INTRODUCTION TO ADVANCED ELBOW ARTHROSCOPY
The evolution of elbow arthroscopy has transformed the management of complex intra-articular pathology. Historically, conditions such as symptomatic synovial plicae, malunited radial head fractures, and severe post-traumatic arthrofibrosis required extensive open arthrotomies, which carried significant risks of iatrogenic stiffness, neurovascular injury, and prolonged rehabilitation. Today, advanced arthroscopic techniques offer a minimally invasive, highly effective alternative. However, the elbow remains an unforgiving joint. The proximity of major neurovascular structures—namely the radial, median, and ulnar nerves—demands meticulous portal placement, a profound understanding of three-dimensional capsuloligamentous anatomy, and strict adherence to evidence-based surgical principles.
This comprehensive masterclass details the indications, biomechanical considerations, and step-by-step surgical techniques for three critical arthroscopic procedures: the resection of a thickened pathological synovial plica, arthroscopic radial head resection, and the comprehensive release of the arthrofibrotic elbow.
RESECTION OF THICKENED PATHOLOGICAL SYNOVIAL PLICA
Pathoanatomy and Biomechanics
The synovial plica of the elbow is a normal embryological remnant, most commonly located in the posterolateral radiocapitellar joint. In the normal elbow, this thin synovial fold glides asymptomatically during flexion, extension, pronation, and supination. However, repetitive microtrauma—often seen in throwing athletes, racquet sports players, or manual laborers—can induce localized synovitis. Over time, this inflammatory cascade leads to fibrotic hypertrophy of the plica.
A thickened, pathological plica alters the delicate kinematics of the radiocapitellar articulation. It can become mechanically incarcerated between the radial head and the capitellum during dynamic movement, producing a characteristic "catching" or "popping" sensation. This mechanical impingement not only causes localized lateral elbow pain but can also lead to secondary chondromalacia of the radial head or capitellum if left untreated.
Clinical Evaluation and Indications
Patients typically present with lateral-sided elbow pain that mimics lateral epicondylitis. However, unlike epicondylitis, the pain is often exacerbated by terminal extension and combined pronation-supination. A palpable snap or click may be appreciated over the posterolateral joint line. Magnetic Resonance Imaging (MRI) is the gold standard for preoperative diagnosis, often revealing a thickened, nodular band of tissue in the posterolateral gutter with associated focal synovitis.
Surgical resection is indicated when patients fail a comprehensive conservative regimen consisting of rest, non-steroidal anti-inflammatory drugs (NSAIDs), targeted physical therapy, and intra-articular corticosteroid injections.
Surgical Technique: Step-by-Step Resection
Surgical Warning: The radial nerve lies in close proximity to the anterolateral portal. To minimize risk, the joint must be maximally distended with fluid prior to portal establishment, and the incision should be made using a "nick and spread" technique with a hemostat down to the capsule.
- Patient Positioning and Setup: The patient may be positioned in the lateral decubitus, prone, or supine suspended position, depending on surgeon preference. A proximal arm tourniquet is applied. The elbow is flexed to 90 degrees to relax the anterior neurovascular structures.
- Diagnostic Arthroscopy:
- Establish the anteromedial portal first. This serves as the primary viewing portal for the anterior compartment.
- Visualize the elbow anteriorly and posteriorly using multiple portals. The anterolateral aspect of the elbow, including the anterior radiocapitellar joint, is comprehensively visualized through this anteromedial portal.
- Dynamic Assessment: Under direct visualization, range the elbow through flexion, extension, pronation, and supination. If a pathological catching or popping of the plica is noted as it snaps across the radiocapitellar joint, surgical resection is confirmed.
- Anterior Debridement: Establish the anterolateral portal under direct inside-out visualization. Introduce a 4.0-mm arthroscopic shaver. Debride the anterior joint space and shave the anterior extension of the thickened plica.
- Posterior Compartment Evaluation:
- Transition the arthroscope to the posterolateral portal. Utilizing a 70-degree, 2.7-mm or 4.0-mm arthroscope is highly recommended to navigate the tight confines of the posterior radiocapitellar joint.
- Identify the main body of the hypertrophic plica in the posterolateral gutter.
- Plica Resection: Establish a direct lateral portal (soft spot portal). Introduce an aggressive shaver or a small arthroscopic basket punch. Resect the thickened pathological tissue back to a stable, healthy synovial rim. Ensure that the resection is thorough enough to prevent recurrence but conservative enough to avoid iatrogenic injury to the lateral ulnar collateral ligament (LUCL).
Postoperative Care Protocol
Postoperatively, the patient is placed in a sling for 3 to 5 days to allow for initial settling of the elbow and to minimize hemarthrosis. Early active range of motion (ROM) is initiated immediately after sling removal to prevent capsular adhesions. A progressive strengthening program targeting the forearm and periscapular stabilizers begins at 3 weeks. Return to competitive sports or heavy manual labor is generally allowed in 2 to 3 months, contingent upon the restoration of painless, full ROM and symmetrical strength.
ARTHROSCOPIC RADIAL HEAD RESECTION (TECHNIQUE 52-33)
Indications and Biomechanical Considerations
The radial head is a crucial secondary stabilizer of the elbow, providing resistance against valgus stress and longitudinal radioulnar translation. However, in cases of severe malunited radial head fractures (e.g., late-stage Mason Type III or IV) or painful, advanced radiocapitellar osteoarthritis, the radial head becomes a source of debilitating mechanical block and pain.
Arthroscopic radial head resection is indicated when the primary stabilizers (the medial ulnar collateral ligament and the interosseous membrane) are intact. If these structures are compromised, radial head resection is strictly contraindicated due to the risk of catastrophic proximal radial migration (Essex-Lopresti syndrome) or gross valgus instability.
Surgical Technique: Arthroscopic Excision
Clinical Pearl: When performing an arthroscopic radial head resection, the annular ligament must be meticulously preserved. Iatrogenic transection of the annular ligament can lead to symptomatic posterolateral rotatory instability (PLRI).
- Portal Placement and Visualization:
- The arthroscope is placed in the anteromedial portal to provide a panoramic view of the radiocapitellar joint.
- An arthroscopic burr (typically 4.0-mm or 5.5-mm, hooded to protect adjacent soft tissues) is introduced through the anterolateral portal.
- Synovectomy and Exposure: A partial synovectomy is often necessary to adequately examine the radial head, the capitellum, and the annular ligament. Clear the anterior capsule away from the radial neck to define the safe resection margins.
- Piecemeal Resection:
- Begin the resection at the articular surface of the radial head.
- The radial head and a portion of the neck are resected using the arthroscopic burr in a piecemeal fashion.
- The resection must be carried proximally past the level of the sigmoid notch of the ulna to ensure no bony impingement remains during forearm rotation.
- Dynamic Impingement Check: After the visual resection is completed, the burr is removed. The forearm is actively pronated and supinated while the elbow is moved through a full arc of flexion and extension. The surgeon must directly observe the resection site to ensure that no residual bony prominences impinge against the ulna or the annular ligament.
ARTHROSCOPIC MANAGEMENT OF ELBOW ARTHROFIBROSIS
Pathophysiology of the Stiff Elbow
Arthrofibrosis is a relatively common and highly debilitating complication following elbow fractures, dislocations, or severe inflammatory events. The elbow capsule is uniquely prone to fibroblastic proliferation and contracture. Post-traumatic bleeding and inflammation lead to the deposition of dense, disorganized collagen within the anterior and posterior capsules, obliterating the normal capsular recesses. Furthermore, osteophyte formation in the coronoid and olecranon fossae frequently exacerbates the mechanical block to motion.
For patients with mild symptoms (flexion contractures < 30 degrees), aggressive conservative treatment—including static progressive orthoses, dynamic splinting, and intensive physical therapy—may be sufficient. However, in patients with severe, recalcitrant involvement that has plateaued after 6 months of conservative care, surgical intervention is generally indicated.
The Challenge of the Arthrofibrotic Joint
Good to excellent results can be obtained using arthroscopic treatment for elbow stiffness; however, it is one of the most technically demanding procedures in orthopedic surgery. In arthrofibrotic elbows, the ability to distend the joint capsule and identify normal anatomical landmarks is severely compromised.
Surgical Warning: Gallay et al. demonstrated that the capacity of a normal elbow joint is 15 to 25 mL of saline, whereas the capacity of an arthrofibrotic elbow is reduced to a mere 6 mL. This drastic reduction in volume means the neurovascular structures are not pushed away from the capsule during distension, drastically increasing the risk of iatrogenic nerve injury during portal placement.
When performing procedures on arthrofibrotic elbows, a thorough, masterful familiarity with elbow arthroscopy and regional anatomy is mandatory. The surgeon must always be prepared to convert to an open procedure (e.g., a lateral column procedure) if adequate visualization cannot be obtained safely.
Surgical Technique: Arthroscopic Capsular Release (Technique 52-34)
- Initial Access and Anterior Release:
- Due to the contracted capsule, portals must be established with extreme caution. A spinal needle is used to locate the joint space, often requiring fluoroscopic assistance.
- Once the anteromedial and anterolateral portals are established, the initial view is often obscured by dense fibrotic tissue.
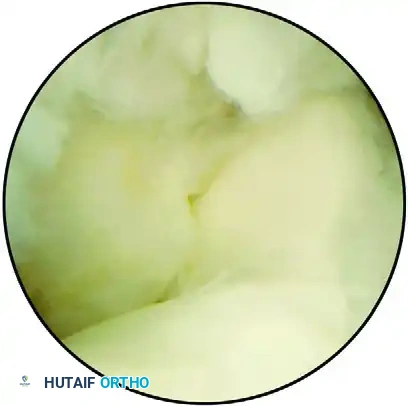
FIGURE 52-70 A: Arthroscopic view of an arthrofibrotic joint. The coronoid is visible on the left and the trochlea on the right, obscured by extensive, dense fibrosis superiorly.
- Capsulectomy:
- Using an arthroscopic shaver and radiofrequency ablation wand, the fibrotic tissue is systematically resected.
- An anterior capsulectomy is performed, releasing the distal capsular insertion off the anterior humerus. This allows the brachialis muscle fibers to be visualized, confirming a complete anterior release.

FIGURE 52-70 B: View after the resection of fibrotic tissue and the release of the distal capsular insertion onto the humerus. The underlying bony architecture is revealed, showing the coronoid fossa completely filled by a large, impinging osteophyte.
- Osteophyte Resection and Fossa Recreation:
- Once the soft tissue contracture is released, bony blocks to motion must be addressed.
- An arthroscopic burr is introduced to resect the osteophytes filling the coronoid fossa (anteriorly) and the olecranon fossa (posteriorly).
- The fossae must be deepened and re-created to accommodate the coronoid process during terminal flexion and the olecranon tip during terminal extension.

FIGURE 52-70 C: The coronoid fossa after complete resection of the osteophyte and re-creation of the anatomical fossa. This critical step restores the mechanical clearance necessary to allow full elbow flexion.
- Posterior Compartment Release:
- The arthroscope is moved to the posterior portals (posterocentral and posterolateral).
- A posterior capsulectomy is performed, and any fibrous bands tethering the triceps or obliterating the olecranon recess are excised.
- Care must be taken medially to avoid the ulnar nerve, which may be encased in scar tissue. If ulnar nerve symptoms were present preoperatively, an open ulnar nerve decompression and transposition should be performed prior to the arthroscopic posterior release.
Postoperative Rehabilitation for Arthrofibrosis
The success of an arthroscopic arthrolysis is entirely dependent on the postoperative rehabilitation protocol.
1. Immediate Phase (Days 0-3): An indwelling interscalene or supraclavicular nerve block is highly recommended to provide profound analgesia, allowing for immediate, painless continuous passive motion (CPM). The elbow is never immobilized.
2. Intermediate Phase (Weeks 1-6): Aggressive active and active-assisted ROM exercises are performed multiple times daily. Static progressive extension and flexion splints are utilized during sleep and rest periods to maintain the intraoperative gains.
3. Late Phase (Weeks 6-12): Strengthening is gradually introduced only after the newly acquired ROM is stable and painless. NSAIDs (e.g., Indomethacin) or localized radiation therapy may be prescribed in high-risk patients to prevent heterotopic ossification (HO).
By adhering to these strict biomechanical principles and meticulous surgical techniques, the orthopedic surgeon can safely navigate the complexities of the elbow joint, restoring function and alleviating pain in patients with plica syndrome, radial head pathology, and severe arthrofibrosis.
