Comprehensive Management of Extensor Mechanism Injuries: Boutonnière Deformity, Zone IV-V Lacerations, and Sagittal Band Ruptures
Key Takeaway
Chronic boutonnière deformities, Zone IV-V lacerations, and sagittal band ruptures present complex challenges in hand surgery. This comprehensive guide details the modified Littler technique for centralizing lateral bands, evidence-based core suture repairs for proximal phalanx and metacarpophalangeal joint injuries, and the Rayan and Murray classification for traumatic extensor tendon dislocations. Mastery of these pathoanatomical principles ensures optimal restoration of digital kinematics and function.
INTRODUCTION TO EXTENSOR MECHANISM PATHOLOGY
The extensor mechanism of the digits is a highly intricate, finely balanced system of intrinsic and extrinsic tendinous contributions. Disruption of this delicate equilibrium—whether through chronic attenuation, acute laceration, or traumatic dislocation—results in predictable, often debilitating kinematic failures. Mastery of extensor tendon anatomy across the defined zones (particularly Zones IV and V) and an in-depth understanding of the pathoanatomy driving conditions such as the chronic buttonhole (boutonnière) deformity and sagittal band ruptures are mandatory for the practicing hand surgeon.
This comprehensive masterclass delineates the evidence-based surgical management of these complex extensor mechanism pathologies, providing step-by-step technical guidance for reconstruction, repair, and postoperative rehabilitation.
RECONSTRUCTION OF THE EXTENSOR MECHANISM FOR CHRONIC BUTTONHOLE DEFORMITY
The boutonnière (buttonhole) deformity is characterized by flexion of the proximal interphalangeal (PIP) joint and hyperextension of the distal interphalangeal (DIP) joint. Pathoanatomically, it is initiated by the disruption or severe attenuation of the central slip at its insertion on the base of the middle phalanx. Over time, the triangular ligament stretches, allowing the lateral bands to subluxate volarly past the axis of rotation of the PIP joint. Once volarly displaced, the lateral bands act as PIP flexors rather than extensors. Concurrently, the transverse retinacular ligaments contract, tethering the lateral bands in their abnormal volar position and driving the DIP joint into rigid hyperextension.
When conservative management (e.g., dynamic splinting, serial casting) fails, or when the deformity becomes chronic and fixed, surgical reconstruction is indicated. The modified Littler technique is a highly reliable procedure designed to release the contracted transverse retinacular ligaments, mobilize the lateral bands, and centralize them dorsally to restore PIP joint extension without sacrificing active DIP joint extension.
Preoperative Considerations and Indications
Surgical reconstruction is indicated for chronic boutonnière deformities where the PIP joint remains passively correctable (supple) but lacks active extension. If the PIP joint is rigidly contracted, a preliminary phase of serial casting or a surgical joint release (capsulectomy) must precede or accompany the tendon reconstruction.
Clinical Pearl: The success of a soft-tissue extensor reconstruction hinges entirely on the preoperative passive mobility of the PIP joint. Attempting a tendon transfer or centralization in the presence of a fixed volar plate contracture will uniformly fail.
Surgical Technique: The Modified Littler Reconstruction
The modified Littler technique elegantly restores the extensor mechanism by repurposing the volarly subluxated lateral bands, shifting them dorsally to recreate the function of the deficient central slip.
1. Incision and Exposure
* Perform a dorsal curved or lazy-S incision centered directly over the PIP joint. This approach prevents postoperative scar contracture from limiting joint flexion.
* Elevate the skin flaps carefully, preserving the dorsal venous network.
* Identify the attenuated central tendon, the volarly displaced lateral bands, and the contracted transverse retinacular ligaments.
2. Dissection of the Transverse Retinacular Ligaments
* Using the fine point of a surgical probe, dissect deep to each transverse retinacular ligament. Trace the ligament from its origin near the volar plate to its insertion on the lateral border of the lateral band.
* Using small tenotomy scissors, sharply divide each transverse retinacular ligament near its midportion. This critical step releases the tethering force holding the lateral bands in their volar position.
3. Mobilization of the Lateral Bands
* Free the insertions of the lateral bands bilaterally so they can be mobilized and replaced dorsally over the PIP joint.
* Crucial Step: On the radial side, perform sharp dissection to separate the bands, but strictly leave intact the radial-most fibers of the lateral band. These fibers represent the terminal contribution of the lumbrical muscles and the oblique retinacular ligament.
* Preserving these radial fibers is paramount; it ensures the preservation of active extension at the distal interphalangeal (DIP) joint.
Surgical Warning: Overzealous resection or complete division of the radial lateral band will result in a severe extensor lag at the DIP joint, trading a PIP pathology for a DIP deficit.
4. Dorsal Shift and Fixation
* At this stage, the insertions of the lateral bands should be completely free, save for the preserved radial-most fibers of the radial lateral band.
* Shift both lateral bands dorsally and proximally.
* Suture the mobilized bands to the soft tissue and periosteum over the proximal third of the middle phalanx.
* Suture the bands to the attenuated central tendon. This repair must be performed with the PIP joint held in absolute, full extension to set the appropriate resting tension.
5. Joint Pinning and Closure
* To protect the delicate repair from early mechanical failure, support the reconstruction with a transarticular 0.045-inch Kirschner wire (K-wire). Place the wire obliquely across the PIP joint, maintaining it in full extension.
* Leave the divided transverse retinacular ligaments unsutured to prevent recurrent volar tethering.
* Close the skin wound using 5-0 interrupted monofilament nylon sutures.
Postoperative Rehabilitation Protocol
The K-wire is typically maintained for 3 to 4 weeks to allow primary healing of the centralized bands. Following pin removal, a strict regimen of dynamic extension splinting is initiated. Active flexion is introduced gradually, often utilizing a short-arc motion protocol to prevent stretching of the newly reconstructed central slip mechanism. Full unrestricted activity is generally delayed until 10 to 12 weeks postoperatively.
ZONE IV EXTENSOR TENDON INJURIES
Zone IV encompasses the extensor mechanism overlying the proximal phalanx. In this region, the extensor tendon is broad, flat, and wraps around the convexity of the phalanx. Because of this broad cross-sectional area, lacerations in Zone IV frequently result in incomplete (partial) tendon injuries.
Evaluation and Nonoperative Management
Clinical evaluation must carefully assess the degree of active PIP joint extension. Because the lateral bands and central slip begin to differentiate in this zone, a partial laceration may not completely ablate active extension.
- Closed Treatment: If the patient demonstrates full, active PIP joint extension against mild resistance, closed treatment is often sufficient. The digit is immobilized in an extension splint for 4 to 6 weeks.
- Operative Indication: If PIP joint extension is limited, weak, or accompanied by an extensor lag, surgical exploration is mandatory to determine the extent of the disruption and restore continuity.
Surgical Repair in Zone IV
When exploring a Zone IV injury, the broad nature of the tendon requires a robust repair technique that resists gapping without causing excessive shortening, which could limit subsequent PIP flexion.
- Suture Configuration: A core stitch utilizing a modified Bunnell configuration (Kleinert modification) or a modified Kessler stitch is recommended.
- Reinforcement: The core repair should be reinforced with a running or cross-stitch epitenon repair.
- Biomechanical Evidence: According to biomechanical studies by Newport et al., this specific configuration provides a high-tensile-strength repair that resists gap formation and, crucially, does not shorten the broad tendon apparatus.
Postoperative Care
Postoperative management involves continuous extension splinting for 6 to 8 weeks. However, to prevent dense adhesions between the broad tendon and the underlying periosteum of the proximal phalanx, a "short arc" range-of-motion (SAM) rehabilitation program is often initiated early (within the first week), provided the repair is deemed biomechanically secure.
ZONE V EXTENSOR TENDON INJURIES
Zone V includes the extensor mechanism at the level of the metacarpophalangeal (MCP) joint. Injuries here are frequently the result of direct lacerations, crush injuries, or human bites.
Clean Lacerations
For a clean, sharp laceration over the MCP joint, primary repair is indicated. The tendon is repaired using a robust core suture (e.g., 4-0 non-absorbable or slowly absorbable braided suture) reinforced with a cross-stitch or running epitendinous suture. The sagittal bands must also be inspected and repaired if disrupted, to prevent postoperative tendon subluxation.
The "Fight Bite" (Human Tooth Injury)
A critical caveat in Zone V injuries is the high incidence of human bite wounds, classically sustained when a clenched fist strikes a tooth.
Surgical Warning: If a Zone V tendon injury is the result of a tooth strike (fight bite), primary closure and immediate tendon repair are strictly contraindicated due to the extreme risk of polymicrobial septic arthritis and deep space infection (commonly involving Eikenella corrodens, Staphylococcus aureus, and anaerobes).
Management of Bite Injuries:
1. Aggressive surgical debridement and copious irrigation of the MCP joint.
2. The wound is left open to heal by secondary intention or delayed primary closure.
3. Intravenous broad-spectrum antibiotics are administered.
4. Repair of the extensor tendon is delayed until it is definitively clear that there are no septic complications and the infection is fully controlled.
TRAUMATIC DISLOCATION OF THE EXTENSOR TENDON (SAGITTAL BAND RUPTURE)
Traumatic dislocation of the extensor tendon at the MCP joint—often referred to as "Boxer's knuckle"—is a debilitating injury that disrupts the normal tracking of the extensor mechanism. It occurs most commonly in the long (middle) finger.
Mechanism of Injury and Pathoanatomy
The dislocation typically results from a tear in the proximal radial portion of the shroud ligament (sagittal bands) and the more proximal extensor fascia. The classic mechanism involves the finger being suddenly and forcefully extended against resistance, such as in a flicking or thumping motion.
Because the radial sagittal band is most frequently ruptured, the extensor tendon almost universally displaces toward the ulnar aspect of the MCP joint. Ulnar-sided disruption with radial displacement is exceedingly rare. In high-energy or violent mechanisms, the surgeon must also maintain a high index of suspicion for concomitant collateral ligament tears or osteochondral joint surface injuries.
Clinical Presentation and Classification
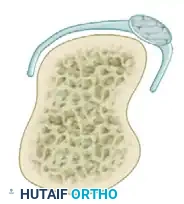
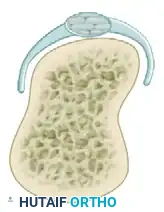
Patients typically present with pain, swelling over the MCP joint, and a snapping sensation upon finger flexion and extension. A pseudodeficit of extension may be observed; the patient cannot actively initiate MCP extension from a fully flexed position because the subluxated tendon lies volar to the joint's axis of rotation. However, if the joint is passively extended, the tendon centralizes, and the patient can maintain extension.
Rayan and Murray described three distinct clinical types of sagittal band injuries, which dictate the treatment algorithm:
Type I: Sagittal Band Strain
Mild injury characterized by contusion or strain of the sagittal band. There is localized pain and swelling, but no extensor tendon instability or subluxation during active range of motion.
Type II: Extensor Tendon Subluxation
Moderate injury involving a partial or complete tear of the sagittal band. The extensor tendon subluxates (usually ulnarly) during MCP flexion but remains partially perched on the metacarpal condyle. It spontaneously centralizes upon extension.
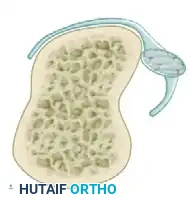
Type III: Extensor Tendon Dislocation
Severe injury with complete disruption of the sagittal band. The extensor tendon completely dislocates into the intermetacarpal gutter during flexion. Active extension is often impossible from a flexed position.
Management Strategies
Acute Injuries (< 3 Weeks)
In nonrheumatoid patients, acute sagittal band injuries (treated within 3 weeks of the initial trauma) generally achieve highly satisfactory results with nonoperative management.
* Protocol: The MCP joint and wrist are splinted in extension for 3 to 4 weeks. This allows the ruptured edges of the sagittal band to approximate and heal.
* Transition: Following the initial immobilization, the patient transitions to 3 to 4 weeks of removable splinting or buddy taping to the adjacent finger on the radial side (to counteract the ulnar displacement vector).
Chronic Injuries and Failed Conservative Management
If the condition goes undetected, becomes chronic (> 3-4 weeks), or fails conservative splinting, operative intervention is required.
* Direct Repair: In some subacute cases, direct primary repair of the radial sagittal band is possible.
* Reconstruction: In chronic cases where the sagittal band tissue is attenuated or retracted, a reconstructive procedure is necessary. A highly successful technique involves utilizing a distally based slip of the central fibers of the extensor tendon itself. This slip is routed deep to the deep transverse metacarpal ligament and sutured back onto itself, creating a robust radial tether that permanently centralizes the extensor mechanism over the MCP joint.
Conclusion
Pathologies of the extensor mechanism—ranging from the insidious progression of a boutonnière deformity to the acute snapping of a sagittal band rupture—demand a profound understanding of hand biomechanics. Whether executing a delicate modified Littler reconstruction, navigating the septic risks of a Zone V bite wound, or centralizing a dislocated tendon, the orthopaedic surgeon must adhere to strict anatomical principles. Meticulous tissue handling, appropriate suture selection, and rigorous postoperative rehabilitation are the cornerstones of restoring optimal digital function.
📚 Medical References
- Extensor mechanism reconstruction with an allograft after total knee arthroplasty, Clin Orthop Relat Res 303:79, 1994.
- Engh GA, Ameen DJ: Periprosthetic fractures adjacent to total knee implants: treatment and clinical results, J Bone Joint Surg 79A:1100, 1997.
- Falahee MH, Matthews LS, Kaufer H: Resection arthroplasty as a salvage procedure for a knee with infection after a total arthroplasty, J Bone Joint Surg 69A:1013, 1987.
- Felix NA, Stuart MJ, Hanssen AD: Periprosthetic fractures of the tibia associated with total knee arthroplasty, Clin Orthop Relat Res 345:113, 1997.
- Firestone TP, Krackow KA, Davis JD, et al: The management of fi xed fl exion contractures during total knee arthroplasty, Clin Orthop Relat Res 284:221, 1992.
- Fujikawa K, Ohtani T, Matsumoto H, et al: Reconstruction of the extensor apparatus of the knee with the Leeds-Keio ligament, J Bone Joint Surg 76B:200, 1993.
- Geerts WH, Pineo GF, Heit JA, et al: Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy, Chest 126(3 suppl):338S, 2004.
- Göksan SB, Freeman MAR: One-stage reimplantation for infected total knee arthroplasty, J Bone Joint Surg 74B:78, 1992.
- Goldberg VM, Figgie HE, Inglis AE, et al: Patellar fracture type and prognosis in condylar total knee arthroplasty, Clin Orthop Relat Res 236:115, 1988.
- Grace JN, Rand JA:
You Might Also Like

