INTRODUCTION AND HISTORICAL CONTEXT
The resection of the distal ulna, universally recognized as the Darrach procedure, remains a foundational technique in operative orthopaedics for the management of severe, painful conditions involving the distal radioulnar joint (DRUJ). First performed by William Darrach at the suggestion of Thomas Dwight in 1910, the operation was originally designed to address chronic, irreducible dislocations of the distal ulna associated with malunited fractures of the distal radius.
Over the past century, the indications for distal ulnar resection have evolved. While historically utilized as a primary intervention for a broad spectrum of DRUJ disorders, contemporary orthopedic practice reserves the Darrach procedure primarily for elderly, low-demand patients, or as a salvage operation when joint-preserving techniques have failed.
Darrach’s original observations remain clinically relevant today: following subperiosteal resection, new bone frequently forms within the sutured periosteal envelope. This osteogenesis varies from a mild excrescence on the distal ulnar stump to almost complete osseous union with the preserved styloid process; however, the functional articular head of the ulna never regenerates. When executed correctly in the appropriately selected patient, rotary motions of the forearm are reliably restored, and debilitating pain is typically relieved within a few weeks postoperatively.
BIOMECHANICS OF THE DISTAL RADIOULNAR JOINT
To understand the consequences of distal ulnar resection, the orthopedic surgeon must possess a profound grasp of DRUJ biomechanics. The DRUJ is a diarthrodial trochoid joint that, in conjunction with the proximal radioulnar joint (PRUJ) and the interosseous membrane (IOM), facilitates pronosupination of the forearm.
Under normal physiological conditions, the distal ulna acts as the fixed fulcrum around which the radius rotates. Furthermore, the ulna provides critical structural support to the ulnar carpus. Axial loading across the human wrist is distributed approximately 80% through the radiocarpal articulation and 20% through the ulnocarpal articulation via the triangular fibrocartilage complex (TFCC).
Biomechanical Warning: Resection of the distal ulna fundamentally alters the axial loading characteristics of the wrist. By removing the ulnar head, the ulnocarpal support is obliterated, forcing the radius to absorb nearly 100% of the axial load. This can lead to ulnar translation of the carpus, radiocarpal overload, and subsequent degenerative changes.
Furthermore, the distal ulna serves as the primary attachment site for the TFCC, the distal interosseous membrane (DIOM), and the pronator quadratus. Excision of the ulnar head disrupts these stabilizing structures, predisposing the remaining ulnar stump to dynamic instability, particularly during forceful grip and pronation.
INDICATIONS FOR DISTAL ULNA RESECTION
The Darrach procedure is highly effective but must be applied judiciously. It is most commonly recommended for symptomatic DRUJ pathology in patients who are elderly, debilitated, or possess low functional demands.
Primary Indications
- Rheumatoid Arthritis: Severe destruction of the DRUJ with dorsal subluxation of the ulnar head (caput ulnae syndrome), threatening extensor tendon rupture (Vaughan-Jackson syndrome).
- Post-Traumatic Osteoarthritis: End-stage arthrosis of the DRUJ following intra-articular fractures where joint-preserving procedures are not viable.
- Complex Malunions and Nonunions: In cases of radial shaft nonunion or malunion with significant overlapping of fragments (without concomitant ulnar fracture), radial shortening produces severe derangement of the DRUJ articular surfaces. If the shortening is marked, secondary dislocation occurs. In chronic cases where soft tissue contracture prevents the restoration of radial length, resecting the distal ulna and bone-grafting the shortened radius with the fragments in apposition is often the most pragmatic and successful alternative.
- Salvage: Failed partial resection arthroplasties (e.g., Bowers procedure) or failed DRUJ arthrodesis (e.g., Sauvé-Kapandji procedure).
Contraindications
- High-Demand Patients: Young, active individuals or manual laborers will poorly tolerate the loss of grip strength and potential stump instability.
- Essex-Lopresti Injuries: Global longitudinal instability of the forearm axis (radial head fracture, IOM tear, DRUJ disruption) is an absolute contraindication. Resecting the distal ulna in this setting will result in catastrophic proximal migration of the radius and severe ulnocarpal impingement.
- Incompetent TFCC in High-Demand Wrists: Hemiresection procedures should be avoided if the TFCC cannot be reconstructed or preserved.
DISADVANTAGES AND COMPLICATIONS
While successful in relieving pain, the Darrach procedure is fraught with potential biomechanical disadvantages. Peterson, Adams, and other prominent authors have extensively documented the complications associated with this technique.
- Ulnar Stump Instability: The most common and debilitating complication. If the ulna is resected excessively (proximal to the insertion of the pronator quadratus), the distal stump loses its dynamic volar restraint. During pronation, the stump subluxates dorsally, causing a painful "clunk," visible deformity, and severe disability.
- Decreased Grip Strength: Loss of the ulnar fulcrum significantly diminishes the mechanical advantage of the extrinsic flexors.
- Radioulnar Impingement: The unstable ulnar stump may dynamically converge and impinge against the distal radius during forceful grip, causing severe pain (radioulnar convergence).
- Carpal Kinematic Alteration: Coulet et al. demonstrated that ulnar resection after distal radial osteotomy is limited in its ability to correct deformity or increase mobility. Post-resection, patients frequently exhibit ulnar tilt of the wrist, cartilage damage, and ulnar deviation of the carpus exceeding 5 mm due to the loss of the ulnar buttress.
Surgical Pearl: The golden rule of the Darrach procedure is meticulous preservation of the ulnar styloid and its attached ulnar collateral ligament (UCL), combined with minimal bone resection. Except for compelling oncologic or infectious reasons, no more than 2.5 cm of bone should ever be resected.
SURGICAL TECHNIQUE: THE DARRACH PROCEDURE (STEP-BY-STEP)
Meticulous surgical technique is paramount to minimizing postoperative complications, specifically ulnar stump instability. The procedure is typically performed under regional anesthesia (supraclavicular or axillary block) with a proximal pneumatic tourniquet.
Step 1: Approach and Exposure
Position the patient supine with the arm extended on a radiolucent hand table. The forearm is placed in neutral rotation.
Expose the distal ulna through a 5 to 6 cm medial (ulnar) longitudinal incision, centered over the palpable ulnar head and extending proximally.
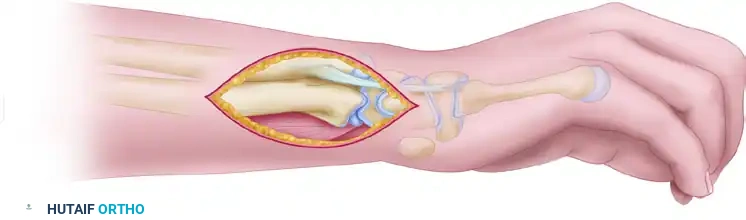
Carefully dissect through the subcutaneous tissues, identifying and protecting the dorsal sensory branch of the ulnar nerve, which typically crosses from volar to dorsal approximately 5 cm proximal to the ulnar styloid.
Step 2: Periosteal Incision and Reflection
Identify the extensor carpi ulnaris (ECU) tendon and its subsheath. Incise the periosteum of the distal ulna longitudinally along its ulnar border.
Using a sharp Freer or periosteal elevator, reflect the periosteum from the distal ulna.
Pitfall: Exercise extreme caution to avoid perforating the periosteal sleeve. A robust, intact periosteal envelope is critical for postoperative stabilization of the ulnar stump.
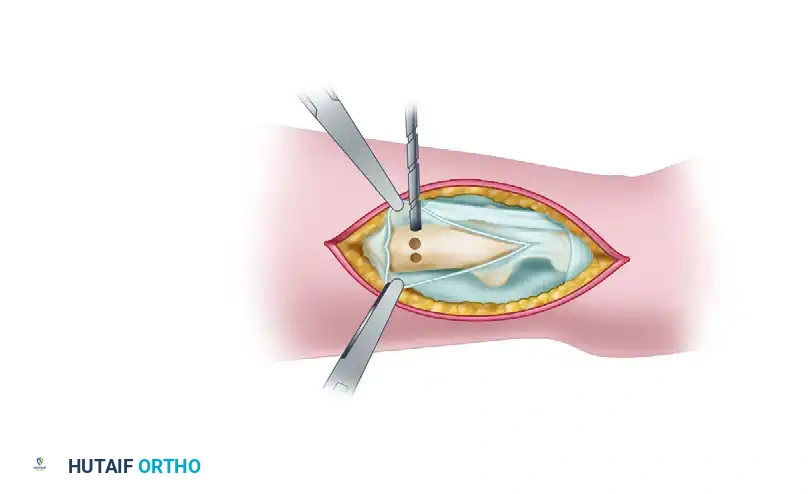
Step 3: Osteotomy Preparation
Measure approximately 2.5 cm proximal to the distal articular end of the ulna. This level is critical; resecting proximal to the pronator quadratus insertion guarantees stump instability.
To prevent stress risers and control the osteotomy, drill multiple holes transversely through the ulnar diaphysis at the planned resection level.
Step 4: Resection of the Ulnar Head
Complete the division of the bone using a sharp bone-biting forceps or an oscillating saw, connecting the pre-drilled holes.
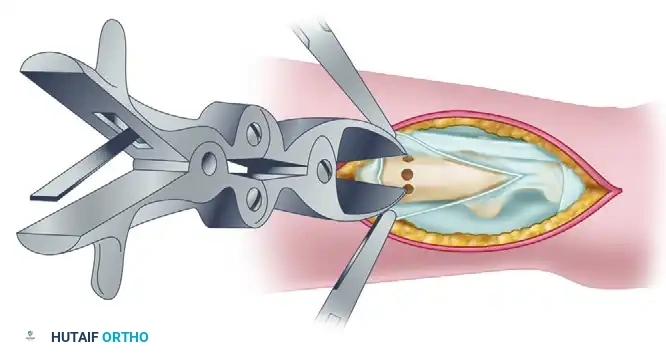
Once the osteotomy is complete, grasp the distal fragment with a towel clip or bone tenaculum. Gently lift the distal fragment outside the wound to expose the deep capsular attachments.
Step 5: Capsular Division and Styloid Preservation
Divide the capsule of the DRUJ close to the articular cartilage of the ulnar head.
Crucially, divide the ulnar styloid at its base using a fine osteotome or bone rongeur. Leave the ulnar styloid attached to the ulnar collateral ligament and the TFCC. This preserves the ulnocarpal ligamentous complex and prevents ulnar translation of the carpus. Remove the resected ulnar head.
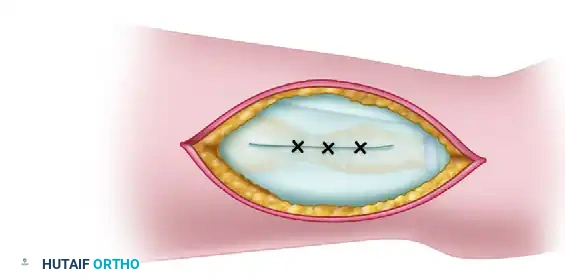
Step 6: Soft Tissue Stabilization and Closure
The most critical step in preventing postoperative instability is the management of the empty periosteal sleeve.
Reef and plicate the periosteal envelope tightly.
Use heavy, non-absorbable sutures (e.g., 0 or 2-0 Ethibond) to imbricate the periosteum and the dorsal capsule over the distal end of the remaining ulnar stump. This creates a soft-tissue tether that stabilizes the bone during pronosupination.

Deflate the tourniquet, achieve meticulous hemostasis, and close the skin with interrupted sutures.
POSTOPERATIVE CARE AND REHABILITATION
Unlike many joint reconstructive procedures, the classic Darrach procedure requires minimal immobilization, provided the periosteal sleeve was securely plicated.
- Days 1-14: No rigid immobilization is strictly necessary, though a bulky soft dressing or a removable volar splint may be used for comfort. Active range of motion (ROM) exercises for the fingers, wrist, and forearm (pronosupination) are encouraged starting the day after surgery to prevent capsular adhesions.
- Weeks 2-6: Suture removal at 10-14 days. Progressive strengthening is initiated. Patients are cautioned against heavy lifting or forceful gripping in pronation, which stresses the stabilizing soft tissues.
- Long-Term: Maximum medical improvement is typically reached by 3 to 6 months. Patients should be counseled that while pain is significantly reduced, grip strength will permanently remain at approximately 70-80% of the contralateral side.
MANAGEMENT OF COMPLICATIONS: THE BUNNELL TECHNIQUE
If the ulna has been inadvertently resected at a level proximal to the pronator quadratus, or if the periosteal sleeve fails, the distal ulnar stump will subluxate dorsally during pronation, causing severe pain and mechanical disability.
If conservative management (bracing, activity modification) fails and the disability warrants surgical intervention, the Bunnell Technique is a highly effective salvage procedure. This technique utilizes a tendon graft to create a dynamic volar restraint.
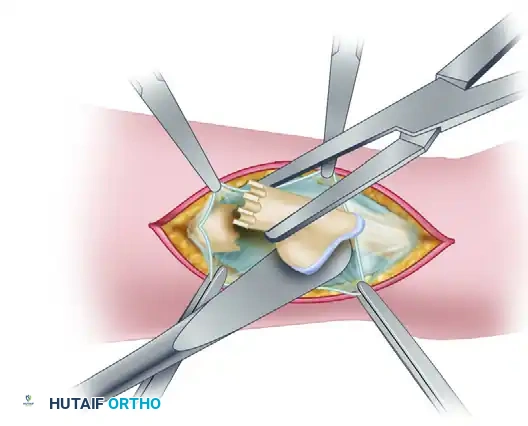
Bunnell Stabilization Technique
- A free tendon graft (often palmaris longus or a strip of flexor carpi ulnaris) is harvested.
- The graft is looped circumferentially around the unstable ulnar stump and intertwined with the intact tendon of the flexor carpi ulnaris (FCU).
- The tendon graft is joined to itself using a removable running suture of stainless steel wire.
- The dynamic tension of the FCU effectively holds the ulnar stump anteriorly (volarly), counteracting the dorsal subluxation forces during pronation.
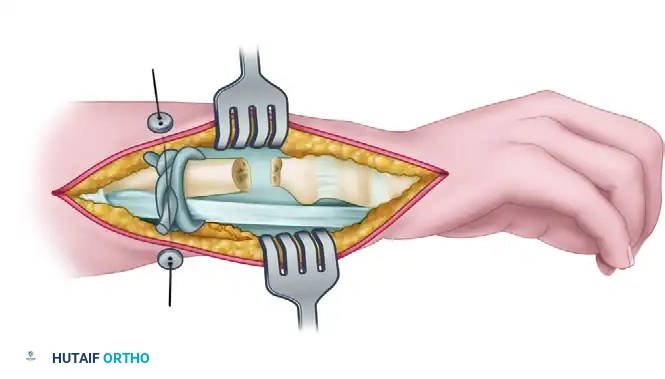
Figure: Bunnell technique for restoring stability of the distal ulna after excessive bone resection. The tendon graft loops around the ulna and FCU, secured by a running removable wire.
ALTERNATIVE PROCEDURES TO THE DARRACH RESECTION
Given the biomechanical drawbacks of complete ulnar head resection, several alternative procedures have been developed to preserve DRUJ kinematics while eliminating pain.
Partial Distal Ulnar Resection (Bowers Hemiresection Interposition Arthroplasty)
Preferred for active patients with DRUJ arthritis associated with distal radial malunions. The Bowers procedure involves resecting only the articulating portion of the ulnar head (the radial aspect) while preserving the ulnar styloid, the TFCC, and the ulnocarpal ligaments. A soft tissue interposition (usually dorsal capsule or an extensor retinaculum flap) is placed into the dead space.
Advantage: Preserves the ulnocarpal sling and prevents ulnar translation.
Requirement: Must be avoided if the TFCC is incompetent. If positive ulnar variance exists, an ulnar shortening osteotomy must be performed concurrently to prevent ulnocarpal impingement.
Sauvé-Kapandji Procedure
The Sauvé-Kapandji technique involves an arthrodesis (fusion) of the DRUJ combined with a proximal ulnar pseudarthrosis (creation of a surgical nonunion just proximal to the fusion).
Advantage: Allows restoration of forearm rotation through the pseudarthrosis while completely eliminating DRUJ pain. Crucially, the ulnar carpal ligaments and the bony support of the carpus are entirely preserved.
Indication: Highly recommended for younger, higher-demand patients with fixed radioulnar joint subluxation and concomitant joint destruction.
Ulnar Styloid Osteotomy for Malunion
In some clinical scenarios, dorsal dislocation of the DRUJ is driven entirely by a malunion of an ulnar styloid fracture (often seen in association with Galeazzi, Colles, or Smith fractures). Because the TFCC inserts on the proximal half of the ulnar styloid, a displaced styloid base fracture pulls the TFCC and destabilizes the joint.
Patients present with ulnar-sided wrist pain, restricted rotation, and weakness. CT imaging typically reveals dorsal DRUJ dislocation and palmar/proximal displacement of the styloid fragment.
Nakamura Technique:
Rather than resecting the ulna, Nakamura et al. recommend an intra-articular osteotomy.
1. An ulnar incision exposes the malunited styloid base.
2. An osteotomy is performed to mobilize the styloid fragment.
3. The fragment (with the attached TFCC) is translocated ulnarly to anatomically reduce the DRUJ.
4. Fixation is achieved with a tension band construct and two 0.062-inch Kirschner wires.
5. If positive ulnar variance is present, a concurrent ulnar shortening diaphyseal osteotomy is performed.
Postoperative Protocol: A long-arm cast is applied for 2 weeks to control rotation, followed by a short-arm cast for an additional 6 weeks to allow osseous union of the styloid.
CONCLUSION
The resection of the distal ulna remains a powerful tool in the orthopedic surgeon's armamentarium. While the Darrach procedure has largely been superseded by joint-preserving techniques in young, active patients, it provides reliable, definitive pain relief and functional restoration in the elderly or low-demand population. Mastery of the surgical anatomy, strict adherence to resection limits (maximum 2.5 cm), and meticulous soft-tissue reconstruction are imperative to avoid the crippling complication of ulnar stump instability. When complications do arise, techniques such as the Bunnell tendon weave provide robust salvage options to restore forearm kinematics.
