Introduction to the Restoration of Pinch
The evolutionary advantage of the human hand is inextricably linked to the opposability of the thumb. Opposition is the cornerstone of pinch—one of the three most critical functions of the hand, alongside power grip and hook grip. Frequently, the capacity for opposition is either partially or totally lost secondary to median nerve palsy, severe brachial plexus injuries, or anterior horn cell diseases such as poliomyelitis.
Successful restoration of pinch requires a profound understanding of hand biomechanics. Opposition depends primarily on the function of the intrinsic muscles of the thumb, with the abductor pollicis brevis (APB) serving as the primary kinematic driver. However, intrinsic function alone is insufficient; extrinsic muscles are equally necessary to dynamically stabilize the metacarpophalangeal (MCP) and interphalangeal (IP) joints of the thumb. Without this extrinsic stabilization, the forces generated during pinch would result in joint collapse, necessitating surgical arthrodesis or tenodesis to provide a rigid post against which the fingers can articulate.
Biomechanics and Kinematics of Thumb Opposition
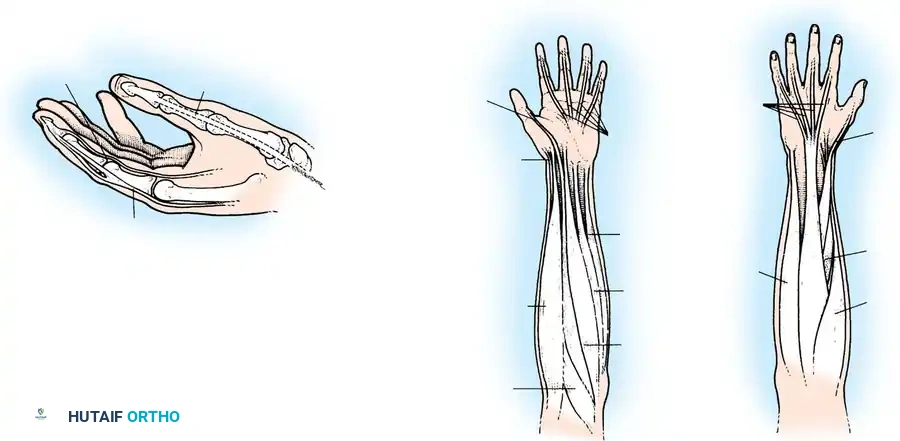
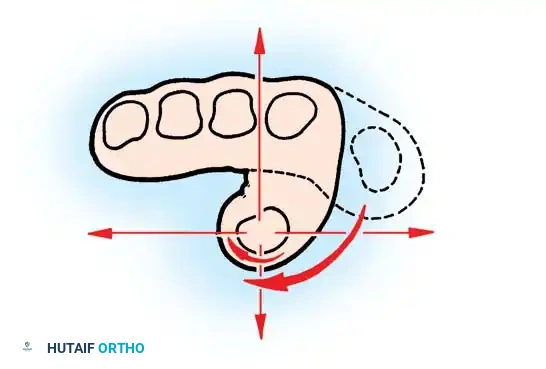
Opposition of the thumb is not a single, isolated movement but rather a highly complex, multi-planar motion achieved through the precise coordination of several distinct biomechanical events:
- Abduction of the thumb away from the palmar surface of the index finger.
- Flexion of the metacarpophalangeal (MCP) joint of the thumb.
- Internal rotation (pronation) of the thumb metacarpal at the trapeziometacarpal joint.
- Radial deviation of the proximal phalanx of the thumb on the metacarpal.
- Dynamic translation of the thumb toward the volar aspect of the fingers.
Although opposition is the culmination of coordinated function among all long and short muscles acting on the thumb, the abductor pollicis brevis is the most important single muscle participating in this complex movement. It internally rotates and abducts the thumb away from the index metacarpal, internally rotates and abducts the proximal phalanx on its metacarpal, and synergistically assists the extensor pollicis longus (EPL) in extending the interphalangeal joint.
For these biomechanical reasons, pioneers in hand surgery such as Littler and Riordan established the fundamental principle that, when restoring opposition via tendon transfer, the transferred tendon must be inserted directly into the tendon of the abductor pollicis brevis to replicate its exact vector of pull.
Principles of Tendon Transfer for Opponensplasty
The success of any tendon transfer relies on matching the physiological parameters of the donor muscle to the requirements of the deficient function. Two critical factors must be evaluated: Amplitude of Excursion and Muscle Power.
Amplitude of Excursion
The donor tendon must possess sufficient excursion to allow full range of motion.
According to Curtis (1974), the natural amplitudes of key tendons are as follows:
* Flexor digitorum profundus (FDP): 70 mm
* Flexor digitorum sublimis (FDS): 64 mm
* Extensor pollicis longus (EPL): 58 mm
* Flexor pollicis longus (FPL): 52 mm
* Extensor digitorum communis (EDC): 50 mm
* Wrist extensors and flexors: 33 mm
* Abductor pollicis longus (APL) / Extensor pollicis brevis (EPB): 28 mm
Because the required excursion for thumb opposition is significant, wrist tendons (33 mm) are generally insufficient without extensive mobilization, whereas the FDS (64 mm) provides an ideal amplitude match.
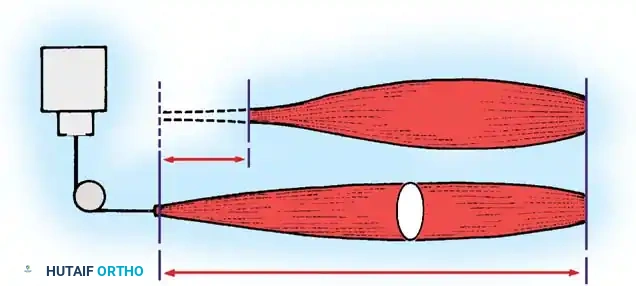
Muscle Power and Working Capacity
The working capacity of a muscle is defined by the equation W = F × d, where F (force) equals the absolute muscle power (calculated as 3.65 × cm² of physiological cross-section), and d (distance) equals the amplitude or displacement.
Surgical Pearl: A transferred tendon cannot be expected to glide properly when it crosses raw bone, passes through unyielding fascia without a sufficient opening, or is buried within scarred tissue. With very few exceptions, transferred tendons must be passed subcutaneously through healthy, pliable adipose tissue.
The Necessity of a Pulley
To replicate the vector of the APB, the transferred tendon must approach the thumb from the ulnar side of the wrist or palm. This necessitates the creation of a pulley. While a pulley redirects the force vector appropriately, the surgeon must remember that the mechanical efficiency of the donor muscle is inherently diminished by friction at the pulley site.
Some surgeons prefer a static pulley created by making a loop at the distal end of the flexor carpi ulnaris (FCU) tendon, whereas others advocate for a dynamic pulley formed by looping the transfer around the intact FCU tendon.
Preoperative Evaluation and Correction of Thumb Deformity
To restore function properly, any pre-existing deformities or contractures must be corrected before or during the opponensplasty. A transferred tendon will never overcome a fixed bony or soft-tissue contracture.
Substitution Patterns
In the paralytic hand, patients often develop substitution patterns to achieve a rudimentary pinch. As a substitute for opposition, adduction of the thumb by the long thumb extensor (EPL) frequently becomes a habit.
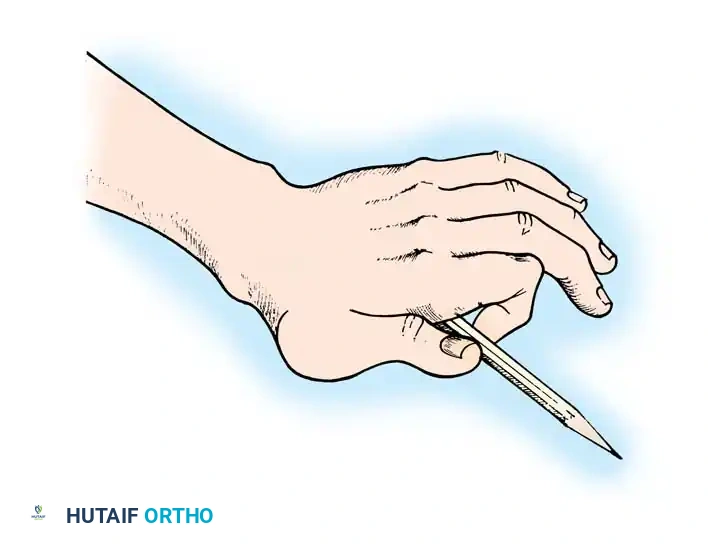
In these instances, adduction and extension occur as a single function: the flexed tip of the thumb is brought against the base of the proximal phalanx of the index finger by the pull of the EPL toward Lister's tubercle. Pinch occurs at the base of the finger instead of the tip. To pick up an object, the patient must rotate the point of contact downward by pronating the wrist, elevating the elbow, and abducting the shoulder. Over time, the EPL tendon gradually migrates into the web space, acting purely as an adductor.
Contracture Release and Joint Stabilization
- Web Space Contracture: Any fixed adduction and external rotational deformity must be corrected. This is usually accomplished by dividing the fascia in the web space between the index and thumb metacarpals and performing subperiosteal stripping of the ulnar side of the first metacarpal (as recommended by Goldner and Irwin). Severe deformities may require a Z-plasty of the web space.
- Carpometacarpal (CMC) Joint: The CMC joint must be freely movable. If the deformity is so severe that it cannot be corrected by soft-tissue release, arthrodesis of the first CMC joint may be indicated. Alternatively, if mobility is prioritized over stability, excising the trapezium can release the soft tissues enough to make arthrodesis unnecessary.
- Metacarpophalangeal (MCP) Joint: Arthrodesis of the MCP joint is indicated if available muscle power is insufficient to stabilize it dynamically, or if the joint is rendered unstable by capsular laxity. The joint should be arthrodesed in 15 degrees of flexion and slight internal rotation.
- Interphalangeal (IP) Joint: Occasionally, arthrodesis of the IP joint is required for a fixed flexion contracture. The optimal position is 20 degrees of flexion.
Motor Selection Hierarchy
The proper muscle for a motor is selected only after a meticulous evaluation of the strength of the remaining musculature in the hand.
- Flexor Digitorum Sublimis (FDS) of the Ring Finger: This is the absolute muscle of choice. It possesses excellent amplitude, adequate power, and its removal causes minimal donor site morbidity, provided the associated FDP is strong enough to flex the ring finger independently.
- Flexor Digitorum Sublimis (FDS) of the Middle Finger: The second choice if the ring FDS is unsuitable.
- Extensor Indicis Proprius (EIP): An acceptable alternative that does not require a tendon graft, though its vector routing differs.
- Extensor Carpi Ulnaris (ECU), Palmaris Longus (PL), or Extensor Carpi Radialis Longus (ECRL): These muscles require the interposition of a free tendon graft to reach the thumb. A wrist extensor should only be utilized if the remaining wrist extensors are robust.
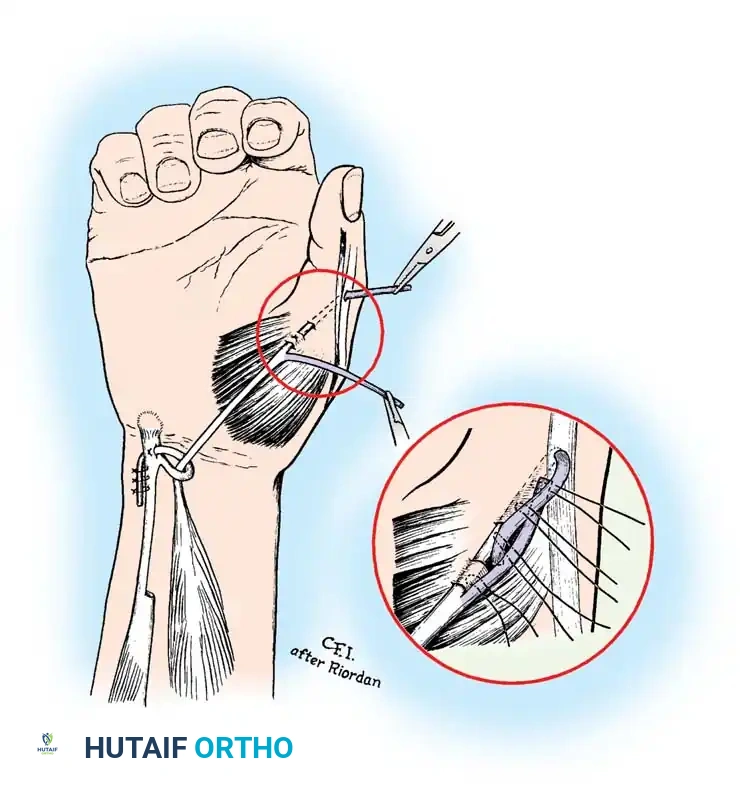
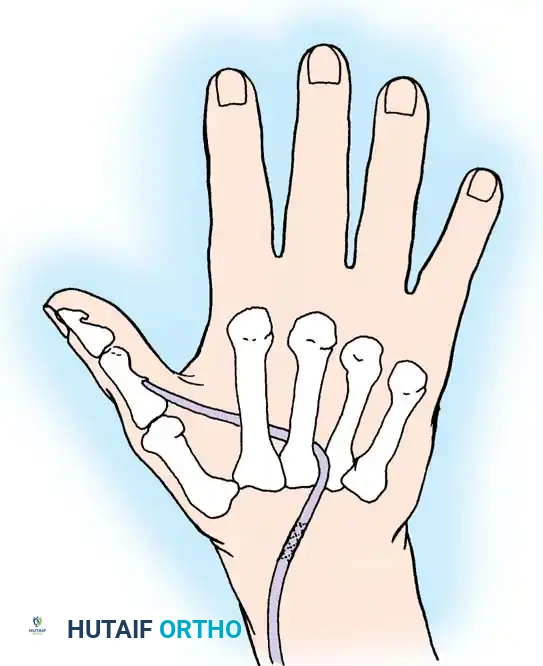
Surgical Technique: The Riordan Transfer
The Riordan technique remains the gold standard for restoring opposition using the FDS of the ring finger, routed through a static pulley constructed from the FCU.
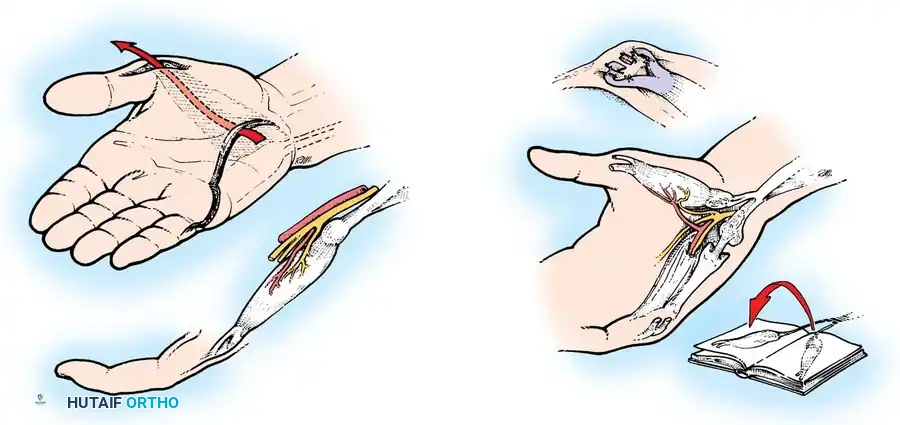
Step 1: Tendon Harvest
Expose the sublimis tendon of the ring finger through an ulnar midlateral incision over the proximal interphalangeal (PIP) joint. Divide the tendon at the level of the joint or just proximal to it.
Carefully divide the chiasm of Camper, separating the two slips of the FDS tendon at the level of the joint so that they pass freely around the profundus tendon. This ensures the tendon can be withdrawn easily at the wrist without tethering.
Step 2: Creation of the FCU Pulley
Expose the flexor carpi ulnaris (FCU) tendon through an L-shaped incision at the wrist. The incision should extend proximally along the FCU tendon and turn radially at its distal end, parallel to the flexor creases of the wrist.
To construct the static pulley, cut halfway through the FCU tendon at a point approximately 6.3 cm proximal to the pisiform. Strip the radial half of the tendon distally, stopping just short of the pisiform. Create a loop large enough for the sublimis tendon to pass through without friction. Carry the end of the radial segment through a split in the remaining intact half of the FCU, loop it back upon itself, and suture it securely.
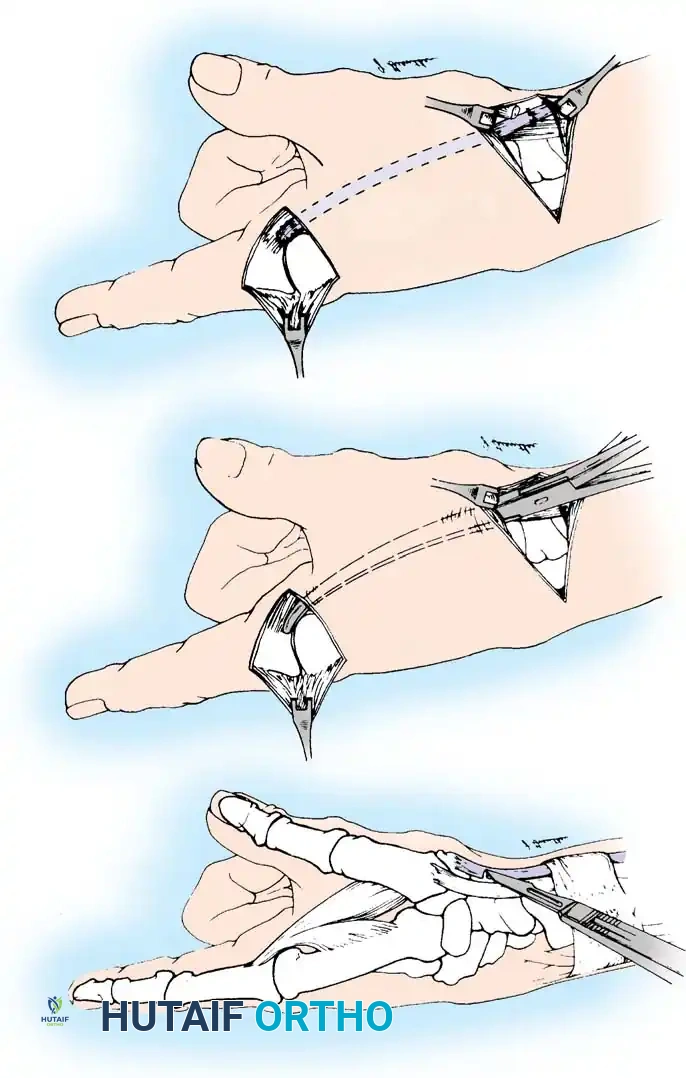
Step 3: Thumb Incision and Preparation
Make a wide, C-shaped incision on the thumb. Begin on the dorsum of the thumb just proximal to the IP joint, proceed proximally and volarward around the radial aspect of the thumb, and curve the incision dorsalward in line with the major skin creases of the thenar eminence just proximal to the MCP joint.
Surgical Warning: On the dorsoradial aspect of the thumb, meticulously identify and preserve the fine sensory branches of the superficial radial nerve to prevent painful postoperative neuromas.
Expose and define the extensor pollicis longus (EPL) tendon over the proximal phalanx, the extensor aponeurosis over the MCP joint, and the insertion footprint of the abductor pollicis brevis (APB).
Step 4: Tendon Routing
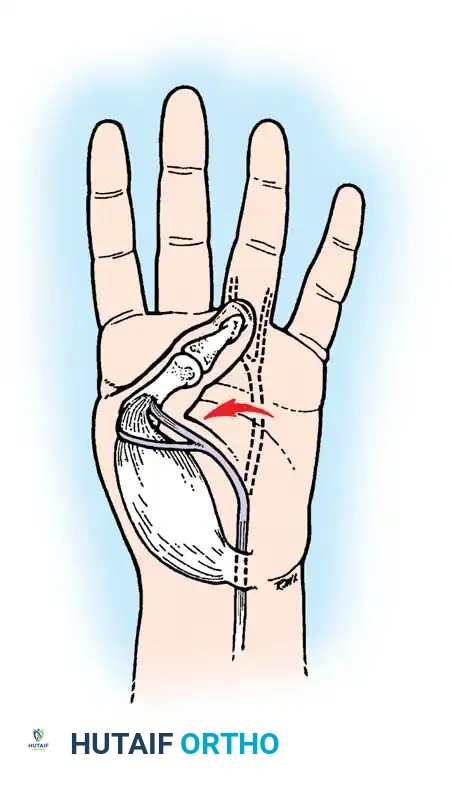
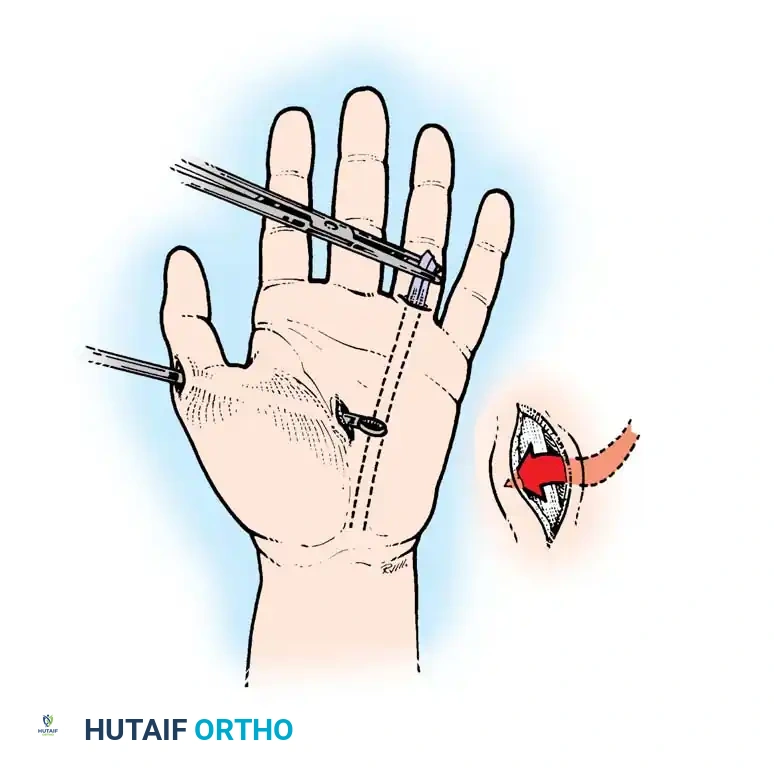
At the wrist, identify the previously released FDS tendon of the ring finger and withdraw it into the proximal forearm incision. Pass the tendon through the newly fashioned FCU loop.
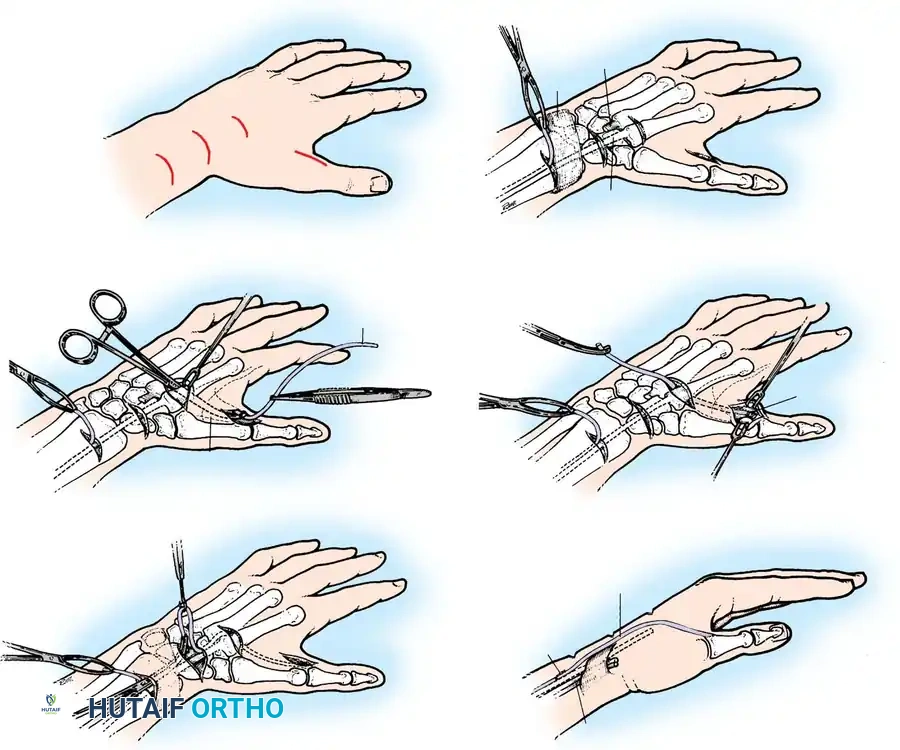
Using a tendon carrier or a small hemostat, pass the FDS tendon subcutaneously across the palm and thenar eminence. The trajectory must perfectly align with the natural muscle fibers of the APB to ensure the correct vector of pull.
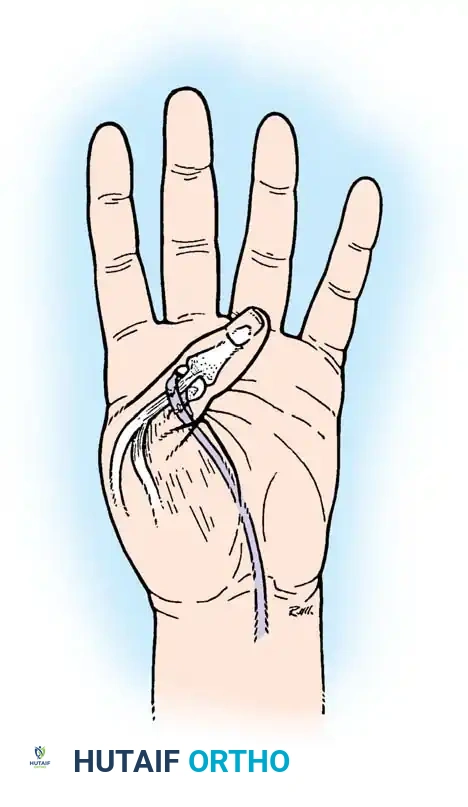
Step 5: Insertion and Anchoring
Make a small tunnel for the insertion of the transfer by burrowing between two small parallel incisions directly within the APB tendon.
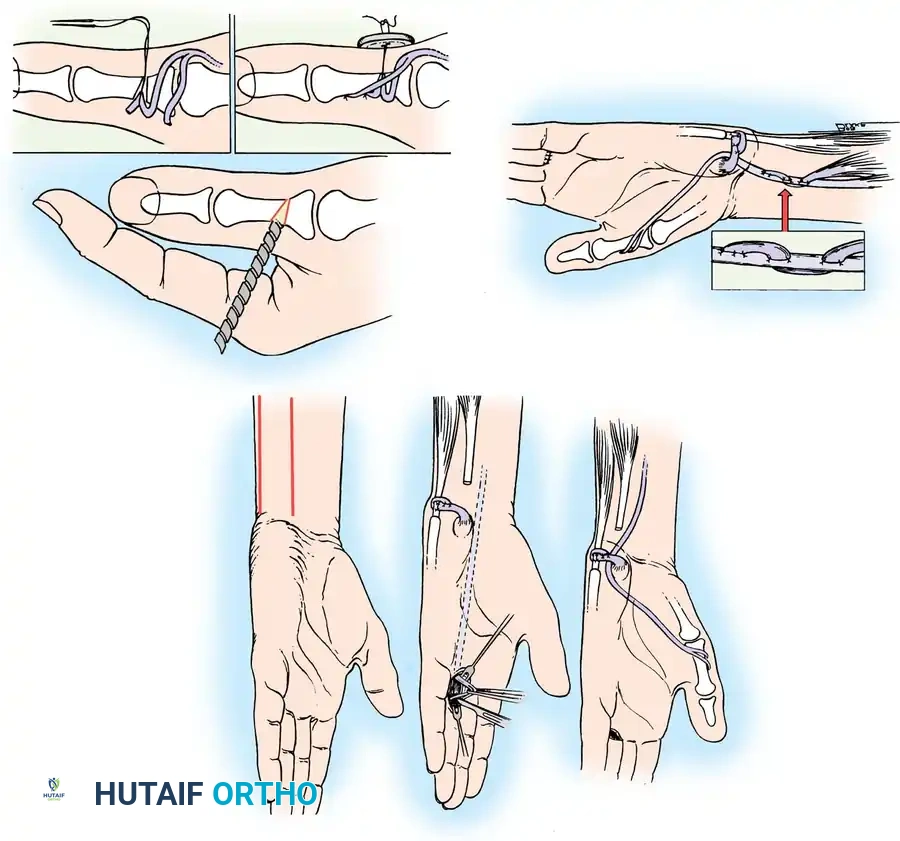
Split the distal end of the FDS tendon for approximately 2.5 cm. Pass one half of the split tendon through the APB tunnel. Next, separate the extensor aponeurosis from the periosteum of the proximal phalanx. Make a small incision in the aponeurosis 6 mm distal to the first tunnel, and pass the same slip of the FDS through it. Finally, bring this slip out from beneath the aponeurosis through a small longitudinal slit in the EPL tendon, approximately 3 mm proximal to the IP joint.
Step 6: Setting the Tension
Determining the proper tension is the most critical step of the operation. Grasp the two slips of the FDS with small hemostats and cross them.
- Testing Tension: With the thumb held in full opposition and the wrist in a neutral (straight) position, place the overlapping slips under moderate tension.
- Relaxation Check: Releasing the thumb and passively flexing the wrist should completely relax the transfer, allowing the thumb to be brought into full extension and abduction.
- Opposition Check: Extending the wrist to 45 degrees should place enough tension on the transfer via the tenodesis effect to automatically bring the thumb into complete opposition, with the tip of the thumb extending fully.
If the tension is insufficient, advance the tendon slips, increase the tension, and repeat the kinematic test.
Once the correct tension is confirmed, suture the slips of the FDS together using non-absorbable braided suture, ensuring the cut ends are buried smoothly to prevent adhesions.
To prevent the transferred tendon from displacing toward the palmar aspect of the joint during active opposition, anchor the transfer and the APB tendon to the underlying MCP joint capsule with a single nylon or wire suture, ensuring the transfer passes over the exact anatomical center of the metacarpal head.
Postoperative Protocol and Rehabilitation
Meticulous postoperative care is essential to protect the transfer while it heals and to facilitate cortical re-education of the donor muscle.
- Immediate Postoperative Phase (0-3 Weeks): Close the wounds with non-absorbable sutures. Immobilize the hand in a bulky pressure dressing reinforced with a dorsal plaster splint. The wrist is positioned in 30 degrees of flexion, the fingers in a functional resting position, and the thumb in full opposition with the distal phalanx extended. Place gauze between the digits to prevent skin maceration.
- Intermediate Phase (3-9 Weeks): At 3 weeks, the rigid splint and sutures are removed. Active range of motion is initiated. However, the thumb must be continuously supported with a custom-molded thermoplastic opponens splint for an additional 6 weeks between exercise sessions.
- Motor Re-education: Because the FDS of the ring finger is a flexor, cortical re-education is highly intuitive. Patients are instructed to actively attempt to touch the tip of their thumb to their ring finger. This maneuver naturally produces flexion of the ring finger, automatically triggering the transferred FDS to fire and oppose the thumb.
- Long-Term Precautions: In patients with lower extremity weakness who habitually rise from a sitting position by pushing up with flattened hands, or in patients who rely on crutches, the transfer is at high risk of attenuation. In these specific populations, the transfer must be protected with an orthosis during weight-bearing activities for a minimum of 3 months, or the tendon will overstretch and permanently cease to function.
