Acetabular Augment: Rebuilding Bone in Complex Revision
Introduction & Epidemiology
Acetabular bone loss in revision total hip arthroplasty (THA) represents one of the most formidable challenges encountered by orthopedic surgeons. The increasing volume of primary THA, combined with an aging patient population and extended implant longevity, has inevitably led to a rising incidence of revision procedures. Many of these revisions are characterized by significant acetabular defects, which compromise mechanical stability, impede biological fixation, and complicate reconstruction. Acetabular augments have emerged as critical tools in addressing these complex defects, allowing for the restoration of bone stock, recreation of a stable hip center, and provision of a robust platform for definitive acetabular component fixation.
The primary goals of employing acetabular augments are multifaceted: to restore the integrity of the bony acetabulum, to provide adequate support and containment for a hemispheric or custom acetabular component, to facilitate biological ingrowth, and ultimately, to achieve long-term implant stability and patient function. The spectrum of acetabular bone loss, as categorized by the Paprosky classification system, ranges from contained cavitary defects (Type I, IIA) to segmental defects with compromised rim integrity (Type IIB, IIC), and ultimately to severe forms involving pelvic discontinuity (Type III A/B, Type IV). While less severe defects can often be managed with oversized hemispheric cups and screw fixation, Paprosky Type IIB and higher defects frequently necessitate the use of bone graft and/or structural augments to provide the necessary support and improve long-term outcomes.
Epidemiologically, revision THA constitutes approximately 10-15% of all hip arthroplasty procedures, with a significant proportion involving some degree of acetabular bone loss. The specific use of augments varies by institution and surgeon preference but is increasingly prevalent as surgeons confront more severe and challenging cases. The evolution of augment materials, from bulk structural allografts to modular porous metal designs and, more recently, custom 3D-printed implants, reflects a continuous effort to optimize biological integration and mechanical stability in this demanding reconstructive environment. This guide aims to provide a comprehensive, high-yield overview of the indications, surgical techniques, and expected outcomes associated with acetabular augments in complex revision THA.
Surgical Anatomy & Biomechanics
A thorough understanding of acetabular surgical anatomy and biomechanics is paramount for successful acetabular reconstruction with augments.
Acetabular Anatomy
The acetabulum is formed by the confluence of the ilium, ischium, and pubis. Key anatomical landmarks critical for surgical planning and intraoperative orientation include:
*
True Acetabulum:
The articular cartilage-lined surface that articulates with the femoral head.
*
Acetabular Rim:
The bony circumference of the acetabulum, providing peripheral support for the acetabular component. Defects here are classified as segmental.
*
Columns:
The acetabulum is supported by two main columns:
*
Anterior Column:
Consists of the anterior ilium, anterior acetabular wall, and superior pubic ramus.
*
Posterior Column:
Comprises the posterior ilium, posterior acetabular wall, and ischium.
* Integrity of these columns is essential for pelvic stability. Defects or discontinuity of these columns (e.g., Paprosky Type III, IV) significantly compromise reconstruction.
*
Teardrop:
The inferomedial aspect of the acetabulum, a radiographic landmark formed by the anterior cortex of the ischium and the quadrilateral surface. Its integrity provides medial containment.
*
Kohler's Line:
A radiographic line corresponding to the medial aspect of the quadrilateral surface. Medial migration of the femoral head past this line indicates severe medial wall deficiency or protrusion.
*
Quadrilateral Surface:
The thin bone of the medial wall, between the teardrop and the iliopectineal line. Frequently deficient in protrusion defects.
Vascularity and Innervation
Understanding the neurovascular anatomy around the acetabulum is crucial for preventing iatrogenic injury.
*
Arterial Supply:
The acetabulum receives blood supply primarily from branches of the internal iliac artery, including the superior and inferior gluteal arteries, obturator artery, and occasionally branches of the medial and lateral femoral circumflex arteries. The integrity of this vascular supply is vital for bone graft incorporation and osseointegration of porous implants.
*
Nerves:
The sciatic nerve passes posterior to the acetabulum and is at significant risk during posterior approaches, especially with posterior column defects or screw placement. The obturator nerve and vessels are medial to the acetabulum and are vulnerable during medial reaming or penetration of the quadrilateral surface. The femoral nerve lies anterior and lateral to the iliopsoas muscle and can be at risk during anterior approaches or extensive anterior column reconstruction.
Biomechanics of the Pelvis and Bone Loss
The hip joint is subjected to significant load during daily activities, with joint reaction forces often exceeding several times body weight. The acetabulum dissipates these forces, maintaining stability and allowing mobility.
*
Hip Center:
The anatomical hip center provides optimal biomechanical advantage, minimizing joint reaction forces and maximizing abductor lever arm. Restoration of the hip center is a key objective in revision THA.
*
Bone Loss Patterns:
Acetabular bone loss patterns are classified by Paprosky:
*
Type I:
Minimal bone loss, intact rim and columns.
*
Type IIA (Cavitary, Contained):
Peripheral rim intact, superomedial wall deficient.
*
Type IIB (Segmental, Uncontained):
Superior rim deficient, columns intact.
*
Type IIC (Segmental, Uncontained):
Medial wall deficient (protrusio), columns intact.
*
Type IIIA (Columnar with Intact Pelvic Discontinuity):
Superior column defects, typically involving the anterior or posterior column, but pelvic ring remains intact.
*
Type IIIB (Columnar with Compromised Pelvic Discontinuity):
Severe columnar defects, often with a large medial wall defect.
*
Type Type IV (Pelvic Discontinuity):
Complete separation of the superior and inferior aspects of the acetabulum, indicating a structural failure of the pelvic ring. This is the most challenging defect to manage.
Augment Biomechanics
Acetabular augments are designed to restore lost bone stock, contain the definitive acetabular component, and transfer physiological loads to the remaining host bone.
*
Load Sharing:
Ideally, augments should share load with the host bone, preventing stress shielding and encouraging bone ingrowth.
*
Stability:
Initial mechanical stability of the augment and the definitive cup is paramount for osseointegration. Screw fixation into healthy host bone is crucial.
*
Reconstruction of Hip Center:
Augments allow for reconstruction of the anatomical hip center, which is vital for restoring abductor function, preventing impingement, and minimizing dislocation risk.
*
Biological Fixation:
Porous metal augments and structural allografts rely on bone ingrowth/incorporation for long-term stability. The biomechanical environment must be conducive to this process (e.g., micromotion below 150 µm).
Indications & Contraindications
The decision to utilize an acetabular augment is based on a comprehensive assessment of the extent and pattern of bone loss, the integrity of the remaining host bone, and patient-specific factors.
Indications for Acetabular Augments
Acetabular augments are primarily indicated in cases of significant acetabular bone loss where a standard hemispheric cup cannot achieve stable fixation or adequate coverage, or where structural support for the definitive component is compromised.
-
Severe Acetabular Bone Loss (Paprosky Classification):
- Paprosky Type IIB: Superior segmental defects involving the acetabular rim. Augments restore the superior rim to provide cup coverage and stability.
- Paprosky Type IIC: Medial wall defects (protrusion) where the quadrilateral surface is significantly compromised. Augments provide medial containment and prevent component migration.
- Paprosky Type IIIA and IIIB: Columnar defects involving either the anterior or posterior column, often with associated cavitary or segmental defects. Augments help bridge these defects and reinforce the columns.
- Paprosky Type IV (Pelvic Discontinuity): Complete separation of the superior and inferior hemi-pelvis. Augments are essential components of complex reconstruction strategies, often in conjunction with anti-protrusio cages or plates, to stabilize the fractured pelvis and provide a stable base.
- Containment of Revision Cup: When the remaining host bone cannot fully contain a revision cup (e.g., <70% coverage), augments extend the available bone surface.
- Restoration of Hip Center: To reposition a superolaterally migrated hip center back to its anatomical location, optimizing biomechanics and leg length.
- Failed Prior Reconstructions: Cases with failed bulk allografts, cages, or other revision constructs that have led to progressive bone loss.
- Impending Structural Failure: Extensive periacetabular osteolysis with impending fracture or collapse, even if not yet a frank discontinuity.
Contraindications for Acetabular Augments
While augments are powerful tools, certain conditions preclude their use or necessitate extreme caution.
-
Absolute Contraindications:
- Active Periprosthetic Joint Infection (PJI): The presence of active infection is an absolute contraindication for the implantation of any permanent hardware, including augments. A two-stage revision protocol is mandated, with augments only considered at the second stage after infection eradication.
- Uncontrolled Systemic Sepsis: Patients with systemic sepsis are not candidates for elective or semi-elective implant surgery.
-
Relative Contraindications:
- Insufficient Host Bone for Fixation: While augments address bone loss, there must be enough viable, healthy host bone to securely fix the augment itself. In extreme cases, a custom triflange acetabular component might be a more appropriate solution.
- Severely Compromised Soft Tissue Envelope: Poor soft tissue coverage or quality around the hip may increase the risk of wound complications and infection, making complex reconstructions less advisable.
- Patient Comorbidities: Uncontrolled medical comorbidities (e.g., severe cardiac disease, end-stage renal disease, uncontrolled diabetes) that significantly elevate surgical risk.
- Patient Non-compliance: Inability or unwillingness to adhere to post-operative weight-bearing restrictions and rehabilitation protocols, which are critical for augment integration and long-term success.
Summary Table: Indications for Acetabular Augments
| Indication Category | Operative (Augment Indicated) | Non-Operative (Augment NOT Indicated, Conservative Management or Alternative Surgical Options) |
|---|---|---|
| Acetabular Bone Loss Severity (Paprosky) | Type IIB, IIC, IIIA, IIIB, Type IV (segmental defects, medial wall defects, columnar defects, pelvic discontinuity). Large cavitary defects (Type IIA) sometimes benefit, especially if combined with significant containment issues. | Type I, Type IIA (contained defects) amenable to cementless cups with adequate host bone coverage and screw fixation, or impaction grafting alone for smaller cavitary defects. Minimal bone loss not affecting cup stability or coverage. |
| Pelvic Integrity | Identified pelvic discontinuity, significant anterior or posterior column defects compromising stability, large medial wall defects requiring structural support (e.g., protrusio acetabuli), failed anti-protrusio cages leading to further bone loss. | Intact pelvic ring, minor cavitary defects not compromising overall stability. |
| Infection Status | Eradicated Periprosthetic Joint Infection (PJI) , confirmed by cultures and inflammatory markers (two-stage revision protocol). | Active Periprosthetic Joint Infection (PJI) . Definitive augment placement must await complete infection eradication. |
| Functional Impairment | Significant pain, instability, recurrent dislocation, limb length discrepancy, or functional limitation directly attributable to acetabular bone loss and component instability. | Minimal symptoms, stable implant, minor bone loss not affecting stability or functional mechanics. Patients with non-surgical causes for pain or instability. |
| Patient Factors | Medically optimized, reasonable bone quality for screw fixation, willing and able to comply with post-operative rehabilitation. Adequate soft tissue envelope. | Medically unstable (unacceptable anesthetic risk), severe osteoporosis precluding stable screw fixation, non-compliant patient, severely compromised soft tissue envelope predisposing to wound complications. Patients with limited life expectancy where a less invasive approach would suffice. |
| Previous Reconstructions | Failed structural allografts with resorption/non-union, failed cages or cup-cage constructs with progressive bone loss, recurrent aseptic loosening despite prior revision attempts. | Stable previous revisions without progressive bone loss or implant failure. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is the cornerstone of a successful complex acetabular revision with augments.
Pre-Operative Imaging
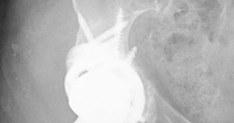
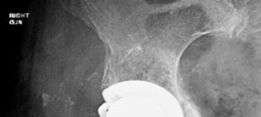
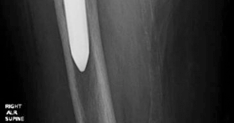
- Standard Radiographs: Anteroposterior (AP) pelvis, frog-leg lateral, and a true lateral of the affected hip are essential. These provide initial assessment of component position, subsidence, osteolysis, and general bone architecture. Stress views may be helpful for suspected pelvic discontinuity.
-
Computed Tomography (CT) Scan with 3D Reconstructions:
This is indispensable for severe defects (Paprosky Type III and IV).
- Precise Assessment: CT allows for detailed visualization of the extent and morphology of bone loss, identification of specific columnar defects, quantification of medial wall integrity, and assessment of pelvic discontinuity.
- Measurement: Accurate measurements for cup size, augment dimensions, and screw length are obtained.
- Neurovascular Mapping: Identifies the proximity of critical neurovascular structures (e.g., sciatic nerve, external iliac vessels) relative to potential screw trajectories.
- Templating: 3D models from CT data can be used for advanced digital templating or even for the fabrication of custom 3D-printed guides or implants.
- Magnetic Resonance Imaging (MRI): May be indicated if soft tissue pathology, occult infection, or tumor is suspected, though less critical for bone loss assessment directly.
- PET/CT or Bone Scans: Used in conjunction with serological markers (ESR, CRP) to rule out occult infection if suspicion is high.
Templating and Surgical Simulation
- Digital Templating Software: Utilizing software such as TraumaCad, OrthoView, or similar platforms allows for virtual placement of revision cups and augments. This helps determine optimal cup size, inclination, anteversion, and reconstruct the hip center.
- Augment Sizing and Placement: Templating aids in selecting the appropriate size and geometry of modular augments (e.g., wedges, hemispherical pieces, customized shapes) and planning their exact placement and screw fixation trajectories.
- Custom 3D-Printed Implants: For extreme Paprosky Type IIIB or Type IV defects, patient-specific 3D-printed titanium implants may be planned. This involves a collaborative process with the implant manufacturer based on the patient's CT data, leading to a truly custom fit.
Patient Optimization
- Medical Clearance: Thorough medical evaluation by an internist or cardiologist to optimize co-morbidities.
- Anemia Correction: Pre-operative iron supplementation or erythropoietin may be required to optimize hemoglobin levels, reducing the need for intraoperative transfusion.
- Nutritional Status: Assess and optimize nutritional parameters (e.g., serum albumin, prealbumin), as malnutrition can impair wound healing and bone ingrowth.
- Infection Workup: If suspicion for PJI exists (elevated ESR/CRP, prior history of infection), joint aspiration with cell count, differential, and cultures is mandatory. A two-stage approach is typically required for active PJI.
- DVT Prophylaxis: A comprehensive DVT prophylaxis plan, tailored to the patient's risk factors, should be established.
Equipment Preparation
- Ensure availability of a full revision instrument set, including specialized acetabular reamers (variable sizes, offset reamers), cement removal tools, osteotomes, and a high-speed burr.
- A wide array of acetabular augments (e.g., Trabecular Metal, porous titanium, different sizes and geometries), revision acetabular components, and various lengths and diameters of locking and non-locking screws must be on hand.
- Bone graft material: Allograft (morselized, structural femoral heads), autograft (if available and indicated), or synthetic bone graft substitutes.
- Intraoperative fluoroscopy (C-arm) is essential for confirming component position, augment placement, and screw trajectory.
Patient Positioning
- Lateral Decubitus Position: This is the most common position for revision THA, allowing excellent access to both the acetabulum and proximal femur.
- Padding: Meticulous padding of all pressure points (axilla, contralateral knee, ankles, perineum) is crucial to prevent nerve palsies and skin breakdown.
- Secure Fixation: The patient must be securely fixed to the operating table with a beanbag or sacral supports to prevent intraoperative movement, especially during reaming and impaction.
- C-arm Access: Ensure unrestricted C-arm access for intraoperative imaging, typically in AP and lateral planes.
- Preparation and Drape: The surgical field should be prepped and draped to allow for wide exposure and potential extension of the incision if needed. Mark critical bony landmarks (ASIS, greater trochanter) and plan the skin incision.
Detailed Surgical Approach / Technique
The surgical technique for implanting acetabular augments in complex revision THA demands precision, meticulous attention to bone preservation, and a systematic approach to reconstruction.
Approach Selection
- Posterior (Kocher-Langenbeck) Approach: This is the most widely utilized approach for revision THA due to its excellent exposure of the posterior acetabulum, sciatic nerve, and proximal femur. It allows for broad access to the true acetabulum and is versatile for addressing most defect patterns.
- Anterolateral (Hardinge) Approach: May be preferred by some surgeons, offering good exposure of the anterior and superior acetabulum. However, it can be more challenging for severe posterior bone loss or femoral component revision.
- Direct Anterior (DA) Approach: Less commonly used for complex revision with augments due to limited exposure for significant acetabular defects, particularly posterior and inferior. Its utility is generally reserved for less complex revisions or specific anterior pathology.
- Trochanteric Osteotomy: A greater trochanteric osteotomy may be indicated in cases of severe proximal femoral deformity, challenging exposure, retained well-fixed femoral components, or for facilitating safe removal of extensive cement or implants. This provides extensive access but carries its own set of complications.
Dissection & Exposure
- Skin Incision and Soft Tissue Dissection: The existing incision is typically utilized. Careful dissection through scar tissue, identifying and preserving neurovascular structures. The deep fascia (fascia lata for posterior/anterolateral approach) is incised.
- Muscle Release: For a posterior approach, the short external rotators (piriformis, gemelli, obturator internus, quadratus femoris) are detached from the greater trochanter, ensuring the sciatic nerve is identified and protected. The posterior capsule is released.
-
Explantation:
The existing acetabular component, any cement mantle, and osteolytic membrane or fibrous tissue are meticulously removed. Use of specialized explantation tools, osteotomes, and a high-speed burr may be necessary. Ensure all foreign material is removed, leaving a clean, bleeding bone bed.
-
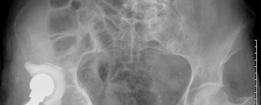
- This image might depict a large acetabular defect after explantation, highlighting the extent of bone loss.
-
Acetabular Preparation & Bone Grafting
- Defect Assessment and Debridement: Following explantation, the extent of the acetabular bone loss is meticulously assessed and correlated with pre-operative imaging. All remaining fibrous tissue, cement, and sclerotic bone are debrided to expose healthy, bleeding host bone.
- Reaming: Reaming aims to create a hemispherical cavity in the remaining host bone. Start with small reamers and progressively increase size, aiming to medialize the hip center where possible, while respecting the boundaries of the remaining intact bone. Avoid over-reaming, which can compromise precious host bone.
-
Bone Grafting (as needed):
- Cavitary Defects: Morselized allograft (or autograft if available) is typically impacted into cavitary defects (e.g., Paprosky Type IIA) to restore bone stock and provide a biologic scaffold for ingrowth.
- Segmental Defects/Medial Wall: Structural allograft (e.g., femoral head) may be used to reconstruct larger segmental defects or medial wall deficiencies, particularly if a metal augment is not ideal or available for that specific morphology.
-
- This image could show the process of impaction grafting or the placement of a structural allograft to fill a defect.
Augment Selection & Placement
-
Augment Type:
- Modular Porous Metal Augments: These are increasingly preferred due to their immediate mechanical stability and propensity for bone ingrowth. They come in various shapes (wedges, hemispheres, quadrants) and sizes, often made of highly porous titanium (e.g., Trabecular Metal, tantalum).
- Structural Allografts: Bulk femoral head allografts can be shaped and fixed with screws to reconstruct large defects. They have a higher risk of non-union or resorption but provide a biological reconstruction. They are often used in conjunction with cages or metal augments.
- Custom 3D-Printed Implants: For rare, extreme defects (Paprosky IIIB/IV) where modular augments cannot restore anatomy, custom implants can be fabricated to precisely match the patient's anatomy.
-
- This image might display a selection of modular metal augments, showcasing their various shapes and sizes, or instruments for their manipulation.
-
Positioning:
The augment is positioned to:
- Restore the deficient acetabular rim or wall.
- Provide a stable, contained bed for the definitive acetabular cup.
- Restore the anatomical hip center and offset.
- Ensure maximal contact with healthy host bone for optimal fixation and ingrowth.
-
- This image could illustrate an augment being carefully placed or trialed within the acetabular defect.
Fixation of the Augment
-
Screw Fixation:
Augments are typically fixed with multiple cancellous or cortical screws.
- Screws should achieve bicortical purchase where safely possible, avoiding neurovascular structures.
- Divergent screw trajectories enhance stability.
- Fluoroscopic guidance is often invaluable to ensure safe and adequate screw length and trajectory, particularly in the anterior-superior (near external iliac vessels) and posterior (near sciatic nerve) quadrants.
-
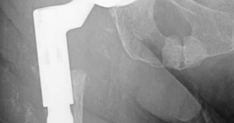
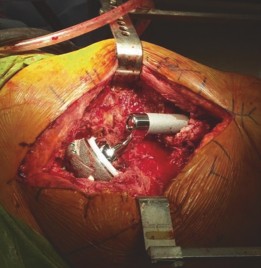- This image likely shows an acetabular augment securely fixed with multiple screws into the host bone.
Definitive Acetabular Component Implantation
-
Reaming for the Cup:
Once the augment is stable, the entire construct (augment + remaining host bone) is reamed to the desired size and orientation for the definitive acetabular component.
- The aim is to achieve a press-fit of the cup into the reamed bed, ensuring stability and contact for osseointegration.
-
- This image might depict the reaming of the acetabulum, post-augment fixation, to prepare for the definitive cup.
-
Trial Reduction:
Trial cups and femoral heads are used to assess stability, range of motion, leg length, and offset. Adjustments can be made at this stage.
-
- This image could show a trial acetabular cup in place, assessing fit and coverage.
-
-
Final Cup Implantation:
A highly porous acetabular cup, often with additional screw holes, is impacted into the prepared bed. Screws are placed through the cup into the host bone and/or augment for enhanced primary stability.
-
- This image likely illustrates the final acetabular component being implanted or fully seated.
-
Trial Reduction, Leg Length, and Offset
- After definitive component placement, perform a thorough trial reduction using appropriate trial heads and necks.
- Assess stability throughout a full range of motion, ensuring no impingement or dislocation.
- Carefully assess leg length discrepancy and femoral offset. Adjustments to femoral component choices (e.g., modular necks) or head length may be necessary.
Closure
- Irrigation and Hemostasis: Thorough irrigation to remove debris, followed by meticulous hemostasis.
- Drainage: Suction drains may be placed if significant bleeding is anticipated.
-
Layered Closure:
The deep fascia and muscle layers are carefully repaired to restore anatomical planes and provide soft tissue coverage. Subcutaneous tissues and skin are closed in layers.
-
- This image could be a post-operative radiograph showcasing the completed reconstruction with an augment and revision cup. -
- Another post-operative X-ray providing a different view or illustrating a similar case. -
- A close-up radiographic view highlighting the augment and its screw fixation, along with the acetabular cup. -
- An example of a particularly complex reconstruction, potentially involving a larger augment or cage. -
- A final illustrative image, possibly demonstrating long-term follow-up or a specific technical detail.
-
Complications & Management
Complex acetabular revision with augments carries a higher risk of complications compared to primary THA due to the extensive surgical dissection, compromised bone stock, and often, the patient's co-morbidities.
Common Complications
-
Intraoperative:
- Hemorrhage: Significant blood loss is common; prepare for transfusion and consider cell saver.
- Neurovascular Injury: Sciatic nerve (posterior approach), femoral nerve (anterior approach), obturator nerve/vessels (medial reaming/screw placement), external iliac vessels (anterior-superior screw placement).
- Acetabular Fracture: Intraoperative fracture of the remaining host bone or pelvis, particularly with aggressive reaming or component impaction.
- Difficulty with Implant Seating/Fixation: Due to insufficient bone or unexpected defect morphology.
-
Early Postoperative (within 30 days):
- Periprosthetic Joint Infection (PJI): A devastating complication, incidence higher in revision.
- Dislocation: Due to soft tissue imbalance, malposition of components, or patient non-compliance.
- Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE): Increased risk in complex hip surgery.
- Wound Healing Issues: Hematoma, seroma, superficial infection, dehiscence.
- Periprosthetic Fracture: Postoperative acetabular or femoral fracture.
-
Late Postoperative (>30 days):
- Aseptic Loosening: Of the augment, the acetabular component, or both. This is the most common mode of failure.
- Non-union/Resorption of Allograft: If structural allograft was used, failure of incorporation can lead to subsidence or loosening.
- Heterotopic Ossification (HO): Aberrant bone formation around the hip, potentially limiting range of motion.
- Progressive Bone Loss: Continued osteolysis or stress shielding around the implant.
- Nerve Palsy: Persistent or delayed onset of nerve dysfunction.
- Limb Length Discrepancy: Despite efforts to restore leg length intraoperatively.
- Recurrent Instability: Even without overt dislocation.
Summary Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (%) (approx.) | Salvage Strategy |
|---|---|---|
| Aseptic Loosening (Augment/Cup) | 5-15% at 5-10 years | Revision surgery: Explantation of loose components, extensive debridement, re-augmentation (if bone loss has progressed), impaction grafting, use of larger or constrained components, or custom triflange implants in severe cases. Focus on achieving biological fixation through host bone ingrowth or cementation where appropriate. |
| Periprosthetic Joint Infection (PJI) | 1-5% | Two-stage exchange: Explantation of all implants, extensive debridement, placement of antibiotic-loaded cement spacer, systemic antibiotic therapy (6-12 weeks), followed by reimplantation of new components after infection markers normalize. In select cases, one-stage exchange may be considered. Salvage with chronic suppressive antibiotics or resection arthroplasty if further surgery is not feasible. |
| Dislocation | 2-10% | Closed reduction if possible. If recurrent: investigation for component malposition (XR, CT), soft tissue imbalance, or impingement. Management options include: revision of malpositioned components, exchange to a larger femoral head, use of a constrained liner or dual mobility construct, trochanteric advancement, or abductor repair. |
| Periprosthetic Fracture (Acetabulum) | <1% (intra-op), 1-2% (post-op) | Intraoperative: Immediate fixation with plates/screws, adjustment of augment/cup size, use of cement, or larger reconstructive implants. Postoperative: Non-weight-bearing (NWB) immobilization, surgical fixation (ORIF) with plates/screws for unstable fractures, or formal revision if the fracture compromises implant stability. |
| Nerve Palsy (e.g., Sciatic, Femoral) | 1-3% | Observation: Most nerve palsies resolve spontaneously within 6-12 months. Neurophysiology studies: EMG/NCS to assess severity. Nerve decompression: If severe or progressive deficit is noted. Bracing/Assistive devices: To manage foot drop or quadriceps weakness. |
| Heterotopic Ossification (HO) | 10-20% (clinical), up to 50% (radiographic) | Prophylaxis: Indomethacin or single-dose post-operative radiation therapy, especially for high-risk patients (history of HO, ankylosing spondylitis). Surgical excision: If HO is mature and causing significant functional limitation (e.g., impingement, severely restricted ROM). |
| Non-union/Resorption of Allograft | 5-20% (for structural allograft) | Revision surgery: Explantation of non-united allograft, thorough debridement, re-grafting, use of metal augments or cages for structural support, with robust screw fixation. Extended protected weight-bearing post-operatively. Bone stimulators may be considered. |
| Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE) | DVT: 5-10%, PE: <1% | Anticoagulation: Therapeutic anticoagulation (e.g., LMWH, DOACs). IVC filter: For recurrent PE despite adequate anticoagulation or in patients with contraindications to anticoagulation. Early mobilization and mechanical prophylaxis. |
| Limb Length Discrepancy (LLD) | Variable | Conservative: Heel lifts for minor LLD (<1-1.5 cm) if symptomatic. Surgical revision: For significant symptomatic LLD refractory to conservative measures, involves adjusting component lengths (femoral neck, head) or considering osteotomies, though this is rare after complex revision with augments where reconstruction of the hip center is prioritized. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following complex acetabular revision with augments is crucial for successful integration of the augment, osseointegration of the acetabular component, and restoration of function. Protocols must be individualized based on the surgical findings, type of augment, quality of host bone, and achieved intraoperative stability.
Immediate Post-Operative Phase (Days 0-7)
- Pain Management: Aggressive multi-modal analgesia to facilitate early mobilization.
- DVT Prophylaxis: Continue chemical (anticoagulants) and mechanical (compression devices) prophylaxis.
-
Weight-Bearing (WB) Restrictions:
This is the most critical aspect.
- Non-Weight-Bearing (NWB) or Touch-Down Weight-Bearing (TDWB) (10-15 kg): Typically prescribed for 6-12 weeks, especially with large structural allografts, significant bone grafting, Paprosky Type IV defects, or when primary stability of the augment/cup is a concern. The goal is to protect bone ingrowth and allograft incorporation.
- Protected Weight-Bearing (PWB): In cases with excellent primary stability and strong host bone, PWB with crutches or a walker may be initiated, gradually progressing.
- Hip Precautions: If a posterior approach was used, standard hip precautions (avoiding hip flexion >90°, adduction past midline, and internal rotation) are maintained to prevent dislocation.
- Early Mobilization: Out of bed to chair and short ambulation with assistive devices, respecting WB restrictions.
- Gentle Range of Motion (ROM): Initiate gentle, protected active and passive ROM exercises within prescribed limits.
- Muscle Activation: Isometric exercises for gluteal muscles (quad sets, gluteal sets) to prevent atrophy.
Early Phase (Weeks 2-6)
- Continued WB Restrictions: Adherence to NWB/TDWB or PWB is paramount.
- Progressive ROM: Gradually increase the range of motion of the hip, avoiding extreme positions.
- Gentle Strengthening: Initiate gentle strengthening exercises, such as supine hip abduction, flexion, and extension within pain limits and precautions. Focus on core stability.
- Gait Training: Continue gait training with emphasis on proper technique with assistive devices, avoiding compensatory patterns.
Mid Phase (Weeks 6-12)
- Radiographic Assessment: Obtain follow-up radiographs to assess early signs of osseointegration, allograft incorporation, and implant stability.
- Progression of Weight-Bearing: Based on radiographic findings and clinical stability, gradually progress to Partial Weight-Bearing (PWB) and then Weight-Bearing As Tolerated (WBAT). This transition is often phased over several weeks.
- Increased Strengthening: Advance strengthening exercises with increased resistance (resistance bands, light weights) for hip abductors, adductors, extensors, and flexors.
- Proprioceptive Training: Balance exercises to improve neuromuscular control.
- Stair Training: Begin stair negotiation training with appropriate assistance.
Late Phase (Weeks 12+)
- Full Weight-Bearing (FWB): Once radiographic evidence of stable osseointegration (e.g., absence of lucencies, evidence of bone ingrowth) and clinical stability are achieved, full weight-bearing can be initiated.
- Advanced Strengthening: Progress to advanced strengthening and conditioning, including closed-chain exercises.
- Functional Training: Focus on functional activities relevant to the patient's daily life.
- Return to Activity: Gradual return to light activities and low-impact sports, avoiding high-impact activities (running, jumping sports) indefinitely.
- Long-Term Follow-up: Regular clinical and radiographic follow-up is necessary to monitor implant stability, identify progressive bone loss, or detect late complications.
Note: For structural allografts, NWB or TDWB may be extended up to 3-6 months to allow for robust allograft incorporation and remodeling. Any signs of impending failure (e.g., increasing pain, implant subsidence, increasing lucency zones on X-ray) necessitate immediate re-evaluation and potential modification of the rehabilitation plan.
Summary of Key Literature / Guidelines
The landscape of acetabular augments in complex revision THA is continuously evolving, supported by a growing body of literature. The Paprosky classification remains the universally accepted standard for characterizing acetabular bone loss, guiding surgical planning and dictating reconstructive strategies.
Paprosky Classification and Treatment Algorithms
The Paprosky classification system (1994) is fundamental. Studies consistently demonstrate that increasing Paprosky grades correlate with increased surgical complexity, longer operative times, higher complication rates, and potentially lower long-term survivorship. Current guidelines emphasize the need for robust structural support and biological fixation for Paprosky Type IIB, IIC, III, and IV defects.
Modular Metal Augments
-
Porous Titanium/Tantalum (Trabecular Metal):
Numerous studies have demonstrated excellent mid- to long-term results with modular porous metal augments. These implants benefit from their highly porous architecture, which mimics cancellous bone, allowing for rapid bone ingrowth and high rates of osseointegration.
- Head et al. (2006, 2011) presented early positive outcomes with Trabecular Metal augments in complex revisions, showing high rates of implant stability and bone ingrowth.
- Lacroix et al. (2018) reviewed a multicenter series, reporting survivorship of Trabecular Metal augments around 90-95% at 5-10 years, emphasizing their efficacy in bridging defects and providing a stable platform for definitive cup fixation.
- The biomechanical advantage lies in their high friction coefficient for immediate stability and interconnected pore structure for biological fixation. They offer a strong alternative to bulk allografts, with significantly lower rates of non-union and resorption.
Structural Allografts
-
Historically,
bulk structural allografts (e.g., femoral head allografts)
were a mainstay for large acetabular defects. However, long-term studies highlighted significant limitations:
- High Rates of Resorption and Non-union: Studies by Gie et al. (1993) and Lynch et al. (2006) reported non-union rates ranging from 15-30% and subsequent aseptic loosening rates. Allografts rely on creeping substitution, a slow and often incomplete process.
- Disease Transmission Risk: Although rare, the potential for disease transmission remains a concern.
- Current use of structural allografts is often limited to filling large cavitary defects or as a biological filler in combination with metal augments or cages, rather than as primary structural support. They are rarely used as standalone structural elements in modern practice due to the superior mechanical and biological performance of porous metal augments.
Custom 3D-Printed Implants
-
Emerging Technology:
For extremely complex Paprosky Type IIIB and Type IV defects, especially with significant pelvic discontinuity or severe bone loss where standard modular augments are insufficient,
custom 3D-printed titanium implants
are gaining traction.
- These implants are patient-specific, designed from pre-operative CT scans to perfectly match the unique anatomy and defect morphology. This precise fit can theoretically optimize load transfer and bone ingrowth.
- Windsor et al. (2018) and Sporer et al. (2020) have published early series demonstrating promising results, with high rates of initial stability and good functional outcomes.
- Advantages: Excellent anatomical restoration, potentially reduced intraoperative time for shaping, and optimal initial stability.
- Limitations: High cost, extended manufacturing lead time, and a relative lack of long-term outcome data compared to modular systems. Their use is typically reserved for cases where conventional methods are deemed inadequate.
Pelvic Discontinuity Management
-
Paprosky Type IV defects (pelvic discontinuity)
represent the most severe challenge. The literature supports a reconstructive approach that aims to stabilize the discontinuity first, then reconstruct the acetabulum.
- Techniques include plates across the discontinuity (e.g., hook plates, reconstruction plates), anti-protrusio cages (e.g., Kerboull, Burch-Schneider), and increasingly, modular metal augments used in conjunction with these systems or custom triflange implants.
- Studies by Berry et al. (2005) and Jahng et al. (2018) highlight the improved outcomes achieved with stable fixation of the discontinuity, often involving posterior column plating, and a well-fixed revision cup. Modular augments play a crucial role by bridging defects and providing a robust platform for cup fixation within the stabilized pelvic frame.
Outcomes and Future Directions
Overall, the use of acetabular augments in complex revision THA has improved patient outcomes, with reported survivorship rates generally ranging from 80-95% at 5-10 years, considering the challenging nature of these cases. The choice of augment depends heavily on the defect morphology and surgeon experience.
Future directions include further advancements in biomaterials with enhanced osteoinductive properties, improved integration of virtual surgical planning and robotic assistance for precise implant placement, and continued development of patient-specific implants to tackle the most intractable bone loss scenarios. Continued research is needed to refine indications, optimize surgical techniques, and provide robust long-term data for these advanced reconstructive options.
Clinical & Radiographic Imaging