Surgical Release of the Fibroosseous Tunnel and Flexor Hallucis Longus Management
Key Takeaway
Flexor hallucis longus (FHL) tendinitis and posterior ankle impingement often necessitate surgical release of the fibroosseous tunnel. This procedure involves decompressing the FHL tendon, excising the os trigonum, and restoring tendon excursion. Utilizing either a medial or lateral approach, surgeons must carefully navigate the posterior tibial neurovascular bundle or sural nerve. Complete release resolves functional hallux rigidus and restores biomechanical kinematics, particularly in high-demand athletes and dancers.
Introduction and Pathoanatomy
The flexor hallucis longus (FHL) tendon is a critical dynamic stabilizer of the medial longitudinal arch and the primary plantar flexor of the hallux interphalangeal joint. As the FHL tendon courses from the posterior compartment of the lower leg into the foot, it traverses a highly constrained fibroosseous tunnel. This tunnel begins at the posterior aspect of the talus, passing between the medial and lateral talar tubercles, and continues distally beneath the sustentaculum tali of the calcaneus.
In high-demand populations—most notably ballet dancers, gymnasts, and jumping athletes—repetitive extreme plantar flexion (such as the en pointe or demi-pointe positions) places immense mechanical stress on the FHL tendon and its surrounding retinacular sheath. This repetitive microtrauma frequently leads to stenosing tenosynovitis, hypertrophy of the tendon, and the formation of intratendinous nodules. When the thickened tendon or nodule becomes mechanically trapped at the proximal entrance of the fibroosseous tunnel, patients develop "hallux saltans" (triggering of the great toe) or functional hallux rigidus.
Furthermore, the presence of an os trigonum or an enlarged lateral talar tubercle (Stieda process) can exacerbate posterior ankle impingement. During forced plantar flexion, these osseous structures compress the FHL tendon and the posterior joint capsule between the posterior tibia and the calcaneus, necessitating surgical decompression and release of the fibroosseous tunnel.
Preoperative Evaluation and Imaging
A meticulous clinical examination is paramount. Patients typically present with posteromedial ankle pain that is exacerbated by push-off during gait or specific athletic maneuvers. Palpation posterior to the medial malleolus, specifically over the FHL sheath, often elicits tenderness. The "FHL stretch test"—passively dorsiflexing the ankle while simultaneously dorsiflexing the hallux—will frequently reproduce the patient's posteromedial pain.
Imaging is essential for surgical planning. Weight-bearing lateral radiographs of the ankle in maximal plantar flexion can demonstrate posterior osseous impingement and the presence of an os trigonum.

Magnetic Resonance Imaging (MRI) is the gold standard for evaluating the soft tissue integrity of the FHL tendon. MRI effectively delineates tenosynovitis (fluid within the tendon sheath), tendinosis, partial-thickness tears, and the exact location of any intratendinous nodules relative to the fibroosseous tunnel.

💡 Clinical Pearl
Always evaluate for functional hallux rigidus preoperatively. If the hallux lacks dorsiflexion when the ankle is in neutral or dorsiflexion, but regains motion when the ankle is plantar-flexed, the restriction is likely due to FHL tethering within the fibroosseous tunnel rather than primary metatarsophalangeal (MTP) joint osteoarthritis.
Surgical Approaches for Fibroosseous Tunnel Release
Surgical intervention is indicated following the exhaustion of conservative measures, which include nonsteroidal anti-inflammatory drugs (NSAIDs), physical therapy, immobilization, and judicious use of ultrasound-guided corticosteroid injections. The primary goals of surgery are to release the constricting retinaculum, perform a tenosynovectomy, excise any impinging osseous structures (os trigonum), and restore unhindered FHL excursion.
The Medial Approach
The medial approach is the workhorse incision for FHL decompression, offering excellent visualization of the tendon sheath and the posterior tibial neurovascular bundle.
Positioning and Preparation:
The patient is placed in the supine position with a bump under the contralateral hip to allow for external rotation of the operative leg. A thigh tourniquet is applied to ensure a bloodless surgical field.
Surgical Steps:
1. Incision: Make a 4-cm curvilinear incision posterior to the medial malleolus. The incision should be centered at the level of the superior border of the calcaneus, carefully following the anatomical course of the underlying neurovascular bundle.
2. Superficial Dissection: Deepen the incision through the subcutaneous tissue. Take meticulous care to identify and protect the medial calcaneal branches of the tibial nerve, which often cross the operative field.
3. Neurovascular Protection: Identify the flexor retinaculum (laciniate ligament). Incise the retinaculum to expose the posterior tibial artery, accompanying venae comitantes, and the tibial nerve. Retract the entire neurovascular bundle posteriorly using a blunt retractor (e.g., a Ragnell or mini-Hohmann retractor).
4. Identification of the FHL: The FHL tendon lies deep and slightly posterior to the neurovascular bundle. Confirm the identity of the FHL by passively flexing and extending the great toe; the tendon will be seen gliding within its sheath. Note that the flexor digitorum longus (FDL) lies anterior to the FHL.
5. Tunnel Release: Identify the proximal entrance of the fibroosseous tunnel. Often, the FHL will appear constricted at this exact entrance.

- Decompression: Using a blunt-tipped tenotomy scissor or a grooved director and a #15 blade, release the fibroosseous tunnel from proximal to distal. The release must extend completely to the level of the sustentaculum tali to ensure total decompression.
- Tendon Inspection and Debridement: Once the tunnel is open, inspect the tendon for tears, severe tendinosis, or nodules. Perform a thorough tenosynovectomy.

⚠️ Surgical Warning
Nodules on or within the flexor hallucis longus tendon usually should not be excised. Once the fibroosseous tunnel has been fully released, the excursion of the tendon is no longer restricted. Excising an intratendinous nodule risks creating a structural defect that could lead to iatrogenic tendon rupture.
- Os Trigonum Excision: Retract the released FHL tendon posteriorly alongside the neurovascular bundle. This exposes the posterior aspect of the talus. Identify the os trigonum or enlarged lateral tubercle on the lateral side of the entrance to the fibroosseous tunnel. Sharply dissect the capsular attachments and excise the osseous fragment.
- Dynamic Intraoperative Assessment: Evaluate for functional hallux rigidus intraoperatively. Dorsiflex the ankle to neutral and passively dorsiflex the great toe to ensure complete release and free excursion of the tendon. Examine the ankle in full plantar flexion to confirm that all bone or soft tissue impingement has been eradicated.
- Closure: Deflate the tourniquet and achieve meticulous hemostasis. The ankle should be held in a neutral position of flexion and extension during closure so that the skin edges align properly without undue tension. Close the subcutaneous tissue and skin in a standard layered fashion. The flexor retinaculum is left open to prevent recurrent stenosis.
The Lateral Approach
The lateral approach is highly advantageous for patients with concomitant lateral pathology, prominent lateral-sided impingement, or specific postural requirements. Because of the increased external rotation of the lower extremities commonly seen in classical dancers, the lateral approach is often preferred in this demographic.
Positioning and Preparation:
The patient is placed in the lateral decubitus position on the operating table. All bony prominences are padded, and a thigh tourniquet is utilized.
Surgical Steps:
1. Incision: Make a 4- to 5-cm curvilinear incision at the posterior aspect of the ankle mortise, running in line with the posterior border of the peroneal tendons.
2. Nerve Protection: The lesser saphenous vein and the sural nerve lie in the subcutaneous tissues near the incision. Meticulous blunt dissection is required to identify and protect the sural nerve, retracting it laterally or anteriorly as dictated by the specific anatomical variant.
3. Deep Dissection: Incise the deep fascia parallel to the peroneal tendons. Retract the peroneal tendons anteriorly.
4. Capsulotomy and Osseous Resection: Perform a posterior capsulotomy with the ankle held in slight dorsiflexion. Identify the lateral talar tubercle or the os trigonum, which lies lateral to the FHL tunnel. Excise the impinging bone using an osteotome or rongeur.
5. FHL Decompression: Once the bone is removed, the lateral aspect of the FHL fibroosseous tunnel is visualized. The tunnel can be released under direct vision.
6. Impingement Assessment: Assess for adequate osseous decompression by maximally plantar flexing the foot and palpating for any residual bone-on-bone impingement. Occasionally, loose bodies, calcaneal protuberances, or hypertrophic portions of the posterior tibial plafond need to be debrided.
7. Closure: Irrigate the wound copiously. Close the deep fascia, subcutaneous tissue, and skin.
Management of Flexor Hallucis Longus Tears (Technique 82-20)
While tenosynovitis and stenosis are common, frank rupture of the FHL is rare but debilitating. If the FHL is torn proximal to the metatarsophalangeal (MTP) joint such that the repair site will not glide smoothly through the pulley system, primary repair may be justified.
However, it is generally recommended not to repair this tendon within the pulley system of the hallux itself. If the flexor hallucis brevis (FHB) remains intact in the forefoot-midfoot area, repair of the FHL is often unnecessary for basic function. If the surgeon and patient elect to proceed with repair to restore maximal push-off strength, a plantar approach is required. The exposure on the plantar surface of the forefoot proximal to the MTP joint is anatomically complex.
Plantar Approach for FHL Repair
Positioning:
The patient is positioned supine. The hip and knee may be slightly flexed and externally rotated to allow direct access to the plantar aspect of the foot.
Surgical Steps:
1. Incision: Begin a plantar longitudinal incision on the sole of the foot between the first and second metatarsals, just lateral and distal to the fibular sesamoid. Continue this incision proximally for 4 to 5 cm.
- Fascial Dissection: Deepen the incision through the thick plantar fat pad. Bluntly remove the fibrous connections between the slips of the plantar fascia that extend to the first and second toes.
- Neurovascular Identification: Using small, blunt-tipped dissecting scissors, carefully expose the common digital nerve and its accompanying vessels leading to the first web space.

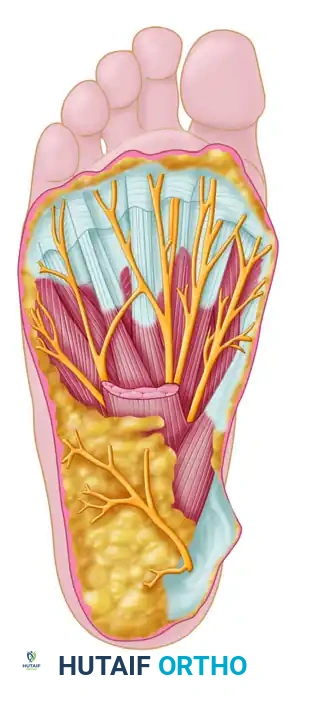
💡 Anatomical Landmark
The medial proper branch of the medial plantar nerve courses to the tibial side of the hallux (1), while the common digital branch of the medial plantar nerve courses to the first web space (2). The FHL tendon (3) lies deep to these structures.
- Retraction: Gently retract the common digital nerve and vessels laterally and toward the distal part of the wound. This maneuver exposes the lateral head of the flexor hallucis brevis (FHB) tendon.
- Tendon Retrieval: Develop the anatomical plane between the two muscle bellies of the FHB throughout the length of the wound. Acutely flex the great toe; this action should cause the distal tendon stump of the FHL to appear in the wound, guiding the surgeon toward the optimal repair site.
- Repair: Retrieve the proximal stump (which may require a separate medial midfoot incision near the Master Knot of Henry if it has retracted significantly). Perform a robust core suture repair (e.g., Krackow or modified Kessler technique) using non-absorbable suture.
- Closure: Ensure hemostasis. Close the plantar fascia loosely, followed by meticulous closure of the plantar skin using interrupted non-absorbable vertical mattress sutures to withstand weight-bearing forces.
Postoperative Care and Rehabilitation Protocol
The postoperative rehabilitation protocol is designed to protect the surgical site while preventing restrictive adhesions of the FHL tendon.
Phase I: Immediate Postoperative (Weeks 0-1)
* A bulky, sterile compression dressing and a posterior plaster splint are applied in the operating room with the ankle in neutral.
* The patient is allowed weight-bearing as tolerated (WBAT) with the assistance of crutches, utilizing a rigid postoperative boot if a simple release was performed. (Note: If an FHL repair was performed, the patient is strictly non-weight-bearing for 4-6 weeks).
* Strict elevation is encouraged to minimize edema and promote wound healing.
Phase II: Early Mobilization (Weeks 1-2)
* The initial compression dressing is removed at 1 week postoperatively.
* Wound evaluation is performed.
* Active range of motion (AROM) of the ankle and great toe is initiated immediately as tolerance to pain permits. Early motion is critical to prevent the FHL tendon from scarring to the surrounding tissues or the released retinaculum.
Phase III: Physical Therapy and Strengthening (Weeks 2-6)
* At 2 weeks, sutures are removed.
* The patient begins formal physical therapy consisting of progressive active and passive range-of-motion exercises.
* Strengthening exercises for the intrinsic foot musculature, peroneal tendons, and posterior calf are introduced.
* Swimming and stationary cycling are highly encouraged once the surgical wound has completely healed and sealed.
Phase IV: Return to Activity (Weeks 6+)
* The patient is progressed to higher levels of activity, including plyometrics and sport-specific drills, under the direct supervision of a physical therapist.
* For dancers, a gradual return to demi-pointe and eventually en pointe is guided by pain tolerance and the restoration of symmetric strength.
* An average of 6 months should be expected for full recovery and return to elite-level athletic or dance performance, though many patients experience significant pain relief much earlier in the postoperative course.
You Might Also Like
