Proximal Interphalangeal Joint Capsulotomy: Surgical Guide
Key Takeaway
Proximal interphalangeal (PIP) joint capsulotomy is a precise surgical intervention indicated for severe, refractory flexion contractures. The Watson technique focuses on the meticulous excision of the checkrein ligaments while preserving the volar plate and critical annular pulleys. This comprehensive guide details the biomechanics, surgical approach, and rigorous postoperative dynamic splinting protocols essential for restoring full passive and active extension in the compromised digit.
INTRODUCTION TO PROXIMAL INTERPHALANGEAL JOINT CAPSULOTOMY
The proximal interphalangeal (PIP) joint is the critical functional hinge of the human digit, responsible for the majority of digital sweep and grip strength. Flexion contractures of the PIP joint are notoriously difficult to manage and represent a formidable challenge in hand surgery. These contractures frequently arise secondary to trauma, prolonged immobilization, volar plate injuries, or as sequelae to conditions such as Dupuytren’s disease.
When conservative measures—including serial casting and dynamic splinting—fail to restore functional extension, surgical intervention becomes necessary. The PIP joint capsulotomy, specifically utilizing the technique popularized by Watson et al., is the gold standard for addressing severe, long-standing flexion deformities. This procedure focuses on the precise identification and resection of the proximal checkrein ligaments, which are the primary pathoanatomic tethers in chronic PIP joint flexion contractures.
This comprehensive academic guide details the biomechanics, indications, step-by-step surgical execution, and rigorous postoperative rehabilitation protocols required to achieve optimal outcomes in PIP joint capsulotomy.
SURGICAL ANATOMY AND BIOMECHANICS
To perform a successful capsulotomy without inducing iatrogenic instability, the surgeon must possess an intimate understanding of the PIP joint's microanatomy.
The Volar Plate and Checkrein Ligaments
The volar plate is a thick, fibrocartilaginous structure that prevents hyperextension of the PIP joint. Distally, it has a firm osseous attachment to the base of the middle phalanx. Proximally, the volar plate becomes membranous and bifurcates into two robust, cord-like structures known as the checkrein ligaments.
These checkreins attach to the periosteum of the proximal phalanx along the volar-lateral margins. In a normal joint, the checkreins unfold and glide during extension. However, following trauma or prolonged flexion, these ligaments undergo fibrotic shortening, effectively tethering the volar plate to the proximal phalanx and preventing the joint from extending.
The Collateral Ligament Complex
The collateral ligaments consist of the proper collateral ligament (PCL), which is taut in flexion, and the accessory collateral ligament (ACL), which is taut in extension and inserts into the volar plate. While the checkreins are the primary restrictors of extension, chronic contractures may also involve secondary shortening of the ACLs.
The Flexor Tendon Sheath
The flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons glide within a highly specialized retinacular sheath. The A2 and A4 pulleys are critical for preventing tendon bowstringing and must be meticulously preserved during any volar approach to the PIP joint. The cruciform pulleys (C1, C2) and the A3 pulley (located directly over the PIP joint) are more expendable and are often resected during capsulotomy to access the underlying joint capsule.
Clinical Pearl: The primary pathology in a PIP joint flexion contracture is almost universally located in the proximal checkrein ligaments. The distal attachment of the volar plate should rarely, if ever, be disturbed, as doing so will result in catastrophic dorsal subluxation or hyperextension instability (swan-neck deformity).
INDICATIONS AND CONTRAINDICATIONS
Indications
- Refractory Flexion Contracture: PIP joint flexion contracture greater than 30 to 40 degrees that has failed a minimum of 3 to 6 months of rigorous conservative therapy (dynamic splinting, serial casting, hand therapy).
- Post-Traumatic Stiffness: Contractures secondary to healed phalangeal fractures, crush injuries, or volar plate avulsions.
- Soft Tissue Contractures: Severe contractures associated with Dupuytren’s diathesis (often performed in conjunction with fasciectomy).
Contraindications
- Intra-articular Incongruity: Severe osteoarthritis, post-traumatic articular step-off, or joint destruction. Capsulotomy relies on a smooth, congruent articular surface to maintain motion. If the joint is destroyed, arthrodesis or arthroplasty is indicated.
- Inadequate Soft Tissue Coverage: Poor volar skin quality that cannot tolerate the tension of extension.
- Non-Compliant Patient: The success of this procedure is entirely dependent on rigorous, prolonged postoperative splinting. Patients unable or unwilling to comply with therapy are poor candidates.
PREOPERATIVE PREPARATION AND POSITIONING
- Anesthesia: The procedure is typically performed under regional anesthesia (axillary or supraclavicular brachial plexus block) or general anesthesia. A purely local digital block is generally insufficient due to the need for tourniquet hemostasis and extensive dissection.
- Positioning: The patient is positioned supine with the operative arm extended on a radiolucent hand table.
- Tourniquet: A pneumatic upper arm tourniquet is applied and inflated to 250 mm Hg (or 100 mm Hg above systolic pressure) after exsanguination with an Esmarch bandage. A bloodless field is absolutely critical for identifying the microvascular structures and the checkrein ligaments.
- Magnification: Surgical loupes (minimum 2.5x to 3.5x magnification) are mandatory for safe dissection around the digital neurovascular bundles and the vincular blood supply.
SURGICAL TECHNIQUE: STEP-BY-STEP (WATSON ET AL.)
1. Incision and Surgical Approach
The volar aspect of the PIP joint can be approached through either a midlateral or a volar zigzag (Brunner) incision.
- Volar Brunner Incision: This is the preferred approach for most surgeons as it provides extensile, bilateral exposure of the flexor sheath and both neurovascular bundles. If the flexion deformity is severe and of long standing, the volar skin itself will be contracted. In such cases, a longitudinal incision converted to a multiple Z-plasty is highly recommended to recruit skin length and prevent wound dehiscence upon joint extension.
- Midlateral Incision: Placed along the neutral axis of the digit (connecting the apices of the flexion creases). If a midlateral incision is selected, a second counter-incision on the opposite side of the joint is frequently required to safely access and release the contralateral checkrein ligament.
2. Superficial Dissection and Neurovascular Protection
Carefully dissect through the subcutaneous tissue.
* Identify and preserve the cutaneous sensory nerve branches.
* Divide Cleland’s and Grayson’s ligaments as necessary to mobilize the digital neurovascular bundles.
* Retract the neurovascular bundles laterally using blunt retractors or vessel loops to protect them throughout the procedure.
3. Flexor Sheath Management
Isolate the flexor tendon sheath. To access the volar plate, portions of the retinacular sheath must be opened.
* Identify the A2 pulley proximally and the A4 pulley distally. These must be preserved at all costs.
* Resect the C1, A3, and C2 pulleys (the portions of the sheath directly overlying the PIP joint and the proximal aspect of the middle phalanx).
* Retract the FDS and FDP tendons laterally. If the tendons are adherent, a meticulous tenolysis must be performed before proceeding to the joint capsule.
4. Identification of the Volar Plate and Checkrein Ligaments
With the flexor tendons retracted, the volar plate comes into view.
* Using loupe magnification, identify the delicate vincular vessels supplying the flexor tendons. These vessels often traverse near the proximal edge of the volar plate. Retract them gently to avoid devascularizing the tendons.
* Identify the proximal membranous edge of the volar plate.
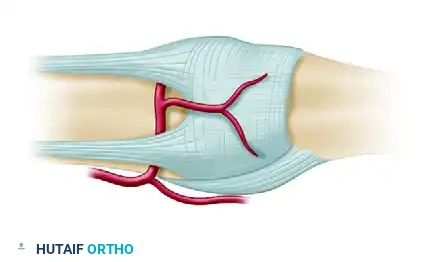
* Bluntly dissect the proximal attachments to reveal the thick, fibrotic checkrein ligaments tethering the volar plate to the proximal phalanx.
Figure A: Anatomy of the volar plate and the proximal checkrein ligaments tethering the joint in flexion. Note the critical vincular blood supply that must be protected during dissection.
5. Excision of the Checkrein Ligaments
This is the most critical step of the Watson technique. The release must be complete, but the volar plate itself must not be detached from the middle phalanx.
- Isolate the checkrein ligament on one side.
- Using a #15 blade or fine tenotomy scissors, sharply divide the checkrein from its attachment on the proximal phalanx.
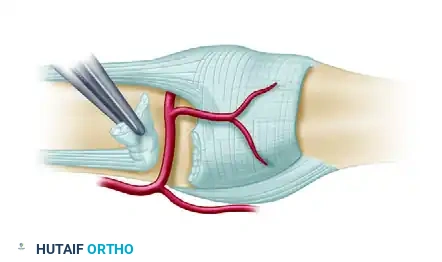
Figure B: Sharp division of the checkrein ligament from the volar plate and proximal phalanx.
- Repeat the process on the contralateral side.
- Once divided, sharply excise the fibrotic segments of the checkrein ligaments entirely to prevent recurrence.
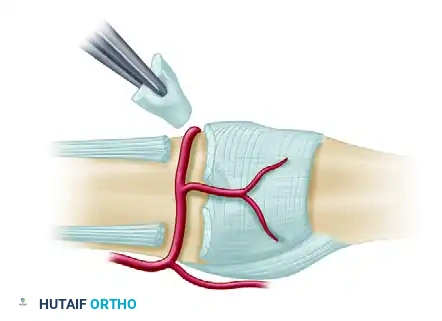
Figure C: Complete excision of the checkrein ligaments on both sides, freeing the proximal aspect of the volar plate.
Surgical Warning: Extreme caution must be exercised to avoid cutting transversely across the main body of the volar plate. Iatrogenic transection of the volar plate will lead to dorsal subluxation of the PIP joint.
6. Joint Mobilization and Adhesion Disruption
Once the checkreins are excised, the primary tether is removed.
* Apply a moderate amount of passive pressure to extend the joint fully.
* You may feel a sudden "give" as intraarticular adhesions and contracted capsular tissues disrupt.
* If full extension is still not achieved, assess the accessory collateral ligaments. If they are severely contracted, a limited, controlled release of the volar-most fibers of the accessory collateral ligaments may be required.
7. Assessment of Extension and Fixation
Evaluate the quality of the extension.
* If the joint extends fully and rests comfortably in extension, no internal fixation is required.
* The "Springy" Joint: If the deformity tends to recur immediately in a “springy” or elastic fashion (often due to residual volar skin shortage or profound flexor muscle-tendon unit shortening), fix the joint in maximum extension using a single transarticular Kirschner wire (0.045-inch). The K-wire is driven obliquely across the PIP joint.
Pitfall: Do not force the joint into extension and pin it if the pressure required is excessive. Forcing a severely contracted joint into pinned extension places immense compressive forces on the articular cartilage, leading to ischemic chondrocyte necrosis and subsequent joint destruction. If excessive pressure is required, accept a slight residual flexion deformity intraoperatively and rely on postoperative dynamic splinting to achieve final extension.
8. Hemostasis and Closure
- Deflate the tourniquet prior to closure.
- Obtain meticulous hemostasis using bipolar electrocautery. Hematoma formation is a primary catalyst for postoperative fibrosis and recurrent stiffness.
- Close the skin with non-absorbable sutures (e.g., 5-0 nylon). If a Z-plasty was designed, transpose the flaps to lengthen the volar skin.
- Apply a non-adherent dressing.
9. Splinting
Apply a bulky, compressive dressing and a plaster splint. The hand should be immobilized in the "intrinsic-plus" or safe position, modified for this specific procedure:
* Wrist in 20 to 30 degrees of extension.
* Metacarpophalangeal (MCP) joints in 70 to 90 degrees of flexion.
* Interphalangeal (PIP and DIP) joints in full extension.
POSTOPERATIVE CARE AND REHABILITATION
The surgical release is only the first half of the treatment; rigorous postoperative rehabilitation is the second, equally critical half. Without strict adherence to splinting protocols, the contracture will inevitably recur.
Phase I: Immediate Postoperative (Days 3 to 7)
- The hand remains immobilized in the initial bulky dressing and splint to allow for reduction of edema and initial wound healing.
- Elevation is strictly enforced to minimize swelling.
Phase II: Early Mobilization (Days 7 to 14)
- The bulky dressing is removed between 3 to 7 days postoperatively.
- A light dressing is applied, and active joint movement is initiated under the supervision of a certified hand therapist.
- Dynamic Splinting Initiation: Dynamic extension splints (e.g., Capener splint or a custom thermoplastic outrigger) are introduced.
- The patient wears the dynamic splint for at least 1 hour of maximal tolerable tension while awake. Tension is reduced throughout the night if tolerated, or a static resting splint in maximum extension is used overnight.
Phase III: Suture Removal and Aggressive Splinting (Weeks 2 to 16)
- Sutures are removed at 12 to 14 days.
- If a transarticular K-wire was utilized, it is typically removed at 2 to 3 weeks in the clinic, followed immediately by dynamic splinting.
- The Watson Protocol: Watson et al. recommended a screw-tension three-point splint. The tension is increased every 3 to 5 minutes for 1 hour before the patient retires for the night, and then the splint is left in place overnight at a tolerable tension.
Clinical Warning: Extreme care must be taken when using screw-tension or three-point dynamic splints. The dorsal skin overlying the PIP joint is exceptionally thin. Excessive pressure can rapidly cause skin ischemia, leading to full-thickness pressure necrosis and exposure of the extensor tendon. Patients must be educated to monitor for severe pain or skin blanching.
- Duration: Night splinting in full extension is continued until full active and passive extension is maintained without regression during the day. Dynamic splinting may be required for up to 4 months postoperatively.
- Serial Casting: At times, if the patient struggles with dynamic splint compliance or if the contracture begins to recur, palmar and dorsal plaster splints (or serial digital casts) may be necessary for 2 to 3 days at a time to force the joint back into full extension through the principle of stress relaxation and tissue creep.
COMPLICATIONS
- Recurrence of Contracture: The most common complication, almost exclusively due to inadequate postoperative splinting or failure to excise the checkreins completely.
- Dorsal Skin Necrosis: Caused by excessive pressure from dynamic extension splints. Requires immediate cessation of splinting and local wound care.
- Digital Ischemia: Forcing a chronic, severe contracture (>60 degrees) into full extension acutely can stretch the digital arteries to the point of vasospasm or occlusion. If the digit becomes white and pulseless upon extension, the joint must be allowed to flex until perfusion returns, and the remaining extension must be gained gradually through postoperative splinting.
- Joint Instability: Iatrogenic transection of the volar plate or excessive release of the collateral ligaments can lead to dorsal subluxation or a swan-neck deformity.
- Infection: Rare, but catastrophic if it involves the flexor tendon sheath or the joint space.
CONCLUSION
Proximal interphalangeal joint capsulotomy via the Watson checkrein excision technique is a highly effective, albeit technically demanding, procedure for resolving refractory flexion contractures. Success relies heavily on a meticulous surgical approach that protects the neurovascular bundles and annular pulleys while completely resecting the fibrotic checkrein ligaments. Furthermore, the surgeon must set clear preoperative expectations with the patient regarding the absolute necessity of a prolonged, rigorous postoperative dynamic splinting regimen to secure a functional, long-lasting result.
You Might Also Like
