
Introduction & Epidemiology
Proximal humerus fractures (PHFs) represent a significant portion of all fractures, accounting for approximately 5-6% of all skeletal injuries and up to 26% of all humeral fractures. Their incidence is biphasic, with a peak in younger, active individuals involved in high-energy trauma, and a much larger, growing peak in the elderly population due to low-energy falls associated with osteoporosis. The increasing life expectancy and prevalence of osteoporosis are driving a substantial rise in PHF incidence, posing a considerable socioeconomic burden due to associated morbidity, functional limitations, and healthcare costs.
Management strategies for PHFs are diverse, ranging from non-operative immobilization to various surgical interventions, including open reduction and internal fixation (ORIF) with plates, intramedullary nailing (IMN), hemiarthroplasty, and reverse total shoulder arthroplasty (rTSA). The selection of the most appropriate treatment modality is predicated on a thorough understanding of fracture morphology, patient demographics, functional demands, bone quality, and associated soft tissue injuries. The AO/OTA classification system, a robust and comprehensive tool, provides a standardized framework for describing these fractures, guiding clinical decision-making, and facilitating research. While historical classifications such as Neer's classification remain conceptually relevant, the AO/OTA system offers a more detailed and biomechanically oriented categorization crucial for surgical planning.
Surgical Anatomy & Biomechanics
A profound understanding of the complex anatomy and biomechanics of the proximal humerus is paramount for successful management of PHFs.
Anatomical Considerations
The proximal humerus comprises the humeral head, anatomical neck, surgical neck, greater tuberosity, lesser tuberosity, and the bicipital groove.
*
Humeral Head:
Articulates with the glenoid fossa. Its vascularity is critical, primarily derived from the ascending branch of the anterior humeral circumflex artery (AHCA) and the posterior humeral circumflex artery (PHCA). The arcuate artery, a branch of the AHCA, typically penetrates the superior-lateral aspect of the head, supplying a significant portion of the epiphysis. Disruption of this blood supply, particularly in multi-fragmentary fractures involving the anatomical neck and tuberosities, predisposes to avascular necrosis (AVN).
*
Anatomical Neck:
The region defining the articular margin of the humeral head. Fractures at this level often imply significant intra-articular involvement and high AVN risk.
*
Surgical Neck:
The narrowest part of the humerus, distal to the tuberosities and anatomical neck. It is a common site for fractures due to its relative weakness.
*
Tuberosities:
*
Greater Tuberosity:
Site of insertion for the supraspinatus, infraspinatus, and teres minor tendons (rotator cuff). Fractures here are frequently avulsion injuries from rotator cuff pull, leading to superior and posterior displacement.
*
Lesser Tuberosity:
Insertion site for the subscapularis tendon. Fractures here result in medial and inferior displacement due to subscapularis pull.
*
Neurovascular Structures:
*
Axillary Nerve:
The most commonly injured nerve in PHFs, running around the surgical neck, approximately 5-7 cm distal to the acromial edge. It innervates the deltoid and teres minor. Injury can result in deltoid paresis/paralysis and sensory loss over the lateral shoulder.
*
Radial Nerve:
Located more distally in the spiral groove, typically not at direct risk in proximal humerus fractures unless there is a significant shaft extension.
*
Musculocutaneous Nerve:
Located anterior to the shoulder joint, innervates the biceps and brachialis.
*
Brachial Plexus:
Can be injured in severe trauma or fracture-dislocations.
*
Axillary Artery and Vein:
Positioned medially and inferiorly to the humeral head, susceptible to injury in severely displaced fractures or fracture-dislocations.
Biomechanical Principles
The proximal humerus is subjected to significant deforming forces from the surrounding musculature, which dictate fracture fragment displacement.
*
Rotator Cuff:
*
Supraspinatus:
Tends to pull the greater tuberosity fragment superiorly and externally.
*
Infraspinatus & Teres Minor:
Exert external rotation and posterior displacement on the greater tuberosity fragment.
*
Subscapularis:
Causes internal rotation and medial displacement of the lesser tuberosity fragment.
*
Deltoid:
Contributes to varus deformity and proximal displacement of the humeral shaft relative to the head fragment.
*
Pectoralis Major & Latissimus Dorsi:
These powerful adductors can cause medial displacement of the humeral shaft.
*
Fracture Stability:
*
Impaction:
Varus or valgus impaction can provide inherent stability, often amenable to non-operative management if alignment is acceptable. Valgus impacted fractures, in particular, tend to be stable and less prone to AVN.
*
Medial Calcar:
The integrity of the medial calcar region is a critical determinant of construct stability in ORIF with plates. Loss of medial support significantly increases the risk of varus collapse, screw cutout, and nonunion.
Proximal Humerus Fracture: AO/OTA Classification
The AO/OTA classification provides a comprehensive system for categorizing proximal humerus fractures based on their anatomical location, articular involvement, and stability. This system, originally developed by Müller et al. in 1988, is widely used for surgical decision-making and prognostic assessment. It categorizes fractures into three main groups (A, B, C), with further subdivisions based on complexity.
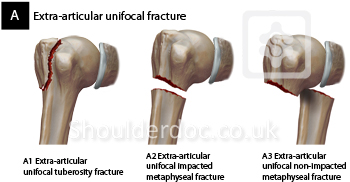
A: Extra-articular unifocal fracture
These fractures do not involve the articular surface and affect only one main segment (tuberosity or surgical neck). They are generally associated with a lower risk of humeral head avascular necrosis compared to articular fractures.
A1 Extra-articular unifocal tuberosity fracture
Fractures involving either the greater or lesser tuberosity, without involvement of the surgical or anatomical neck.
*
.1 Gr Tuberosity, not displaced:
A stable fracture where the greater tuberosity fragment is minimally displaced from its anatomical position. Often managed non-operatively.
*
.2 Gr Tuberosity, displaced:
The greater tuberosity fragment is significantly displaced (>5mm translation, >45 degrees angulation, or subacromial impingement potential). Often warrants surgical fixation due to rotator cuff dysfunction and impingement.
*
.3 Associated with GH dislocation:
A tuberosity fracture occurring concurrently with a glenohumeral joint dislocation. The dislocation must be reduced, and the tuberosity fragment addressed.
A2 Extra-articular unifocal impacted metaphyseal fracture
These involve the surgical neck region where the fragments are impacted, suggesting a degree of inherent stability.
*
.1 No frontal displacement:
A stable, impacted surgical neck fracture with minimal angulation or translation.
*
.2 Varus malalignment:
Impacted surgical neck fracture with a varus deformity of the humeral head relative to the shaft. While impacted, significant varus may impair function and warrant intervention.
*
.3 Valgus malalignment:
Impacted surgical neck fracture with a valgus deformity. Valgus impacted fractures are generally more stable and often have a favorable prognosis regarding AVN.
A3 Extra-articular unifocal non-impacted metaphyseal fracture
These are unstable surgical neck fractures where the fragments are not impacted. They are at higher risk of displacement and typically require surgical stabilization.
*
.1 Simple, angulated:
A two-part surgical neck fracture with significant angulation but minimal translation.
*
.2 Simple, translated:
A two-part surgical neck fracture with significant translation of the fragments.
*
.3 Multifragmentary:
A comminuted surgical neck fracture with multiple fragments.
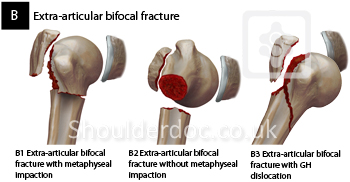
B: Extra-articular bifocal fracture
These fractures involve two distinct regions, typically the surgical neck and one of the tuberosities, but do not involve the articular surface. They represent more complex fracture patterns compared to unifocal types and are often unstable.
B1 Extra-articular bifocal fracture with metaphyseal impaction
Involves two segments, with impaction at the surgical neck providing some stability.
*
.1 Lateral and Gr tuberosity:
Surgical neck fracture with an impacted metaphyseal segment and an associated greater tuberosity fracture.
*
.2 Medial and lesser tuberosity:
Surgical neck fracture with an impacted metaphyseal segment and an associated lesser tuberosity fracture.
*
.3 Posterior and Gr tuberosity:
A less common pattern, often associated with posterior dislocation, involving the posterior aspect of the surgical neck and greater tuberosity.
B2 Extra-articular bifocal fracture without metaphyseal impaction
These are unstable two-segment fractures (surgical neck + tuberosity) without impaction.
*
.1 Without rotational displacement:
Surgical neck fracture and a tuberosity fracture, with minimal rotational deformity.
*
.2 With rotational displacement:
Surgical neck fracture and a tuberosity fracture, with significant rotational displacement of the fragments, often due to muscle pull.
*
.3 Multifragmentary metaphyseal with one of the tuberosities involved:
A comminuted surgical neck fracture combined with a fracture of either the greater or lesser tuberosity.
B3 Extra-articular bifocal fracture with GH dislocation
These are fracture-dislocations where a surgical neck fracture (and often a tuberosity fracture) is combined with a glenohumeral dislocation.
*
.1 Vertical cervical line, Gr Tuberosity intact, Ant-med:
This implies an anterior-medial dislocation (subcoracoid) with a vertically oriented fracture line through the surgical neck, and an intact greater tuberosity.
*
.2 Anterior dislocation with surgical neck fracture:
A classic anterior fracture-dislocation, requiring reduction of the dislocation followed by fixation of the surgical neck.
*
.3 Posterior dislocation with surgical neck fracture:
A posterior fracture-dislocation, often missed, requiring careful assessment and reduction.
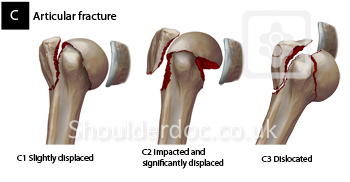
C: Articular fractures
These fractures involve the articular surface of the humeral head, often extending through the anatomical neck. They carry the highest risk of humeral head avascular necrosis and typically present the greatest challenge for anatomical reduction and stable fixation, especially in older, osteoporotic patients.
C1 Articular unifocal fracture (Anatomical Neck)
A fracture involving only the anatomical neck, separating the humeral head from the tuberosities and shaft.
*
.1 Valgus impacted:
An impacted fracture of the anatomical neck in a valgus alignment. While impacted, the articular involvement warrants careful consideration.
*
.2 Varus impacted:
An impacted fracture of the anatomical neck in a varus alignment. More concerning for stability and potential for collapse.
*
.3 Displaced, multifragmentary:
An unstable, often comminuted, anatomical neck fracture where the head fragment is significantly displaced. High risk of AVN.
C2 Articular bifocal fracture (Anatomical Neck and Surgical Neck)
Involves both the anatomical neck and surgical neck, creating a separate humeral head fragment, a tuberosity-shaft fragment, and sometimes separate tuberosity fragments. These correspond to Neer 3-part or 4-part fractures.
*
.1 Valgus impacted:
An impacted fracture involving both anatomical and surgical necks, with a valgus deformity. Despite impaction, these are complex.
*
.2 Varus impacted:
An impacted fracture involving both anatomical and surgical necks, with a varus deformity. Higher risk of fragment instability and AVN.
*
.3 Displaced, multifragmentary:
An unstable fracture involving both anatomical and surgical necks, often with comminution, leading to multiple displaced fragments. Represents a severely disrupted proximal humerus.
C3 Articular multifocal fracture (Head-splitting / Anatomical Neck with Surgical Neck and Tuberosities)
These are head-splitting fractures where the articular surface itself is fractured into multiple pieces, often combined with anatomical and surgical neck fractures. The most severe form of proximal humerus fracture.
*
.1 Valgus impacted:
Head-splitting fracture with some degree of valgus impaction.
*
.2 Varus impacted:
Head-splitting fracture with varus impaction.
*
.3 Displaced, multifragmentary:
Severely comminuted head-splitting fracture with significant displacement of multiple articular fragments. Typically unsalvageable for ORIF.
Indications & Contraindications
The decision-making process for PHFs is complex, balancing patient factors, fracture characteristics, and potential risks versus benefits of operative intervention. The AO/OTA classification is instrumental in guiding these choices.
Non-Operative Indications
Non-operative management typically involves immobilization (sling or coaptation brace) followed by structured rehabilitation. It is generally favored for fractures with inherent stability or in patients where surgical risks outweigh potential functional gains.
-
Minimally Displaced Fractures:
- AO A1.1, A2.1: Non-displaced tuberosity fractures or stable, impacted surgical neck fractures with less than 1 cm translation and less than 45 degrees angulation.
- Neer 1-part fractures: Any fracture with less than 1 cm displacement and less than 45 degrees angulation.
-
Stable Impacted Fractures:
- Valgus impacted surgical neck fractures (e.g., AO A2.3, A2.1). These fractures often have good vascularity and inherent stability.
-
Low-Demand Patients:
- Elderly or frail patients with significant medical comorbidities (e.g., ASA III/IV) where the risks of anesthesia and surgery are high, and their functional demands are limited.
-
Poor Bone Quality:
- Severe osteoporosis where hardware fixation is unlikely to achieve stable purchase, increasing the risk of cutout or failure.
Operative Indications
Surgical intervention aims to restore anatomical alignment, provide stable fixation, and facilitate early rehabilitation to optimize long-term functional outcomes.
-
Displaced Fractures:
- Significant displacement: >1 cm translation or >45 degrees angulation (e.g., AO A2.2, A3, B types).
- Tuberosity displacement: Greater tuberosity displaced >5 mm (risk of impingement and rotator cuff dysfunction) (AO A1.2). Lesser tuberosity displaced >1 cm (significant subscapularis dysfunction).
-
Specific Fracture Patterns:
- Neer 3-part and 4-part fractures (corresponds to AO B2, B3, C2, C3): Highly unstable fractures with significant displacement and high risk of AVN.
- Head-splitting fractures (AO C3): Articular surface is comminuted and often cannot be reconstructed.
- Fracture-dislocations (AO A1.3, B3): Require reduction of the dislocation and stabilization of the fracture.
- Open fractures: Require urgent debridement and fixation.
-
Neurovascular Compromise:
- Acute neurovascular injury requiring surgical exploration and repair in conjunction with fracture fixation.
-
Failure of Non-Operative Management:
- Progressive displacement or intractable pain during conservative treatment.
-
Young, Active Patients:
- Patients with high functional demands who are likely to benefit from anatomical reduction and stable fixation to regain pre-injury activity levels.
-
Irreducible Dislocations:
- Dislocations that cannot be reduced closed due to interposed soft tissue or fracture fragments.
Contraindications
-
Absolute Contraindications:
- Active systemic or local infection.
- Severe, uncontrolled medical comorbidities that make surgery prohibitive (e.g., unstable angina, recent myocardial infarction, severe pulmonary disease).
-
Relative Contraindications:
- Extremely poor bone quality where stable fixation is unachievable (although arthroplasty options may still be considered).
- Pre-existing neurological deficits or rotator cuff pathology that would significantly limit post-operative function irrespective of fracture healing.
- Severe soft tissue compromise (e.g., open wounds, extensive degloving) that precludes safe surgical approach.
Operative vs. Non-Operative Indications
| Indication Category | Non-Operative Management | Operative Management |
|---|---|---|
| Fracture Displacement | < 1 cm translation, < 45° angulation (AO A1.1, A2.1) | > 1 cm translation or > 45° angulation (AO A2.2, A3, B, C) |
| Tuberosity Involvement | Non-displaced tuberosity fractures (AO A1.1) | Displaced greater tuberosity (>5mm), displaced lesser tuberosity (>1cm) (AO A1.2) |
| Articular Involvement | None, or stable impacted articular component (rare) | Articular fractures (AO C types), head-splitting fractures, fracture-dislocations (AO A1.3, B3) |
| Bone Quality | Severe osteoporosis where fixation would be unstable | Good to moderate bone quality for implant purchase |
| Patient Age/Demand | Elderly, low-demand, significant comorbidities (ASA III/IV) | Young, active, high functional demand, minimal comorbidities (ASA I/II) |
| Associated Injuries | Isolated fracture, no neurovascular compromise | Open fractures, neurovascular injury, irreducible dislocations |
| Treatment Response | Stable fracture, acceptable pain control | Progressive displacement, intractable pain despite conservative care |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is crucial for optimizing outcomes in PHFs, particularly for complex fracture patterns.
Diagnostic Imaging
- Plain Radiographs: Standard trauma series including anteroposterior (AP), scapular Y, and axillary lateral views. These provide initial assessment of fracture pattern, displacement, and articular involvement. True AP views are critical, often requiring a 30-degree external rotation of the arm.
-
Computed Tomography (CT) Scan with 3D Reconstructions:
Indispensable for all but the most simple, non-displaced fractures. CT provides detailed information regarding:
- Fracture comminution, especially involving the surgical neck and tuberosities.
- Articular involvement, including head-splitting fragments (AO C3) and glenoid congruity in fracture-dislocations.
- Assessment of medial calcar integrity.
- Accurate measurement of fragment displacement and angulation.
- 3D reconstructions are particularly helpful for visualizing complex multi-fragmentary fractures and planning reduction strategies.
- Magnetic Resonance Imaging (MRI): Less commonly used in the acute setting for fracture assessment itself, but may be indicated if there is suspicion of significant rotator cuff tear (especially in displaced greater tuberosity fractures) or extensive labral injury in fracture-dislocations.
Implant Selection
The choice of implant depends on fracture type (AO classification), bone quality, patient age, and surgeon preference.
-
Plate Osteosynthesis (ORIF):
- Indications: Most common for displaced surgical neck fractures (AO A2, A3), bifocal fractures (AO B types), and some articular fractures (AO C1, C2) where the head can be anatomically reduced and fixed. Best suited for good quality bone.
- Implants: Modern locking plates (e.g., PHILOS plate, Stryker VariAx plate) are standard. These plates provide angular stability, which is crucial in osteoporotic bone, reducing the risk of screw cutout. Key features include multiple diverging screws into the humeral head and dedicated screws for medial calcar support.
-
Intramedullary Nailing (IMN):
- Indications: Primarily for stable or unstable two-part surgical neck fractures (AO A2, A3) with good diaphyseal bone quality. Less ideal for comminuted metaphysis or significant tuberosity involvement due to poor control of head fragment.
- Advantages: Minimally invasive, preserves periosteal blood supply.
-
Hemiarthroplasty:
- Indications: Unsalvageable humeral head due to severe comminution (AO C2.3, C3.3), high risk of AVN (e.g., displaced 4-part fractures in elderly), or severe head impaction/splitting in osteoporotic bone. Typically for older patients with moderate activity levels.
- Considerations: Success heavily relies on stable tuberosity reconstruction for rotator cuff function.
-
Reverse Total Shoulder Arthroplasty (rTSA):
- Indications: Increasing use in acute fracture settings, particularly for elderly patients (typically >70-75 years old) with severely comminuted fractures (AO C2.3, C3.3) where tuberosity repair is compromised, or with pre-existing rotator cuff deficiency. Offers more predictable pain relief and functional outcomes than hemiarthroplasty in this specific population.
-
K-wires / Tension Band Wiring:
- Indications: Primarily for isolated, displaced tuberosity fractures (AO A1.2) or as adjuncts for provisional reduction in complex fractures.
Patient Positioning
-
Beach Chair Position (Most Common):
- Setup: Patient is placed in a semi-recumbent position (30-60 degrees of trunk elevation). The head is supported, and care is taken to avoid brachial plexus traction. The operative arm is draped free to allow full range of motion.
- Advantages: Excellent visualization of the anterior and superior aspects of the shoulder. Allows easy access for fluoroscopy in multiple planes (AP, lateral, axillary). Facilitates reduction maneuvers by leveraging gravity.
- Disadvantages: Potential for hypotension due to pooling of blood in lower extremities ("beach chair hypotension"), requiring meticulous anesthetic management. Careful padding to prevent pressure sores or nerve palsies (e.g., ulnar nerve).
-
Lateral Decubitus Position:
- Setup: Patient lies on their unaffected side, secured with axillary roll and hip/torso supports. The operative arm is suspended in traction.
- Advantages: Excellent for arthroscopic procedures. Can provide good access for certain open approaches if the arm is appropriately positioned. May be preferred in polytrauma patients.
- Disadvantages: More challenging for open fracture fixation (especially plate osteosynthesis) due to limited access to the anterior aspect and difficulty with fluoroscopy in certain planes.
-
Fluoroscopy Setup: Essential for all operative cases. The C-arm must be positioned to allow unobstructed AP, lateral (scapular Y or true lateral), and axillary views without repositioning the patient or C-arm during critical steps. This often requires the C-arm to approach from the opposite side of the patient.
Detailed Surgical Approach / Technique
The choice of surgical approach and technique depends heavily on the specific AO fracture type, surgeon familiarity, and desired outcome. The deltopectoral approach is the workhorse for most open procedures involving the proximal humerus.
Deltopectoral Approach (Standard for ORIF, Hemiarthroplasty, rTSA)
This approach utilizes the internervous plane between the deltoid and pectoralis major muscles.
- Incision: A curvilinear incision is made from the coracoid process, extending distally along the anterior border of the deltoid, typically 8-10 cm. The incision can be extended proximally toward the acromion or distally as needed.
- Superficial Dissection: The superficial fascia is incised, exposing the deltoid and pectoralis major muscles. The cephalic vein, lying in the deltopectoral groove, is identified. While often preserved, it may be ligated if its retraction impedes exposure. Its preservation is generally preferred to reduce postoperative swelling.
- Internervous Plane: The deltoid (innervated by the axillary nerve, C5-C6) is retracted laterally, and the pectoralis major (innervated by medial and lateral pectoral nerves, C5-T1) is retracted medially. This provides safe access to the anterior shoulder without violating major neurovascular structures or muscle fibers.
- Deep Dissection: The clavipectoral fascia, deep to the deltopectoral groove, is incised. This exposes the conjoint tendon (short head of biceps and coracobrachialis) medially, which is retracted with the pectoralis major. The underlying subscapularis muscle and the anterior capsule are identified.
- Identification of Axillary Nerve: The axillary nerve typically runs 5-7 cm distal to the lateral acromial edge. In the deltopectoral approach, it is generally protected posteriorly. However, care must be taken during retraction and drilling, especially for more distal screw placement.
- Rotator Interval: For improved visualization of the humeral head and glenoid, the rotator interval (between supraspinatus and subscapularis) can be opened. This allows access to the articular surface for direct visualization and reduction. The ascending branch of the anterior humeral circumflex artery, critical for humeral head vascularity, typically runs here and should be carefully protected.
Fracture Reduction Techniques
Achieving anatomical reduction is paramount for restoring shoulder function and stability.
- Indirect Reduction (Ligamentotaxis): Gentle axial traction and external rotation can often achieve initial alignment, particularly for Neer 2-part surgical neck fractures (AO A2, A3).
-
Direct Reduction:
- Joy-sticks / K-wires: Large K-wires inserted into the head and shaft fragments act as joysticks to manipulate and align the fragments.
- Blunt Hohmann Retractors: Can be used to lever fragments into position.
- Suture Traction: Heavy non-absorbable sutures can be passed through the rotator cuff tendons attached to the tuberosity fragments to facilitate traction and rotation.
- Ball-spiked Pushers / Bone Hooks: Used to apply direct pressure to reduce displaced fragments.
- Temporary Fixation: Once reduced, fragments are provisionally stabilized with K-wires. This allows for assessment of reduction quality under fluoroscopy and preparation for definitive fixation.
Definitive Fixation
Plate Osteosynthesis (ORIF)
- Preparation: The fracture hematoma is gently debrided, and any interposed soft tissue is removed. The fracture fragments are meticulously reduced, restoring anatomical alignment and glenohumeral congruity.
- Plate Placement: A precontoured locking plate (e.g., PHILOS, VariAx) is positioned laterally on the proximal humerus. The superior edge of the plate is typically placed 5-8 mm distal to the superior border of the greater tuberosity to avoid subacromial impingement. The plate should be centered on the lateral shaft.
- Shaft Fixation: The plate is first secured to the humeral shaft with cortical screws. This provides a stable base.
- Head Fixation: Multiple locking screws are inserted into the humeral head. The goal is to obtain divergent screw trajectories to capture maximum bone stock and achieve subchondral support. At least 3-4 locking screws should engage the humeral head.
-
Medial Column Support:
Crucial for preventing varus collapse, especially in osteoporotic bone. Techniques include:
- Medial Calcar Screws: Specially designed locking screws in many plate systems that provide direct medial support.
- Cancellous Bone Graft: Autologous or allograft bone can be impacted into the medial metaphyseal defect to provide structural support.
- Suture Support: Heavy sutures can be passed around the medial calcar and through the plate to provide additional tensioning.
- Tuberosity Repair: If tuberosity fragments are separate, non-absorbable sutures are passed through the rotator cuff tendons (supraspinatus, infraspinatus, subscapularis) and tied down through holes in the plate or around the shaft, compressing the tuberosities to the humeral head and shaft. This is critical for restoring rotator cuff function and reducing AVN risk by decompressing vessels.
- Final Assessment: The reduction and fixation stability are assessed under fluoroscopy in multiple planes and through intraoperative range of motion.
Intramedullary Nailing (IMN)
- Approach: Often a deltoid-splitting (anterolateral) approach or a supralateral approach directly over the greater tuberosity is used to establish the entry portal.
- Entry Portal: A small incision is made, and the deltoid fibers are split. The entry portal is created at the tip of the greater tuberosity or slightly medial, avoiding disruption of the supraspinatus insertion.
- Nail Insertion: A guide wire is passed down the medullary canal. The canal may be reamed. The intramedullary nail is then inserted.
- Locking Screws: Proximal locking screws are inserted to engage the humeral head, often with multiple divergent screws. Distal locking screws secure the nail to the shaft.
- Limitations: Less suitable for significantly comminuted head fractures or severely displaced tuberosity fractures that require direct reduction. Difficult to control rotation of head fragments.
Hemiarthroplasty (HA)
- Indications: Performed for unsalvageable head fractures (e.g., AO C2.3, C3.3) in older, less active patients.
-
Technique (Deltopectoral Approach):
- The humeral head fragment is excised.
- The medullary canal is prepared for the prosthetic stem.
- A trial component is inserted to determine appropriate head size and version.
- The definitive stem is implanted (cemented or uncemented).
- The tuberosities are meticulously repaired around the prosthetic neck and to the humeral shaft using strong non-absorbable sutures. This is the most crucial step for functional recovery.
Reverse Total Shoulder Arthroplasty (rTSA)
- Indications: Increasingly used for severely comminuted fractures in elderly patients, especially those with pre-existing rotator cuff dysfunction, or when tuberosity repair is deemed unlikely to succeed.
-
Technique (Deltopectoral Approach):
- Similar to hemiarthroplasty, the humeral head is excised.
- The glenoid is prepared, and a baseplate is fixed to the glenoid, followed by the glenosphere.
- The humeral shaft is prepared, and the humeral stem and polyethylene liner are inserted.
- Tuberosity repair, while less critical than in hemiarthroplasty for deltoid function, is still important for external rotation and overall stability.
Anterolateral / Delta-split Approach
- Indications: Primarily for isolated greater tuberosity fractures (AO A1), or as an entry point for IMN.
- Technique: A longitudinal incision is made over the lateral aspect of the deltoid. The deltoid muscle fibers are split bluntly in line with their fibers.
- Axillary Nerve Protection: The axillary nerve typically crosses the deltoid muscle horizontally approximately 5-7 cm distal to the acromion. The deltoid split should not extend beyond this point to avoid nerve injury.
Complications & Management
Proximal humerus fractures and their treatment are associated with a range of potential complications, which can significantly impact functional outcomes. Proactive identification and appropriate management are essential.
| Complication | Incidence (Approximate) | Salvage Strategies / Management |
|---|---|---|
| Avascular Necrosis (AVN) of Humeral Head | 10-30% (after ORIF for 3/4-part), higher in AO C types | Early: Observation for asymptomatic cases. Late (with collapse/symptoms): Hemiarthroplasty, Reverse Total Shoulder Arthroplasty (rTSA) for older patients with cuff deficiency or poor tuberosity repair. |
| Nonunion / Malunion | 5-15% | Nonunion: Revision ORIF with bone grafting (autograft/allograft), plate exchange, IMN. If poor bone quality or significant deformity, consider HA or rTSA. Malunion: If symptomatic (impingement, limited ROM, pain): osteotomy (less common), HA, rTSA (especially for varus malunion). |
| Hardware Failure (e.g., Screw Cutout, Plate Bending) | 5-20% | Early: Revision fixation, often with more robust implants, bone grafting, or switch to arthroplasty (HA/rTSA). Late: If fracture united, hardware removal may suffice. If nonunion, address nonunion as above. |
| Infection | < 5% | Superficial: Oral antibiotics, wound care. Deep (acute): Surgical debridement, extensive irrigation, intravenous antibiotics, may attempt hardware retention if stable. Deep (chronic/failed retention): Hardware removal, repeat debridement, antibiotic cement spacer, delayed reimplantation (rTSA) or excision arthroplasty. |
| Nerve Injury (Axillary Nerve Most Common) | < 5% | Neuropraxia/Axonotmesis: Observation, EMG at 3-6 months. Physical therapy. Neurotmesis (rare): Surgical exploration and repair/grafting. |
| Adhesive Capsulitis (Frozen Shoulder) | 10-20% | Aggressive physical therapy, steroid injections. If refractory: Manipulation Under Anesthesia (MUA) or Arthroscopic Capsular Release. |
| Rotator Cuff Impingement/Failure | Variable | Impingement: Removal of prominent hardware after union, subacromial decompression. Failure/Tear: If amenable to repair, open or arthroscopic rotator cuff repair. If unrepairable, reverse total shoulder arthroplasty (rTSA). |
| Post-traumatic Osteoarthritis | Variable, long-term | Conservative management (NSAIDs, injections, physical therapy). If severe and symptomatic: HA or rTSA. |
Avascular Necrosis (AVN) of the Humeral Head
- Pathophysiology: Disruption of the vascular supply to the humeral head, primarily the ascending branch of the AHCA. Risk is highest in highly comminuted fractures with significant displacement of the head and tuberosity fragments (AO C2, C3, Neer 4-part).
- Incidence: Varies significantly by fracture type and study, ranging from 10% to over 30% after ORIF for complex fractures.
-
Management:
- Asymptomatic AVN: Often observed.
- Symptomatic AVN (head collapse, pain): Requires salvage, typically arthroplasty. Hemiarthroplasty is a traditional option, but rTSA is increasingly favored in the elderly due to more predictable pain relief and functional outcomes, especially if tuberosity healing is compromised.
Nonunion / Malunion
-
Nonunion:
Failure of the fracture to heal after an appropriate period (typically 6-9 months). Often associated with inadequate reduction, unstable fixation, or poor bone biology.
- Management: Revision ORIF with bone grafting (autograft or allograft), plate exchange, or conversion to arthroplasty (HA or rTSA) if bone quality is poor or a successful ORIF is unlikely.
-
Malunion:
Healing of the fracture in an unacceptable anatomical position, leading to impingement, limited range of motion, and pain. Varus malunion is particularly problematic.
- Management: If symptomatic, corrective osteotomy (less common for PHF), or conversion to HA or rTSA.
Hardware Failure
- Screw Cutout: Occurs when screws lose purchase in osteoporotic humeral head bone, leading to loss of reduction, varus collapse, and penetration of the articular surface. Often due to insufficient medial calcar support or inadequate screw placement.
- Plate Bending/Breakage: Less common with modern locking plates, but can occur with inadequate reduction or severe osteopenia.
-
Management:
- Early Failure: Revision surgery often involves more robust fixation, bone grafting, or conversion to arthroplasty.
- Late Failure (after union): Hardware removal may be sufficient if symptoms are related to hardware prominence.
Infection
- Incidence: Relatively low (<5%).
-
Management:
- Acute Superficial: Oral antibiotics and wound care.
- Acute Deep: Surgical debridement, extensive irrigation, intravenous antibiotics. Hardware retention may be attempted if the construct is stable, and the organism is low virulence.
- Chronic/Failed Retention: Hardware removal, repeat debridement, antibiotic-loaded cement spacer, followed by delayed arthroplasty (rTSA) or excision arthroplasty.
Nerve Injury
- Axillary Nerve: Most commonly injured nerve. Can result from direct trauma, excessive traction during reduction, or inadvertent placement of hardware.
-
Management:
- Neuropraxia/Axonotmesis: Often resolves spontaneously. Observation, physical therapy, and electrodiagnostic studies (EMG) at 3-6 months.
- Neurotmesis (Complete Transection): Rare, requires surgical exploration and repair or grafting.
Adhesive Capsulitis (Frozen Shoulder)
- Incidence: High, up to 20% in some series, especially if rehabilitation is delayed or inadequate.
- Management: Aggressive physical therapy. If refractory, manipulation under anesthesia (MUA) or arthroscopic capsular release.
Post-Operative Rehabilitation Protocols
A well-structured and individualized post-operative rehabilitation program is critical for maximizing functional recovery and minimizing complications after PHF surgery. The protocol must be tailored to the patient's age, bone quality, fracture stability, type of fixation, and rotator cuff integrity.
Phase 1: Immobilization & Early Passive Motion (Weeks 0-6)
Goals: Protect the healing fracture/repair, manage pain, prevent stiffness, and initiate early, controlled motion.
-
Immobilization:
- Arm placed in a sling or shoulder immobilizer. Duration varies based on fracture stability and surgeon preference, typically 3-6 weeks.
- For tuberosity repairs, the arm may be positioned in slight abduction/external rotation to reduce tension on the repair.
-
Pain Management:
- Pharmacological (NSAIDs, analgesics), cryotherapy.
-
Pendulum Exercises:
- Initiated early (first few days) to promote joint lubrication and gentle motion, performed with the trunk leaning forward.
-
Passive Range of Motion (PROM):
- Initiated typically at 2-3 weeks, strictly controlled by a therapist.
- Flexion: Limited to 90 degrees in the scapular plane (elevation in plane of scapula).
- External Rotation (ER): Limited to 0-30 degrees (supine), depending on tuberosity repair integrity. If the greater tuberosity was repaired, ER is often restricted.
- Internal Rotation (IR): To tolerance, generally behind the back.
- Avoid: Active motion, lifting, weight-bearing, or sudden movements.
-
Scapular Stabilization Exercises:
- Gentle isometric contractions for scapular musculature.
-
Elbow, Wrist, Hand ROM:
- Active exercises to prevent stiffness in uninvolved joints.
Phase 2: Active-Assisted & Active Motion (Weeks 6-12)
Goals: Gradually increase range of motion, restore muscle activation, and begin light strengthening.
-
Sling Discontinuation:
- As comfort allows, typically by 6 weeks post-op.
-
Active-Assisted Range of Motion (AAROM):
- Progress from passive to active-assisted exercises using a pulley system, wand, or unaffected hand.
- Gradually increase flexion, abduction, and rotation within pain-free limits.
-
Gentle Active Range of Motion (AROM):
- Initiated as bone healing progresses and stability is confirmed (radiographically or clinically).
- Focus on isolated rotator cuff and deltoid activation (e.g., table slides, wall walks).
-
Isometric Strengthening:
- Initiate gentle isometric contractions for rotator cuff and deltoid at various positions, progressing cautiously.
-
Scapular Strengthening:
- Progressive exercises for scapular retractors and stabilizers.
-
Light Strengthening:
- Introduction of very light resistance exercises with elastic bands or light weights for the shoulder and surrounding musculature.
- Avoid: Heavy lifting, pushing, pulling, or sudden, uncontrolled movements.
Phase 3: Progressive Strengthening & Return to Activity (Weeks 12+)
Goals: Achieve full functional range of motion, restore strength and endurance, and facilitate return to pre-injury activities.
-
Aggressive Strengthening:
- Progressive resistive exercises for all major shoulder muscle groups (deltoid, rotator cuff, scapular stabilizers).
- Focus on eccentric control and concentric strength.
- Begin with open-chain exercises, progress to closed-chain.
-
Endurance Training:
- Activities designed to improve muscle endurance.
-
Proprioceptive Training:
- Exercises to improve joint position sense and coordination.
-
Sport-Specific / Work-Specific Training:
- For patients returning to demanding activities, incorporate functional drills that mimic their specific requirements.
-
Gradual Return to Activity:
- Return to activities of daily living (ADLs), work, and sports is gradual, guided by pain levels, strength, and range of motion.
- Full recovery can take 6-12 months, or even longer for complex fractures.
-
Considerations:
- Tuberosity Repairs: Require slower progression of active motion, especially external rotation, to protect the healing tendons.
- Bone Quality: Patients with osteoporosis or severely comminuted fractures require a more conservative and prolonged rehabilitation course.
- Individualization: Protocols must be individualized based on patient response, pain, and tolerance. Close communication between the surgeon and physical therapist is paramount.
Summary of Key Literature / Guidelines
The landscape of proximal humerus fracture management is continuously evolving, driven by ongoing research and clinical experience. Several key areas remain subjects of active investigation and debate.
Current Controversies
-
ORIF vs. Non-Operative Management for Displaced 3- and 4-Part Fractures in the Elderly:
- Historically, displaced 3- and 4-part fractures (AO B2, B3, C2, C3) in the elderly were considered indications for ORIF or hemiarthroplasty.
- The PROFHER trial (Proximal Fracture of the Humerus Evaluation by Randomisation) , a landmark multicenter randomized controlled trial, demonstrated that surgical intervention (ORIF or hemiarthroplasty) offered no significant benefit over non-operative treatment in terms of pain, function, or health-related quality of life at 2 years for the majority of displaced proximal humerus fractures.
- Implication: This challenges traditional indications, suggesting non-operative management may be appropriate for a broader range of displaced fractures in the elderly, particularly when considering patient comorbidities and surgical risks. However, selection bias and the heterogeneity of fracture patterns mean that a subset of patients still clearly benefits from surgery.
-
Hemiarthroplasty vs. Reverse Total Shoulder Arthroplasty (rTSA) for Acute Fractures:
- For unsalvageable head fractures (AO C3) in the elderly, hemiarthroplasty has been the traditional surgical option. However, outcomes have been variable, often limited by the inability to achieve reliable tuberosity healing, leading to poor active elevation and external rotation.
- rTSA has emerged as a superior option in many elderly patients, especially those over 70-75 years old, with severely comminuted fractures, poor bone quality, or pre-existing rotator cuff dysfunction. It provides more predictable pain relief and functional elevation by bypassing a non-functional rotator cuff. Evidence increasingly supports rTSA as the implant of choice for fracture arthroplasty in this demographic.
-
Intramedullary Nailing (IMN) vs. Plate Osteosynthesis (ORIF):
- For two-part surgical neck fractures (AO A2, A3), both IMN and locking plates are viable options.
- IMN offers advantages of less soft tissue disruption and potentially less periosteal stripping, theoretically preserving vascularity. However, it provides less control over comminuted head fragments and tuberosities.
- Locking plates provide robust multi-planar fixation, allowing better control of articular fragments and facilitating tuberosity repair. The choice often depends on fracture morphology, bone quality, and surgeon experience.
-
Importance of Medial Column Support in Locking Plate Fixation:
- Numerous biomechanical and clinical studies emphasize the critical role of restoring and supporting the medial calcar region to prevent varus collapse and screw cutout in locking plate osteosynthesis, especially in osteoporotic bone. Techniques like calcar screws, medial plate application, or bone grafting are advocated.
Key Publications / Guidelines
- Neer, C.S. (1970). Displaced Proximal Humeral Fractures. Part I. Classification and Evaluation. Journal of Bone and Joint Surgery Am , 52:1077-1089. (Classic classification, foundational understanding)
- Müller, M.E., Nazarian, S., Koch, P., Schatzker, R. (1988). The Comprehensive Classification of Fractures of Long Bones. Springer-Verlag, Berlin Heidelberg. (The basis for AO/OTA classification)
- Handoll, H.H.G., Brorson, S. (2015). Interventions for treating proximal humeral fractures in adults. Cochrane Database of Systematic Reviews , Issue 11. Art. No.: CD000434. (Systematic reviews informing treatment decisions)
- Rangan, A., et al. (2015). Surgical versus nonsurgical treatment of adults with displaced proximal humeral fractures: the PROFHER randomised controlled trial. The Lancet , 386(9990):1741-1751. (PROFHER trial - significant impact on non-operative indications)
- Recent American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines: These guidelines provide evidence-based recommendations for the diagnosis and management of proximal humerus fractures, synthesizing current literature to inform clinical practice.
In conclusion, the management of proximal humerus fractures requires a nuanced understanding of anatomical nuances, biomechanical forces, and meticulous application of the AO/OTA classification. While non-operative treatment remains the cornerstone for stable fractures and some complex patterns in selected patients, surgical techniques have advanced considerably, offering diverse solutions for restoring function and improving outcomes in appropriately indicated cases. The ongoing dialogue in the literature continually refines our approach to these challenging injuries.
