Introduction to Recurrent Joint Instability
The management of recurrent joint instability demands a profound understanding of articular biomechanics, dynamic muscular restraints, and static ligamentous anatomy. Chronic instability not only severely limits patient function but also predictably leads to early-onset osteoarthritis due to abnormal contact stresses and chondral shear forces. This masterclass synthesizes the foundational evidence base—spanning classic anatomical studies to contemporary kinematic analyses—to provide a definitive, step-by-step surgical guide for addressing recurrent instability in the patellofemoral joint, the elbow, and the hip.
Designed for the practicing orthopedic consultant and advanced fellow, this text details the indications, pathoanatomy, surgical techniques, and postoperative protocols required to achieve durable, biomechanically sound joint reconstruction.
Part I: Patellofemoral Instability
Patellofemoral instability is a multifactorial pathology driven by osseous dysplasia, ligamentous incompetence, and malalignment. The medial patellofemoral ligament (MPFL) is the primary restraint to lateral patellar translation at early flexion (0° to 30°). Once the knee flexes beyond 30°, the patella engages the trochlear groove, and osseous geometry dictates stability.
Biomechanics and Pathoanatomy
Historically, procedures such as isolated lateral retinacular release or non-anatomic tenodesis (e.g., Roux-Goldthwait) yielded unpredictable long-term results. Contemporary evidence dictates that isolated lateral release is contraindicated for primary instability without a tight lateral retinaculum. Instead, anatomic MPFL reconstruction, combined with tibial tubercle osteotomy (TTO) when indicated by an abnormal tibial tubercle-trochlear groove (TT-TG) distance, represents the gold standard.
Clinical Pearl: A TT-TG distance greater than 20 mm on axial CT or MRI is a strong indication for a medializing tibial tubercle osteotomy (e.g., Elmslie-Trillat procedure). If concurrent patellofemoral chondrosis is present, an anteromedialization osteotomy (Fulkerson procedure) is preferred to offload the distal and lateral patellar facets.
Medial Patellofemoral Ligament (MPFL) Reconstruction
Indications
- Recurrent lateral patellar dislocation.
- Failure of conservative management (physiotherapy, bracing).
- Incompetent MPFL with normal osseous alignment (TT-TG < 15-20 mm, normal patellar height).
Patient Positioning and Preparation
- Place the patient supine on a radiolucent operating table.
- Apply a high thigh tourniquet.
- Position the operative leg in a leg holder allowing full, unencumbered range of motion from 0° to 120° of flexion.
- Perform a diagnostic arthroscopy to evaluate chondral surfaces and remove any loose bodies resulting from osteochondral shear fractures during dislocation.
Surgical Technique: Step-by-Step
- Graft Harvest: Harvest the semitendinosus tendon using a standard anteromedial tibial incision. Whipstitch both ends of the graft with non-absorbable #2 suture.
- Patellar Preparation: Make a 2-3 cm longitudinal incision over the medial border of the upper half of the patella. Dissect down to the extensor retinaculum. Create a subperiosteal trough or drill two transverse 3.2 mm blind tunnels in the proximal two-thirds of the medial patellar edge.
- Femoral Isometric Point Identification: This is the most critical step. Make a 2 cm incision between the medial epicondyle and the adductor tubercle.
- Radiographic Landmark (Schöttle's Point): On a strict lateral fluoroscopic view, the femoral attachment lies 1 mm anterior to the posterior cortex extension line, 2.5 mm distal to the posterior origin of the medial femoral condyle, and proximal to the level of the posterior point of Blumensaat's line.
- Graft Routing: Pass the graft from the patella to the femoral incision between the capsule (layer 2) and the deep fascia (layer 1).
- Fixation: Secure the graft to the patella using suture anchors or interference screws. Loop the graft around a guide pin at the femoral isometric point.
- Tensioning: Cycle the knee through a full range of motion. The graft should be tensioned at 30° of flexion to restore the anatomic check-rein effect without over-constraining the medial compartment. Secure the femoral side with a bioabsorbable interference screw.
Surgical Warning: Over-tensioning the MPFL graft is the most common cause of surgical failure, leading to severe medial patellofemoral articular overload, pain, and iatrogenic medial subluxation. The graft should act as a "seatbelt," engaging only when lateral translation forces are applied.
Tibial Tubercle Osteotomy (Fulkerson Anteromedialization)
Indications
- Recurrent instability with a TT-TG distance > 20 mm.
- Patella alta (Caton-Deschamps index > 1.2).
- Concomitant lateral or distal patellofemoral chondral lesions.
Surgical Technique
- Approach: Make a longitudinal incision lateral to the tibial crest. Expose the anterior compartment musculature and elevate it off the lateral tibia.
- Osteotomy: Use an oscillating saw to create an oblique osteotomy starting proximal to the patellar tendon insertion and exiting distally along the anterior tibial crest (typically 5-7 cm in length). The angle of the cut dictates the ratio of anteriorization to medialization (a steeper angle provides more anteriorization).
- Displacement: Translate the tubercle medially (to correct TT-TG) and anteriorly (to decompress the joint).
- Fixation: Temporarily pin the tubercle and verify tracking arthroscopically. Fix the osteotomy rigidly with two 4.5 mm cortical lag screws directed from anterior to posterior.
Postoperative Protocol (Patellofemoral Realignment)
- Weeks 0-2: Knee immobilized in extension in a hinged brace. Weight-bearing as tolerated with crutches in extension. Passive ROM 0°-30°.
- Weeks 2-6: Gradually increase ROM to 90°. Initiate isometric quadriceps strengthening.
- Weeks 6-12: Discontinue brace once quadriceps control is adequate. Progress to closed-chain kinetic exercises.
- Months 4-6: Return to sport-specific activities following functional testing.
Part II: Posterolateral Rotatory Instability (PLRI) of the Elbow
Recurrent instability of the elbow is most frequently manifested as Posterolateral Rotatory Instability (PLRI), resulting from insufficiency of the Lateral Ulnar Collateral Ligament (LUCL). This pathology often follows a traumatic elbow dislocation where the lateral ligamentous complex fails to heal isometrically.
Anatomy and Biomechanics of the Lateral Collateral Complex
The lateral collateral ligament (LCL) complex is the primary stabilizer against varus and external rotatory stress. It consists of the radial collateral ligament (RCL), the lateral ulnar collateral ligament (LUCL), and the annular ligament.
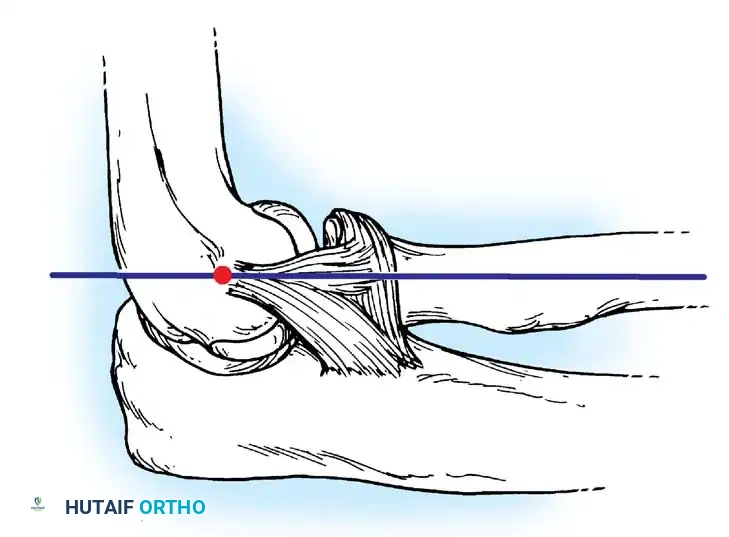
Fig. 45-70 Lateral collateral and annular ligament complex of elbow. Lateral collateral ligament originates off humerus at axis point of ulnohumeral joint, which lies at intersection of anterior humeral line and radiocapitellar axis. Radial collateral ligament blends with annular ligament to insert in conjoined fashion onto proximal ulna. (Redrawn from Cohen MS, Bruno RJ: The collateral ligaments of the elbow, Clin Orthop Relat Res 383:123, 2001.)
The LUCL acts as a hammock supporting the radial head. When incompetent, the radius and ulna supinate and subluxate posterolaterally away from the humerus, pivoting on the intact medial collateral ligament (MCL).
LUCL Reconstruction
Indications
- Symptomatic recurrent PLRI (giving way with pushing off a chair or doing push-ups).
- Positive lateral pivot-shift test or posterolateral rotatory apprehension test.
Patient Positioning
- Position the patient supine with the arm draped across the chest, or in the lateral decubitus position with the arm over a radiolucent post.
- Apply a sterile tourniquet.
Surgical Technique: Step-by-Step
- Approach: Utilize a Kocher approach (between the anconeus and extensor carpi ulnaris). Elevate the common extensor origin anteriorly to expose the lateral epicondyle and the radiocapitellar joint.
- Identifying the Isometric Point: The femoral origin of the LUCL is at the isometric point on the lateral epicondyle, located at the center of the capitellar curvature.
- Ulnar Tunnels: Identify the supinator crest of the ulna. Drill two converging 3.2 mm tunnels at the anatomic insertion of the LUCL, leaving a 1 cm bone bridge.
- Humeral Tunnel: Drill a blind tunnel or converging tunnels at the isometric point on the lateral epicondyle.
- Graft Preparation and Passage: A palmaris longus or gracilis autograft is preferred. Pass the graft through the ulnar tunnels. Route the limbs proximally to the humeral tunnel.
- Tensioning and Fixation: Tension the graft with the elbow in 30° to 40° of flexion and full pronation (to reduce the posterolateral subluxation). Secure the graft in the humeral tunnel using an interference screw or suture anchors.
Clinical Pearl: Always tension the LUCL graft with the forearm in maximum pronation. Pronation tightens the medial soft tissues and perfectly reduces the radiocapitellar joint, ensuring the graft is fixed in the anatomic position.
Postoperative Protocol
- Weeks 0-2: Splint the elbow in 90° of flexion and full pronation.
- Weeks 2-6: Transition to a hinged elbow brace locked in pronation. Allow active ROM from 30° to 130°. Avoid terminal extension and supination, which stress the LUCL reconstruction.
- Weeks 6-12: Wean from the brace. Begin strengthening.
- Months 4-6: Return to unrestricted heavy lifting and sports.
Part III: Recurrent Dislocation of the Hip
Recurrent dislocation of the hip is a rare but devastating complication, typically occurring post-traumatically due to massive capsulolabral disruption, posterior wall acetabular fractures, or unrecognized intra-articular pathology. Atraumatic recurrent dislocations are exceedingly rare and are usually associated with connective tissue disorders or severe dysplasia.
Pathoanatomy
The hip is an inherently stable ball-and-socket joint. Recurrent instability implies a catastrophic failure of the static restraints:
1. Osseous defects: Ununited posterior wall fractures or femoral head impaction fractures.
2. Capsulolabral incompetence: A "Bankart-type" lesion of the hip, where the posterior capsule and labrum are avulsed from the acetabular rim.
3. Intra-articular loose bodies: Preventing concentric reduction and acting as a fulcrum for levering the hip out of the socket.
Surgical Management: Capsulolabral Reconstruction
Indications
- Recurrent posterior hip dislocation without massive osseous defects (which would require structural bone grafting or osteosynthesis).
- Demonstrable posterior capsular avulsion or labral tear on MR arthrography.
Patient Positioning
- Place the patient in the lateral decubitus position on a radiolucent table.
- Ensure rigid pelvic fixation with anterior and posterior supports.
Surgical Technique: Step-by-Step
- Approach: Utilize a standard Kocher-Langenbeck approach. Split the gluteus maximus in line with its fibers. Identify and protect the sciatic nerve throughout the procedure.
- Deep Dissection: Tenotomize the short external rotators (piriformis, obturator internus, gemelli) near their femoral insertion and reflect them posteriorly over the sciatic nerve to act as a protective cushion.
- Capsulotomy and Joint Inspection: Perform a T-shaped capsulotomy if the capsule is intact but redundant. If the capsule is avulsed from the acetabulum, utilize the traumatic rent. Distract the hip and meticulously clear all intra-articular loose bodies and debris.
- Acetabular Preparation: Debride the posterior acetabular rim to bleeding cancellous bone to promote healing.
- Labral and Capsular Repair (Modified Bankart): Place 2 to 3 suture anchors along the posterior-superior and posterior-inferior acetabular rim. Pass the sutures through the labrum and the thick posterior capsule.
- Capsular Plication: Tie the sutures with the hip held in slight extension, abduction, and external rotation to maximally tension the posterior capsular repair. If capsular redundancy is severe, perform a capsular shift by advancing the inferior leaflet superiorly.
- Closure: Repair the short external rotators anatomically to their femoral insertions to provide an additional dynamic buttress against posterior translation.
Surgical Warning: The sciatic nerve is at extreme risk during posterior hip reconstruction, particularly in the setting of dense scar tissue from previous trauma. Meticulous neurolysis and continuous protection of the nerve are mandatory before addressing the capsulolabral structures.
Postoperative Protocol
- Weeks 0-6: Patient is placed in an abduction brace limiting flexion to 70°, with 0° of internal rotation and 0° of adduction. Touch-down weight-bearing only.
- Weeks 6-12: Discontinue brace. Progress to partial, then full weight-bearing. Initiate active-assisted range of motion, strictly avoiding the combined position of flexion, adduction, and internal rotation.
- Months 3-6: Focus on abductor and external rotator strengthening. Return to high-impact activities is generally restricted until 6 to 9 months postoperatively, contingent upon radiographic joint congruity and clinical stability.
Conclusion
The surgical management of recurrent joint instability requires a highly tailored approach based on the specific pathoanatomy of the patient. Whether addressing the patellofemoral joint via MPFL reconstruction and TTO, the elbow via isometric LUCL reconstruction, or the hip via complex capsulorrhaphy, the overarching principles remain identical: restore anatomic alignment, re-establish isometric ligamentous tension, and respect the delicate balance of joint kinematics. Adherence to these evidence-based techniques ensures optimal functional recovery and mitigates the risk of progressive articular degeneration.
