Operative Management of Lesser Ray Pathologies: Fifth Metatarsal Head Resection and Freiberg Infraction
Key Takeaway
Resection of the fifth metatarsal head is a salvage procedure primarily indicated for bunionette deformities in the insensitive foot complicated by ulceration. Conversely, Freiberg infraction, an osteochondrosis of the lesser metatarsal heads, requires a nuanced approach. Joint débridement with metatarsal head remodeling remains the gold standard, while dorsal closing wedge osteotomies are reserved for localized dorsal lesions to restore joint congruity and preserve metatarsophalangeal kinematics.
INTRODUCTION TO LESSER RAY PATHOLOGIES
The operative management of lesser ray pathologies demands a profound understanding of forefoot biomechanics, load distribution, and the delicate soft-tissue envelope of the foot. While joint-preserving osteotomies remain the gold standard for most forefoot deformities, specific clinical scenarios—such as the neuropathic foot with a severe bunionette or advanced osteochondrosis of the lesser metatarsal heads—necessitate specialized, and sometimes ablative, surgical interventions.
This comprehensive guide details the indications, biomechanical rationale, and step-by-step surgical execution for two distinct lesser ray procedures: the resection of the fifth metatarsal head for recalcitrant bunionette deformity, and the joint-preserving and reconstructive options for Freiberg infraction.
RESECTION OF THE FIFTH METATARSAL HEAD FOR BUNIONETTE DEFORMITY
A bunionette, or tailor's bunion, is a painful prominence on the lateral aspect of the fifth metatarsal head. While mild to moderate deformities in sensate patients are typically managed with distal or diaphyseal metatarsal osteotomies, resection of the fifth metatarsal head is a non-anatomic salvage procedure.
Indications and Patient Selection
We do not recommend this procedure for the initial operative treatment of a bunionette deformity in a healthy, sensate foot. Primary resection alters the lateral column biomechanics and can lead to devastating transfer metatarsalgia or lateral column instability.
This procedure is strictly reserved for:
* The Insensitive Foot: Patients with profound peripheral neuropathy (e.g., advanced diabetic neuropathy, Charcot neuroarthropathy).
* Chronic Ulceration: The presence of recurrent, recalcitrant callus formation or active ulceration directly beneath or lateral to the fifth metatarsal head.
* Osteomyelitis: Localized bone infection of the fifth metatarsal head where joint preservation is impossible.
* Salvage: Failed previous osteotomies with severe degenerative joint disease in low-demand, elderly patients.
💡 Clinical Pearl: The Neuropathic Foot
In the diabetic neuropathic foot, the primary goal of surgery is ulcer healing and the prevention of amputation, not radiographic restoration of anatomy. Resecting the prominent fifth metatarsal head effectively decompresses the lateral column, allowing chronic ulcers to heal by removing the underlying bony prominence.
Preoperative Planning
Thorough vascular assessment is mandatory. Non-invasive vascular studies (ABI, TBI, Doppler waveforms) must confirm adequate perfusion for wound healing, particularly in the diabetic cohort. Weight-bearing anteroposterior, lateral, and oblique radiographs are utilized to assess the degree of lateral bowing, the 4-5 intermetatarsal angle, and the presence of osteomyelitis or joint destruction.
Surgical Technique: Fifth Metatarsal Head Resection
1. Patient Positioning and Anesthesia
* The patient is placed in the supine position.
* A regional ankle block or popliteal sciatic nerve block is preferred, supplemented with monitored anesthesia care (MAC).
* A calf or thigh tourniquet is applied, provided there is no severe peripheral arterial disease.
2. Surgical Approach
* Make a 4 to 5 cm midlateral incision over the distal third of the fifth metatarsal.
* Surgical Warning: Avoid a direct plantar or plantar-lateral incision to prevent a painful postoperative scar on the weight-bearing surface.
* Carefully dissect through the subcutaneous tissues. Identify and protect the dorsal cutaneous branch of the sural nerve, which courses dorsolaterally in this region.
3. Capsular Exposure and Resection
* Incise the periosteum and the lateral capsule of the fifth metatarsophalangeal (MTP) joint longitudinally.
* Reflect the capsule dorsally and plantarly to achieve full exposure of the metatarsal head and the head-neck junction.
* Using an oscillating microsaw, resect the metatarsal head obliquely. The cut should begin 5 mm proximal to the capsular insertion at the head-neck junction.
* The trajectory of the cut must be oblique—directed from distal-lateral to proximal-medial, and slightly plantar-distal to dorsal-proximal. This beveling prevents a sharp bony stump that could cause recurrent ulceration or a new pressure point.
4. Closure
* Copiously irrigate the wound to remove all bone debris.
* Rasp the remaining metatarsal stump to ensure absolute smoothness.
* Close the MTP capsule over the resected bone end using 2-0 or 3-0 absorbable sutures (e.g., Vicryl) to interpose soft tissue and stabilize the base of the proximal phalanx.
* Close the skin with nonabsorbable sutures (e.g., 3-0 or 4-0 Nylon) using a tension-free technique.
Postoperative Protocol
- Immediate Post-op: Weight-bearing to tolerance in a rigid, wooden-soled postoperative shoe is allowed immediately.
- First 48-72 Hours: Strict elevation of the extremity is strongly encouraged to minimize edema and protect the incision.
- Suture Removal: At 14 to 21 days, depending on the vascular status and wound healing.
- Long-term: The patient is usually transitioned to a wide, lace-up shoe with a custom accommodative orthotic or a metatarsal pad at 4 weeks.
FREIBERG INFRACTION
First described by A.H. Freiberg in 1914, Freiberg infraction is a painful osteochondrosis (avascular necrosis) of the lesser metatarsal heads. Freiberg initially reported six cases involving the second metatarsal head, noting that three had a history of a single significant traumatic event. He hypothesized the disorder was secondary to acute trauma. In 1917, Campbell reported the identical condition in the third metatarsal head. Despite numerous large series published since, the exact etiology remains debated, likely representing a combination of vascular compromise and repetitive microtrauma.
Pathoanatomy and Biomechanics
The second metatarsal is typically the longest and most rigidly fixed at its base (within the mortise of the cuneiforms). During the terminal stance phase of gait, it bears the highest concentration of stress. The arterial supply to the metatarsal head is tenuous, relying on capsular vessels. Repetitive microtrauma can disrupt this blood supply, leading to subchondral collapse, cartilage fragmentation, and eventual joint incongruity.
It is most commonly recognized in the second decade of life (adolescence) and radiographically resembles other examples of osteochondrosis.
Clinical Presentation and Imaging
Patients typically present with insidious onset of forefoot pain, localized swelling, and restricted range of motion at the affected MTP joint. Pain is exacerbated by weight-bearing, high-heeled shoes, or activities requiring forced dorsiflexion (e.g., running, dancing).
Radiographic evaluation is critical for staging the disease (Smillie's Classification). Early stages may show subtle joint space widening or subchondral sclerosis. Late stages demonstrate flattening of the metatarsal head, central depression, loose body formation, and joint space narrowing.

🔍 Diagnostic Pearl: The Role of MRI
We heavily utilize Magnetic Resonance Imaging (MRI) to evaluate the metatarsal head in early or ambiguous cases. MRI is highly sensitive for detecting early bone marrow edema, occult subchondral fractures, and assessing the exact extent of articular cartilage viability before radiographic collapse occurs.
Surgical Decision Making
When conservative measures (metatarsal pads, stiff-soled shoes, offloading boots, NSAIDs) fail, surgical intervention is warranted. Historically, a multitude of procedures have been proposed:
- Elevation and Bone Grafting: Elevation of the depressed fragment of the metatarsal head and bone grafting of the defect (Smillie).
- Phalangeal Resection: Resection of the base of the proximal phalanx with syndactylization of the second and third toes (Trott).
- Dorsal Closing Wedge Osteotomy: Redirecting the plantar cartilage dorsally (Gauthier and Elbay).
- Joint Débridement and Remodeling: Cheilectomy and removal of loose bodies (Freiberg and Mann).
- Osteochondral Autograft Transfer (OATS): Transplantation of an osteochondral plug from the ipsilateral knee to the second metatarsal head (used in late-stage disease).
Preferred Surgical Techniques
1. Joint Débridement and Metatarsal Head Remodeling
We have been highly pleased with joint débridement and metatarsal head remodeling, utilizing it most often for mild to moderate disease (Smillie Stages II-III).
- Approach: A dorsal longitudinal incision is made over the affected MTP joint. The extensor tendons are retracted laterally.
- Arthrotomy: A dorsal capsulotomy exposes the joint.
- Débridement: All loose osteochondral fragments are excised. The hypertrophic synovium is aggressively resected.
- Remodeling: Using a high-speed burr or rongeur, the peripheral osteophytes and the flattened dorsal lip of the metatarsal head are resected (cheilectomy). The goal is to decompress the joint and restore a smooth, albeit non-spherical, gliding surface.
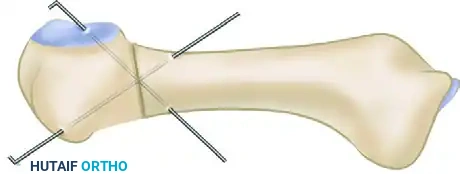
2. Dorsal Closing Wedge Osteotomy (Gauthier and Elbay Technique)
If MRI and intraoperative evaluation reveal that the necrotic lesion is strictly localized to the dorsum of the metatarsal head, with the plantar articular cartilage remaining pristine and uninvolved, a dorsiflexion closing wedge osteotomy of the metatarsal neck is highly successful.
- Rationale: This extra-articular osteotomy rotates the healthy plantar cartilage dorsally, restoring a congruent articular surface to articulate with the proximal phalanx during the critical toe-off phase of gait.
- Technique: Following dorsal exposure, a wedge of bone (base dorsal) is resected from the metatarsal neck, just proximal to the articular surface.

- Fixation: The osteotomy is closed by dorsiflexing the metatarsal head. It is then rigidly fixed. While various fixation methods exist (screws, plates), cross-pinning with Kirschner wires remains a reliable and cost-effective method.
3. Procedures to Avoid in the Young Patient
Rarely, we have added resection of the base of the proximal phalanx. However, this shortens the toe significantly. Because 90% of patients presenting with Freiberg infraction are in late adolescence or early adulthood, we strongly try to avoid this resection. Joint débridement and remodeling of the metatarsal head should suffice in the vast majority of cases.
While a number of other treatments (such as interpositional arthroplasty or total joint replacement) have been proposed, they lack sufficient numbers or long-term follow-up to give clear guidance that they are superior to current recommendations.
Postoperative Care and Patient Counseling
- Immobilization: Following débridement, patients are placed in a stiff-soled surgical shoe. If an osteotomy is performed, heel-weight-bearing in a CAM boot is required for 4 to 6 weeks until radiographic union is achieved.
- Orthotics: Metatarsal bars or custom orthotic pads should be utilized for 3 to 6 months after surgery to continuously offload the healing metatarsal head.
- Patient Counseling (CRITICAL): The patient must be explicitly informed before surgery that some permanent limitation of MTP joint motion is usual and expected. Because motion in the affected joint is frequently limited preoperatively due to pain and mechanical block, this postoperative stiffness is usually not a deterrent to surgery and is well-tolerated provided the pain is resolved.
You Might Also Like
