Comprehensive Introduction and Patho-Epidemiology
The distal tibiofibular syndesmosis represents a highly specialized, critical ligamentous complex fundamentally responsible for maintaining the structural integrity, dynamic stability, and functional congruence of the ankle mortise. Acute rupture of these structures, most frequently occurring via high-energy external rotation forces applied to a dorsiflexed foot, precipitates syndesmotic diastasis and profound biomechanical instability. This injury pattern is classically observed in the Lauge-Hansen pronation-external rotation (PER) and supination-external rotation (SER) fracture sequences, as well as in isolated "high ankle sprains" prevalent among elite collision-sport athletes. The epidemiological burden of syndesmotic injuries is substantial, complicating approximately 10% to 13% of all operatively treated ankle fractures, with the incidence rising to over 20% in patients requiring internal fixation for rotational ankle trauma.
The pathophysiological consequences of an unrecognized or inadequately treated syndesmotic rupture are devastating to the articular cartilage of the tibiotalar joint. The landmark biomechanical study by Ramsey and Hamilton demonstrated that even a seemingly innocuous 1-mm lateral shift of the talus within the mortise decreases the tibiotalar articular contact area by an astonishing 42%. This precipitous loss of contact area exponentially increases peak articular contact pressures, shifting the load-bearing axis to the medial talar dome and lateral tibial plafond. Consequently, the chondrocytes are subjected to supraphysiologic shear and compressive forces, predisposing the patient to rapid-onset, inexorable post-traumatic osteoarthritis.
Given the unforgiving biomechanical environment of the ankle joint, the primary and unwavering objective of surgical intervention is the precise, three-dimensional anatomical reduction of the fibula within the tibial incisura (incisura fibularis). This reduction must be rigidly or semi-rigidly maintained until robust ligamentous healing occurs via secondary intention. Historically, the orthopedic community accepted minor degrees of malreduction; however, contemporary outcome studies have irrefutably established that anatomical reduction of the syndesmosis is the single most critical prognostic factor dictating both subjective patient-reported outcomes and objective functional recovery.
Failure to restore the precise anatomical relationship, particularly in the sagittal plane or regarding the rotational alignment of the fibula, is the leading etiology of intractable postoperative pain, chronic instability, and early arthrodesis. The modern orthopedic surgeon must therefore approach acute distal tibiofibular syndesmosis ruptures with a high index of suspicion, utilizing advanced imaging modalities and meticulous intraoperative techniques to ensure absolute anatomical restoration of the mortise.
Detailed Surgical Anatomy and Biomechanics
A profound comprehension of the surgical anatomy and biomechanics of the distal tibiofibular articulation is paramount for the operating surgeon. The syndesmosis is not a static hinge but a dynamic, multi-ligamentous amphiarthrodial joint that accommodates the complex kinematics of the talus during the normal gait cycle. The osseous architecture is defined by the incisura fibularis of the distal tibia—a concave, triangular groove bounded by the anterior and posterior tibial tubercles. The morphology of the incisura is highly variable; it can be shallow or deep, which significantly influences the inherent osseous stability of the joint and the propensity for iatrogenic malreduction during clamp application.
The soft-tissue envelope securing the fibula within the incisura is composed of four distinct ligamentous structures. The anterior inferior tibiofibular ligament (AITFL) originates from the anterior tibial tubercle (Chaput's tubercle) and courses obliquely to insert on the anterior aspect of the lateral malleolus (Wagstaffe's tubercle). It is the weakest of the syndesmotic ligaments but is the first to fail in external rotation injuries. The posterior inferior tibiofibular ligament (PITFL) is a much thicker, more robust structure originating from the posterior tibial tubercle (Volkmann's triangle) and inserting on the posterior fibula. The PITFL provides the majority of the posterior translational stability to the fibula.
Deep to the PITFL lies the transverse ligament, which functions as a labrum, deepening the posterior aspect of the tibial plafond and preventing posterior talar subluxation. Finally, the interosseous ligament (IOL), a distal thickening of the interosseous membrane, acts as a primary "spring" ligament. The IOL neutralizes axial loads and limits the proximal migration of the fibula during weight-bearing. Biomechanical sectioning studies by Ogilvie-Harris et al. quantified the relative contributions of these ligaments to syndesmotic stability: the AITFL contributes approximately 35%, the deep transverse ligament 33%, the IOL 22%, and the PITFL 9%.
During normal physiological gait, particularly transitioning from plantarflexion to maximum dorsiflexion, the wider anterior dome of the talus engages the mortise. To accommodate this, the syndesmosis must undergo dynamic expansion. The fibula externally rotates approximately 2 to 5 degrees, translates laterally by 1 to 2 millimeters, and migrates proximally. Rigid metallic trans-syndesmotic fixation eliminates this physiological micromotion, which explains the high incidence of screw loosening or breakage upon the resumption of full weight-bearing. Understanding these kinematics is the foundational rationale for the increasing utilization of dynamic suture button constructs, which secure the mortise while permitting physiological fibular motion.
Exhaustive Indications and Contraindications
The decision to proceed with operative repair of an acute distal tibiofibular syndesmosis rupture requires a meticulous synthesis of clinical examination findings, radiographic parameters, and patient-specific functional demands. Not all syndesmotic injuries necessitate surgical intervention; stable, isolated grade I or II sprains without frank diastasis can often be managed with functional bracing and aggressive physical therapy. However, when the structural integrity of the mortise is compromised, operative stabilization becomes mandatory to avert catastrophic joint degeneration.
Absolute indications for operative intervention include frank syndesmotic diastasis visible on static non-weight-bearing radiographs, bimalleolar or trimalleolar equivalent fracture-dislocations (such as Lauge-Hansen PER stage IV injuries), and proximal fibular shaft fractures associated with medial clear space widening (the classic Maisonneuve injury). Furthermore, any Weber B or C lateral malleolar fracture that demonstrates dynamic instability upon intraoperative stress testing (the "Cotton test" or external rotation stress test) mandates trans-syndesmotic fixation. In the context of isolated ligamentous injuries without fracture, surgical repair is indicated when there is dynamic widening of the tibiofibular clear space on stress radiographs, or when conservative management has failed to resolve chronic functional instability.
Relative indications encompass high-demand elite athletes with severe grade III isolated syndesmotic sprains. In this demographic, prolonged conservative management may result in unacceptable delays in returning to play or subtle chronic micro-instability that impairs athletic performance. In such cases, early stabilization with dynamic suture button constructs is increasingly favored to accelerate rehabilitation and provide definitive mechanical support to the healing ligaments.
Contraindications to surgical intervention must be carefully respected to avoid devastating postoperative complications. Absolute contraindications include active local or systemic infection, critically compromised soft tissue envelopes (e.g., severe fracture blisters, massive edema lacking the "wrinkle sign"), and non-ambulatory patients in whom the physiological demands on the ankle are negligible. Severe peripheral vascular disease and uncontrolled diabetes mellitus represent profound relative contraindications, as the risk of wound dehiscence, deep infection, and subsequent amputation may outweigh the biomechanical benefits of anatomical mortise restoration.
| Indication Category | Specific Clinical / Radiographic Criteria | Rationale for Operative Management |
|---|---|---|
| Absolute Indications | Frank diastasis on static AP/Mortise radiographs | Prevents rapid-onset articular cartilage degradation |
| Maisonneuve fracture with medial clear space >4mm | Restores length and rotational alignment of the fibula | |
| Positive intraoperative Cotton / ER stress test | Addresses occult dynamic instability post-fracture fixation | |
| Lauge-Hansen PER Stage IV / Weber C fractures | High probability of complete IOM and syndesmotic disruption | |
| Relative Indications | Elite athlete with Grade III isolated syndesmotic tear | Accelerates return to sport; prevents chronic micro-instability |
| Delayed presentation with persistent pain/instability | Salvages joint mechanics before irreversible arthrosis occurs | |
| Contraindications | Severe soft tissue compromise (e.g., fracture blisters) | High risk of wound necrosis and deep space infection |
| Active localized soft tissue or intra-articular infection | Absolute contraindication to internal hardware placement | |
| Severe peripheral neuropathy / Charcot arthropathy | High risk of hardware failure; requires specialized salvage framing |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful syndesmotic reconstruction. Standard radiographic evaluation must include weight-bearing (if tolerated) anteroposterior (AP), lateral, and mortise views of the injured ankle. The surgeon must meticulously scrutinize three key radiographic parameters. First, the tibiofibular clear space, measured 1 cm proximal to the plafond, should be less than 5 mm on both AP and mortise views. Second, the tibiofibular overlap should be greater than 10 mm on the AP view and greater than 1 mm on the mortise view. Third, the medial clear space must be symmetric with the superior tibiotalar joint space; a medial clear space greater than 4 mm is highly indicative of lateral talar shift and concomitant deep deltoid ligament disruption.
In cases characterized by high clinical suspicion but equivocal static radiographs, gravity stress views or external rotation stress views are mandatory. However, the modern standard of care increasingly relies on advanced cross-sectional imaging. A preoperative computed tomography (CT) scan is highly recommended, particularly for complex fracture-dislocations, to assess the morphology of the incisura fibularis, identify occult osseous avulsions (e.g., Tillaux-Chaput or Volkmann fragments), and evaluate for subtle rotational malalignment that plain films routinely miss. Magnetic resonance imaging (MRI) is reserved for isolated ligamentous injuries to delineate the extent of AITFL, PITFL, and interosseous membrane tearing, as well as to diagnose concomitant intra-articular chondral lesions.
Preoperative templating involves determining the optimal trajectory for trans-syndesmotic fixation. The surgeon must plan for a drill trajectory angled approximately 20 to 30 degrees anteriorly from the lateral fibula to the medial tibia, accounting for the posterior position of the fibula relative to the central axis of the tibia. Implant selection—whether utilizing 3.5 mm or 4.5 mm cortical screws, or dynamic suture button constructs—must be finalized based on the patient's age, bone quality, athletic demands, and compliance with postoperative weight-bearing restrictions.
Patient positioning is critical for facilitating unhindered intraoperative fluoroscopy and surgical access. The patient is placed in the supine position on a fully radiolucent operating table. A bump is strategically placed under the ipsilateral hip to internally rotate the lower extremity, neutralizing the natural external rotation of the hip and bringing the lateral malleolus into a direct, easily accessible vertical orientation. A pneumatic thigh tourniquet is applied over copious padding to ensure a bloodless surgical field, which is essential for identifying delicate neurovascular structures and assessing articular reduction. The fluoroscopy unit (C-arm) should be positioned on the contralateral side of the table, allowing for seamless AP, mortise, and lateral imaging without compromising the sterile surgical field.
Step-by-Step Surgical Approach and Fixation Technique
Surgical Approach and Joint Preparation
The surgical approach to the distal tibiofibular joint must be meticulously executed to provide adequate exposure while preserving the delicate soft tissue envelope. A 5 to 7 cm longitudinal incision is made parallel to the anterior border of the distal fibula. This anterolateral approach allows for direct visualization of the distal tibiofibular joint, the AITFL, and the anterior aspect of the incisura. Dissection is carried sharply through the subcutaneous tissues. The surgeon must maintain a high state of vigilance to identify and protect the superficial peroneal nerve and its terminal branches, which frequently cross the surgical field in the proximal extent of the incision.
Once the extensor retinaculum is incised, the distal tibiofibular joint is exposed. Thorough debridement of the incisura fibularis is an absolute prerequisite for anatomical reduction. The surgeon must use a rongeur and curette to meticulously clear the incisura of organizing hematoma, interposed periosteum, or avulsed ligamentous debris (often remnants of the AITFL or interosseous ligament) that act as mechanical blocks to reduction. Suturing or primarily reattaching the ruptured AITFL is generally unnecessary; the primary biomechanical goal is rigid osseous stabilization, allowing the ligaments to heal via secondary intention under appropriate tension.
Anatomical Reduction and Clamp Application
Reduction of the syndesmosis is the most technically demanding phase of the procedure. The surgeon manually presses the fibula medially into the groove of the tibial incisura. This maneuver not only reduces the fibula but indirectly shifts the talus medially, restoring the medial clear space. Once manually reduced, a large reduction clamp (e.g., a Weber or pelvic reconstruction clamp) is applied to maintain the reduction.
The vector of clamp compression is of paramount importance. One tine is placed on the lateral ridge of the fibula, and the other is placed on the anteromedial aspect of the tibia. Because the fibula sits posterior to the mid-axial line of the tibia, the clamp must be angled approximately 20 to 30 degrees anteriorly from lateral to medial. Applying the clamp in a purely coronal plane will invariably result in iatrogenic anterior translation and internal rotation of the fibula out of the incisura. Furthermore, over-compression must be strictly avoided, as it can crush the fibula into the depths of the incisura, narrowing the mortise and severely restricting postoperative dorsiflexion.
Intraoperative Assessment and Addressing Soft Tissue Interposition
Before committing to drilling and fixation, the surgeon must use intraoperative fluoroscopy to meticulously assess the reduction. True AP, mortise, and lateral views are obtained. The surgeon should evaluate the Shenton's line of the ankle, the symmetry of the clear spaces, and the "dime sign" at the distal tip of the fibula. If the medial clear space remains widened despite lateral compression, a soft tissue structure is almost certainly obstructing the reduction of the talus.
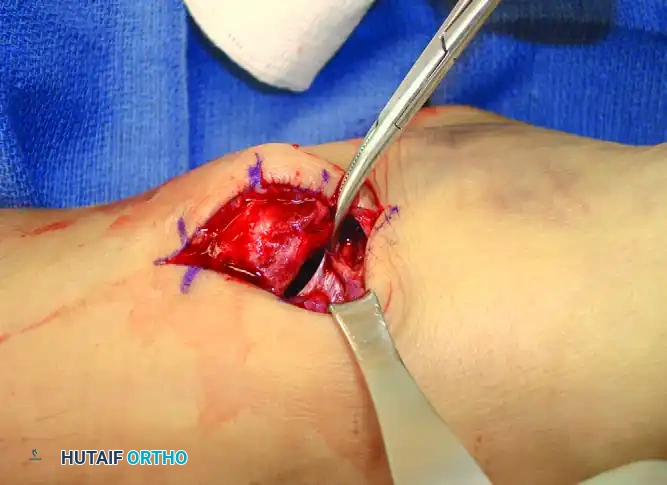
Figure: Deltoid ligament interposed and preventing reduction of the ankle fracture-dislocation. Note the widened medial clear space requiring direct medial exploration to extract the incarcerated ligament.
As illustrated above, the most common culprits for an irreducible medial clear space are an inverted, avulsed deep deltoid ligament or an interposed posterior tibial tendon. In such instances, a secondary medial incision centered over the medial malleolus is mandatory. The incarcerated soft tissues must be manually extracted from the joint space, allowing the talus to anatomically dock against the medial malleolus.
Trans-Syndesmotic Fixation Techniques
With the reduction confirmed and held securely by the clamp, fixation is applied under continuous fluoroscopic guidance. The drill trajectory must match the anatomical axis of the syndesmosis—directed 25 to 30 degrees anteromedially, starting from the posterolateral aspect of the fibula, approximately 2 to 3 cm proximal to the tibial plafond.
If utilizing metallic cortical screws, the surgeon may choose between 3.5 mm or 4.5 mm non-cannulated screws. The screws are inserted in a non-lagged fashion to act as position screws, maintaining the spatial relationship without inducing further compression. If the surgical plan includes eventual hardware removal, quadricortical purchase (engaging both fibular and both tibial cortices) is highly recommended. This ensures that if the screw breaks due to fatigue failure within the interosseous space, the medial tibial segment can be retrieved from the medial side.
Alternatively, dynamic suture button constructs have revolutionized the management of syndesmotic injuries. These devices consist of a heavy non-absorbable suture spanning between two metallic buttons resting on the lateral fibular and medial tibial cortices. Suture buttons provide semi-rigid fixation, maintaining anatomical reduction while permitting physiological micromotion (external rotation and lateral translation) of the fibula during dorsiflexion. This dynamic stabilization mitigates the risk of hardware breakage, negates the need for routine implant removal, and has been shown in multiple prospective randomized trials to yield superior early functional outcomes compared to static screw fixation.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, operative repair of the distal tibiofibular syndesmosis is associated with a significant complication profile. The most catastrophic complication is iatrogenic malreduction of the syndesmosis. Historically underreported on plain radiography, modern postoperative CT analyses reveal malreduction rates ranging from 15% to an alarming 39% in complex fracture-dislocations. Malreduction typically manifests as anterior sagittal translation or internal rotational deformity of the fibula within the incisura. This alters the contact mechanics of the tibiotalar joint, leading to persistent pain, stiffness, and accelerated osteoarthritis. Salvage of a malreduced syndesmosis requires early recognition, hardware removal, open debridement of the organized scar tissue within the incisura, and revision anatomical reduction, often augmented with intraoperative CT imaging.
Hardware-related complications are highly prevalent when rigid metallic screws are utilized. Screw loosening or breakage occurs in up to 30% of patients upon the resumption of weight-bearing, as the rigid implant succumbs to the cyclical physiological forces of the expanding mortise. While asymptomatic broken screws embedded within the bone do not routinely require extraction, symptomatic osteolysis or prominent screw heads necessitate surgical removal. Dynamic suture button constructs, while avoiding screw breakage, carry their own unique complications, including superficial soft tissue irritation from the lateral button knot, osteomyelitis, or button subsidence into osteoporotic bone, which can lead to late loss of reduction.
Infection and wound healing complications occur in approximately 3% to 5% of cases, heavily influenced by patient comorbidities such as smoking, diabetes, and the severity of the initial soft tissue trauma. Iatrogenic nerve injury, specifically to the superficial peroneal nerve or the sural nerve (during posterolateral approaches), results in painful neuromas or sensory deficits. Furthermore, tibiofibular synostosis (heterotopic ossification across the interosseous space) develops in up to 10% of cases. While often asymptomatic, massive synostosis can rigidly lock the fibula, restricting terminal dorsiflexion and causing chronic lateral column pain, necessitating delayed surgical excision of the bony bridge once it has fully matured.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Treatment |
|---|---|---|---|
| Syndesmotic Malreduction | 15% - 39% (CT verified) | Incorrect clamp vector; inadequate incisura debridement | Early revision open reduction; late cases may require arthrodesis |
| Hardware Breakage | 10% - 30% (Screw fixation) | Early weight-bearing on rigid screws; biological mortise expansion | Observation if asymptomatic; removal of symptomatic fragments |
| Tibiofibular Synostosis | 5% - 10% | Severe IOM tearing; bone debris left in interosseous space | Observation; surgical excision if causing severe pain/stiffness post-maturation |
| Superficial Peroneal Nerve Injury | 2% - 5% | Iatrogenic traction or transection during anterolateral approach | Gabapentinoids; surgical exploration and neuroma excision for refractory pain |
| Deep Surgical Site Infection | 1% - 3% | Severe soft tissue trauma; diabetes; smoking | Aggressive I&D; hardware removal if union achieved; targeted IV antibiotics |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following syndesmotic repair must delicately balance two competing biological imperatives: the absolute necessity for rigid immobilization to facilitate primary ligamentous healing, and the urgent need to initiate early motion to prevent debilitating tibiotalar and subtalar joint stiffness. The protocol is inherently dictated by the type of fixation utilized (static screws vs. dynamic suture buttons) and the presence of concomitant osseous fractures.
Phase I: Maximal Protection (0 to 2 Weeks)
Immediately postoperatively, the limb is placed in a well-padded, bulky posterior splint with a U-shaped stirrup, extending from the base of the toes to the tibial tuberosity. The ankle must be strictly immobilized in a neutral position (0 degrees of dorsiflexion) to prevent the rapid development of an Achilles tendon equinus contracture. The patient is instructed to remain strictly non-weight-bearing. Elevation of the limb above the level of the heart and the application of ice behind the knee are critical to mitigate postoperative edema and reduce the risk of wound dehiscence.
Phase II: Controlled Immobilization and Early Motion (2 to 6 Weeks)
At the 2-week follow-up, the splint is removed, and the surgical incisions are meticulously inspected for signs of necrosis or infection. Sutures or staples are removed. If static metallic screws were utilized, the patient is typically transitioned to a short-leg fiberglass cast and remains strictly non-weight-bearing for an additional 4 weeks to protect the rigid hardware from fatigue failure. Conversely, if dynamic suture button constructs were employed, the patient may be transitioned to a removable controlled ankle motion (CAM) walking boot. These patients are permitted to remove the boot multiple times daily to initiate active, non-weight-bearing range-of-motion (ROM) exercises, focusing on restoring sagittal plane dorsiflexion and plantarflexion, while strictly avoiding inversion and eversion stresses.
Phase III: Progressive Loading (6 to 10 Weeks)
At the 6-week mark, radiographic evaluation is performed to assess the maintenance of the mortise reduction and the progression of fracture healing (if applicable). Patients in casts are transitioned to a CAM boot. Progressive, partial weight-bearing is initiated, typically starting at 25% of body weight and advancing by 25% weekly under the guidance of a physical therapist. Hydrotherapy and stationary cycling are excellent modalities introduced during this phase to improve joint mobility and initiate early muscular reactivation without subjecting the syndesmosis to full axial loads.
Phase IV: Advanced Rehabilitation and Hardware Considerations (10 to 12+ Weeks)
By 10 to 12 weeks, patients should be weaning out of the CAM boot and transitioning to supportive athletic footwear. For patients treated with trans-syndesmotic screws, weight-bearing must remain restricted until the hardware is removed. Physiological mortise widening during weight-bearing dorsiflexion will inevitably cause rigid screws to loosen or catastrophically break within the tibiofibular joint space. Screw removal is typically performed as a brief outpatient procedure between 10 and 12 weeks postoperatively. Following screw extraction, or for patients treated with suture buttons, advanced functional rehabilitation commences. This phase focuses intensely on peroneal tendon strengthening, dynamic proprioceptive retraining using wobble boards, and plyometric exercises, which are essential to restore neuromuscular control and prevent chronic functional instability before clearing the patient for a return to high-impact sports or heavy labor.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for acute distal tibiofibular syndesmosis ruptures is deeply rooted in a robust body of biomechanical research and prospective clinical trials. The foundational understanding of syndesmotic biomechanics was established by Ramsey and Hamilton in 1976. Their seminal cadaveric study demonstrated that a mere 1-mm lateral displacement of the talus results in a 42% decrease in tibiotalar contact area. This singular finding fundamentally shifted orthopedic paradigms, establishing absolute anatomical reduction as the non-negotiable standard of care to prevent post-traumatic arthrosis.
The debate regarding the optimal level and rigidity of fixation was heavily influenced by Boden et al. in 1989. Their biomechanical analyses suggested that fixation placed 2 to 3 cm proximal to the plafond provided optimal stability without excessively tethering the joint. Furthermore, they demonstrated that rigid fixation of the syndesmosis was not strictly necessary if the medial malleolus was rigidly fixed, sparking decades of debate regarding the necessity of syndesmotic screws in the presence of stable deltoid or medial malleolar repairs.
In recent years, the literature has been dominated by the comparison between static metallic screws and dynamic suture button constructs. A landmark prospective, randomized multicenter trial by Sanders et al. compared the two modalities and found that patients treated with suture buttons demonstrated significantly improved early functional outcome scores (AOFAS and Olerud-Molander scores) and a drastically lower rate of hardware-related complications and reoperations. Similarly, Coetzee et al. highlighted that dynamic fixation allows for a more forgiving physiological reduction, reducing the incidence of catastrophic rigid malreduction seen with malpositioned clamps and screws.
Current clinical guidelines from the American Academy of Orthopaedic Surgeons (AAOS) and the American Orthopaedic Foot & Ankle Society (AOFAS) reflect this paradigm shift. The guidelines strongly recommend the use of intraoperative stress testing for all rotational ankle fractures to identify occult syndesmotic instability. Furthermore, while both screws and suture buttons remain acceptable standards of care, the guidelines increasingly support dynamic fixation, particularly in young, high-demand patients and athletes, due to the avoidance of secondary hardware removal surgeries and the facilitation of earlier functional rehabilitation. Surgeons are also strongly encouraged to utilize intraoperative or postoperative 3D imaging (CT) in complex cases, as plain radiography has been definitively proven inadequate for detecting subtle, yet clinically devastating, rotational malreductions of the fibula.
