft incorporates. The combination addresses both structural and biological deficiencies.

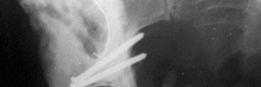
A different patient case, post-operative view demonstrating a Kerboull-type cage used in conjunction with impaction grafting for a complex defect, achieving anatomical restoration.

Another long-term follow-up (8 years) highlighting the successful integration of the cage and graft, with no signs of loosening or progressive bone loss.
This panoramic view shows the pelvic ring integrity and implant alignment, critical for long-term stability and functional outcome following complex revision THA.
Challenges and Limitations
- Graft Resorption/Osteolysis: While the aim is bone stock restoration, some degree of graft resorption can occur over time, especially in response to particulate wear debris. Long-term graft incorporation is variable.
- Mechanical Failure: Aseptic loosening remains the primary mode of failure. Inadequate impaction, poor host bone quality, or excessive initial loading can lead to graft subsidence or component loosening.
- Infection: Allograft bone is generally considered "dead" and less resistant to infection than living bone, making infection control paramount.
- Learning Curve: The technique requires a significant learning curve to achieve consistently good results, emphasizing the importance of specialized training and experience.
Evolving Techniques and Materials
- Uncemented Cups with AIG: While traditionally using cemented polyethylene, some surgeons are exploring uncemented cups directly fixed into robustly impacted graft beds, particularly with newer porous-coated cups designed for enhanced osteointegration. Long-term data for this approach are still evolving.
- Alternative Graft Materials: Research continues into various bone graft substitutes, but morselized cancellous allograft remains the gold standard due to its osteoconductive properties and biomechanical suitability for impaction.
-
3D Planning and Custom Implants:
Advanced 3D printing and planning can assist in pre-operative templating, especially for highly complex defects and custom acetabular components.

A detailed coronal view from a CT scan, used for advanced pre-operative planning, illustrating the residual bone stock and virtual placement of implants for optimal fit and function.
Guidelines and Recommendations
Current guidelines from major orthopedic societies often recommend AIG as a viable and preferred option for contained acetabular bone defects (Paprosky Type II) in revision THA. For uncontained defects (Paprosky Type III), the combination of AIG with a reinforcement cage or plate is a well-accepted reconstructive strategy, offering a biological approach to bone stock restoration. The choice between AIG and other techniques (e.g., structural allografts, custom triflange components) often depends on the extent and morphology of bone loss, patient factors, and surgeon expertise. The overriding principle remains the restoration of the hip center of rotation, reconstruction of bone stock, and achievement of stable, durable implant fixation.
Clinical & Radiographic Imaging