Mastering Direct Anterior Approach Hip Arthroplasty Without a Traction Table

Key Takeaway
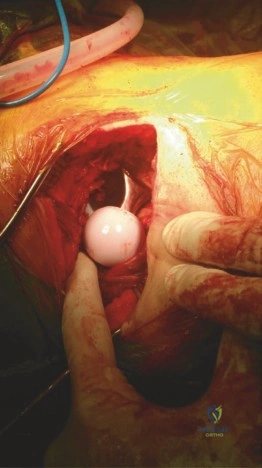
Here are the crucial details you must know about Mastering Direct Anterior Approach Hip Arthroplasty Without a Traction Table. The direct anterior approach for hip arthroplasty involves an incision 45° backward and upward from the greater trochanter. Short rotators and the capsule are tagged, detached for reattachment, and help protect the sciatic nerve. The gluteus medius and minimus muscles are protected, allowing for easy exposure of the acetabular fossa during surgery.
You are performing a primary Total Hip Arthroplasty (THA) via the Direct Anterior Approach (DAA) on a standard, flat operating table. As you attempt to deliver the proximal femur into the wound for broaching, you encounter significant resistance. What is your immediate management strategy, and what specific anatomical structures are you assessing?
Candidate: I would stop forcing the leg, as this risks a femoral fracture. I would check my soft tissue releases, specifically the posterior capsule and the piriformis tendon. I might also need to perform a release of the pubofemoral ligament and potentially use a different retractor or adjust the position of the leg.
Candidates often suggest "pulling harder" or calling for a traction table setup mid-procedure. A failing candidate fails to articulate the sequence of the release and focuses on the retractor rather than the underlying tethering structures, ignoring the biomechanical requirement for external rotation and extension.
A high-scoring answer follows a structured "Stop, Assess, Release" algorithm: 1. Stop: Cease manipulation immediately to prevent iatrogenic calcar fracture. 2. Assessment: Identify the "tethers." This is usually the superior capsule ("saddle" release), the posterior capsule along the intertrochanteric crest, or the pubofemoral ligament. 3. Sequential Release: Systematically release the superior capsule, then the posterior capsule (while protecting the short external rotators), and finally, if needed, the piriformis tendon. 4. Positioning: Confirm adequate extension, adduction, and external rotation of the limb to facilitate anterior delivery of the femur.
During the dissection of the Hueter interval, you encounter a vessel crossing the field transversely. How do you handle this, and what is its clinical significance?
Candidate: This is the ascending branch of the lateral circumflex femoral artery, often called the "leash." I would ligate it or cauterize it to prevent a hematoma.
Failing to name the vessel precisely, or dismissing it as "just a vessel." A poor answer ignores the risk of significant postoperative hematoma if not managed effectively, or suggests blind cautery which risks damaging deeper structures.
Identify this as the ascending branches of the lateral circumflex femoral artery (LCFA). Explain that it must be meticulously isolated and controlled (cautery or ties) because retraction in this area can avulse the vessel, leading to a significant postoperative hematoma, which is a recognized cause of wound complications and delayed recovery in DAA.
You have finished the procedure. A colleague points out that the patient is complaining of numbness and tingling over their lateral thigh. What is the most likely cause, and how could this have been avoided?
Candidate: This is likely an injury to the Lateral Femoral Cutaneous Nerve (LFCN). It happens because of the incision or retraction. I should have made the incision more lateral.
Being vague about the etiology. Failing to mention that the nerve has variable anatomy and that aggressive medial-to-lateral retraction is a major contributor to iatrogenic stretch injury.
The diagnosis is Meralgia Paresthetica caused by injury to the Lateral Femoral Cutaneous Nerve (LFCN). To avoid this, the surgeon should: 1. Incision Placement: Incise the fascia strictly over the Tensor Fasciae Latae (TFL) belly, rather than in the intermuscular groove, as the nerve often branches in the groove. 2. Retraction: Avoid excessive medial-to-lateral retraction force. 3. Awareness: Recognize that anatomical variation is common and the nerve may be superficial or branched.
