Advanced Bilateral Simultaneous THA: Uncemented Monobloc Case Presentation
Patient Presentation & History
A 62-year-old male presented with a 5-year history of progressively worsening bilateral hip pain, more pronounced on the left, severely limiting his activities of daily living. The pain was described as deep, aching, and localized to the groin and buttock, radiating to the anterior thigh. It was exacerbated by weight-bearing activities, prolonged standing, and initiation of movement after rest. Night pain and difficulty sleeping were reported. He ambulated with a significant antalgic gait and required a cane for distances greater than 50 meters. He denied any preceding trauma, inflammatory episodes, or neurological deficits.
Demographics:
* Age: 62 years
* Sex: Male
* Occupation: Retired accountant
* BMI: 28 kg/m²
Comorbidities:
* Controlled hypertension (on lisinopril)
* Type 2 Diabetes Mellitus (HbA1c 6.8%, on metformin)
* Hyperlipidemia (on atorvastatin)
* No history of previous hip surgery, deep vein thrombosis (DVT), pulmonary embolism (PE), or cardiac events.
* ASA physical status classification: II
Etiology of Hip Pathology:
His history and initial workup were consistent with primary osteoarthritis, advanced bilaterally. There was no clear history suggestive of developmental dysplasia of the hip (DDH), Legg-Calve-Perthes disease, or slipped capital femoral epiphysis (SCFE) in childhood, nor significant trauma leading to post-traumatic arthritis. While avascular necrosis (AVN) was considered in the differential, clinical and radiological features did not strongly support it as the primary etiology. The progressive nature of his symptoms, coupled with characteristic radiographic findings, pointed towards idiopathic degenerative arthritis.
Clinical Examination
General Inspection:
The patient appeared comfortable at rest but exhibited an antalgic gait with a shortened stance phase on both lower limbs, more pronounced on the left. A mild Trendelenburg sign was noted on both sides during ambulation. No significant limb length discrepancy was grossly apparent. Mild bilateral quadriceps and gluteal atrophy was observed. No skin changes, scars, or overt deformities around the hips were present.
Palpation:
* Tenderness was elicited over the anterior groin and greater trochanteric regions bilaterally, consistent with capsular irritation and possible trochanteric bursitis.
* No palpable masses, crepitus (grossly), or warmth was noted.
* Peripheral pulses (femoral, popliteal, dorsalis pedis, posterior tibial) were strong and symmetrical bilaterally.
Range of Motion (ROM):
All measurements were taken with the patient supine.
*
Right Hip:
* Flexion: 90° (painful at end range)
* Extension: 0°
* Abduction: 20° (painful)
* Adduction: 10°
* Internal Rotation: 5° (severely painful)
* External Rotation: 15°
* Fixed flexion deformity: 10°
*
Left Hip:
* Flexion: 80° (painful at end range)
* Extension: 0°
* Abduction: 15° (severely painful)
* Adduction: 5°
* Internal Rotation: 0° (excruciatingly painful)
* External Rotation: 10°
* Fixed flexion deformity: 15°
Neurological Assessment:
* Motor strength: 5/5 in all major muscle groups of both lower extremities (hip flexors, extensors, abductors, adductors, knee flexors, extensors, ankle dorsiflexors, plantarflexors). No focal weakness.
* Sensory: Intact light touch and pinprick sensation in L1-S1 dermatomes bilaterally.
* Reflexes: Patellar and Achilles reflexes were 2+ and symmetrical bilaterally. No pathological reflexes.
* Neurovascular status was otherwise unremarkable.
Imaging & Diagnostics
Plain Radiographs:
Standard radiographs including an AP pelvis with both hips, true lateral views of both hips, and a Dunn lateral view were obtained.
-
AP Pelvis (Figure 1):
- Demonstrated severe tricompartmental joint space narrowing bilaterally, with effacement of the superior, medial, and inferior joint spaces.
- Prominent osteophyte formation was evident along the femoral head-neck junction and acetabular rims.
- Subchondral sclerosis and large subchondral cysts were present in the femoral heads and acetabula, more pronounced on the left.
- Loss of the normal spherical contour of both femoral heads.
- Mild acetabular protrusio was noted on both sides, particularly the left, with the femoral head crossing the ilioischial line.
- No evidence of acute fracture, dislocation, or tumor.
- No significant limb length discrepancy observed on the AP pelvis, though clinical assessment suggested minor shortening on the left.
- Pauwel's angle appeared normal.
- Centre-Edge angle (Wiberg) was reduced bilaterally.

Figure 1: Pre-operative AP Pelvis radiograph demonstrating severe bilateral hip osteoarthritis with joint space narrowing, osteophytes, and subchondral changes.
- Lateral Hips: Confirmed the anterior and posterior osteophyte formation and demonstrated the anterior extent of femoral head coverage.
Advanced Imaging (CT/MRI):
*
Computed Tomography (CT) Scan:
A CT scan of the pelvis and hips was performed to assess the three-dimensional morphology of the acetabulum, quantify bone stock, evaluate for potential protrusio or severe acetabular distortion, and assist with precise templating. This was particularly useful in confirming the absence of significant bony deformities that might complicate acetabular reaming or component placement.
*
Magnetic Resonance Imaging (MRI):
An MRI was initially considered to rule out avascular necrosis or significant labral pathology, but given the advanced nature of the radiographic osteoarthritis, it was deemed less critical for surgical planning. It would have provided detailed information on cartilage loss, synovitis, and soft tissue structures, but the decision for THA was already clear based on plain radiographs and clinical presentation.
Templating:
Digital templating was performed meticulously using calibrated radiographs and CT data. This involved:
* Determining optimal acetabular component size and position (inclination and anteversion) to maximize coverage and achieve stability.
* Selecting appropriate femoral stem size and type (cemented vs. uncemented, monobloc vs. modular) to restore leg length, offset, and provide stable fixation.
* Pre-operative planning estimated a 52mm uncemented monobloc acetabular component and a Size 12 uncemented tapered femoral stem for both hips.
* Ceramic-on-polyethylene bearing surfaces were planned due to the patient's age and activity level.
* Consideration for leg length equality was paramount, with careful attention to restoring the native hip center and femoral offset.

Figure 2: Digital templating for femoral component sizing and offset restoration.

Figure 3: Digital templating for acetabular component sizing and placement, ensuring optimal coverage and inclination.
Differential Diagnosis
| Feature | Bilateral Hip Osteoarthritis (Primary) | Bilateral Inflammatory Arthropathy (e.g., RA, AS) | Bilateral Avascular Necrosis (AVN) | Bilateral Femoroacetabular Impingement (FAI) leading to OA |
|---|---|---|---|---|
| Pain Characteristics | Deep, aching groin/buttock pain; insidious onset; worse with activity, relieved by rest; "start-up" pain. | Symmetrical, persistent pain; worse with rest/inactivity (morning stiffness > 30 mins); insidious onset; systemic symptoms (fatigue, fever). | Sudden or insidious onset of pain; often disproportionate to activity level; may precede radiographic changes; can progress rapidly. | Groin pain with specific movements (flexion, adduction, internal rotation); "C" sign; mechanical symptoms (clicking, locking); often in younger, active individuals. |
| Physical Exam | Limited ROM (especially internal rotation); pain on motion; antalgic gait; Trendelenburg sign; fixed deformities common. | Symmetrical polyarthritis; synovitis; extra-articular manifestations (rheumatoid nodules, enthesitis, uveitis); limited ROM due to inflammation/pannus. | Limited ROM, especially internal rotation and abduction; pain with forced motion; antalgic gait. | Limited internal rotation (especially in flexion); positive impingement tests (FADIR); often no significant fixed deformity until late-stage OA. |
| Radiographic Findings | Progressive joint space narrowing (superior, medial); osteophytes; subchondral sclerosis; subchondral cysts; femoral head flattening/deformation. | Symmetrical joint space narrowing; erosions (especially RA); osteopenia/osteoporosis; periarticular swelling; sacroiliitis (AS); ankylosis (AS). | Early: Normal X-rays. Later: Crescent sign (subchondral collapse), flattening of femoral head, joint space preserved until collapse, reactive sclerosis. | Cam/Pincer lesions (e.g., pistol grip deformity of femoral head/neck junction, acetabular retroversion); chondrolabral damage; eventually secondary OA changes. |
| Laboratory Markers | Usually normal ESR, CRP (unless secondary inflammation); no specific markers. | Elevated ESR, CRP; positive Rheumatoid Factor (RF), anti-CCP (RA); HLA-B27 (AS). | Usually normal ESR, CRP; no specific markers. | Usually normal ESR, CRP; no specific markers. |
| Risk Factors | Age, obesity, previous trauma, developmental abnormalities (e.g., DDH, FAI), genetic predisposition. | Autoimmune conditions, genetic predisposition. | Steroid use, alcohol abuse, trauma, sickle cell disease, Gaucher's disease, Caisson's disease, coagulopathies. | Bony morphology of femoral head/neck or acetabulum; high-level athletics. |
| Definitive Diagnosis | Clinical presentation + characteristic radiographic findings. | Clinical presentation + lab markers + characteristic radiographic findings; biopsy if necessary. | MRI (early detection of marrow edema, necrosis); eventually X-rays. | Radiographs (AP pelvis, Dunn lateral), MRI for chondrolabral pathology; CT for 3D bony morphology. |
Surgical Decision Making & Classification
The decision for bilateral simultaneous Total Hip Arthroplasty (THA) was made based on several factors:
Indications for THA:
* Severe bilateral hip pain significantly impacting quality of life and functional independence, refractory to comprehensive non-operative management (NSAIDs, physiotherapy, activity modification, intra-articular injections).
* Radiographic evidence of end-stage bilateral hip osteoarthritis (Kellgren-Lawrence Grade IV bilaterally).
* Significant functional impairment including antalgic gait, restricted ROM, and difficulty with activities of daily living.
Rationale for Bilateral Simultaneous THA:
*
Patient Profile:
The patient was otherwise healthy for his age, with well-controlled comorbidities (ASA II), and motivated for a single surgical event and rehabilitation period. Younger, healthier patients with severe bilateral disease are generally good candidates for simultaneous THA.
*
Efficiency:
A single anesthetic exposure, hospital stay, and rehabilitation period can be advantageous for patient convenience and potentially cost-effectiveness.
*
Functional Gains:
Rapid and symmetrical improvement in gait and function, avoiding compensatory gait patterns associated with staged procedures.
*
Risk-Benefit Analysis:
While simultaneous THA is associated with higher risks of blood loss, DVT/PE, and operative time compared to unilateral THA, the benefits in a carefully selected patient often outweigh these, particularly when performed in centers with established protocols for managing these risks. The patient was thoroughly counselled on these risks.
Choice of Uncemented Monobloc Components:
*
Uncemented Fixation:
Chosen for its potential for long-term biological fixation, particularly in a patient of this age with good bone quality. It aims for direct bony ingrowth into the porous-coated surfaces, offering durable fixation and avoiding issues associated with cement mantle failure.
*
Monobloc Acetabular Shell:
This design implies a single-piece acetabular component (metal shell with an integrated bearing surface, or a porous-coated shell receiving a liner). In this case, it refers to a porous-coated metal shell designed for biological fixation, into which a polyethylene or ceramic liner is inserted. The term "monobloc" often refers to shells without modular screw holes, relying solely on press-fit and equatorial locking. We planned for a porous-coated shell with optional screw fixation for additional primary stability if required, paired with a ceramic femoral head and highly cross-linked polyethylene liner.
*
Femoral Stem:
An uncemented, tapered, extensively porous-coated titanium alloy stem was selected, designed for metaphyseal and diaphyseal fit, relying on biological ingrowth.
*
Bearing Surface:
Ceramic-on-polyethylene (CoP) was chosen, offering excellent wear characteristics and reduced risk of osteolysis compared to metal-on-polyethylene (MoP), especially in an active patient. Ceramic-on-ceramic (CoC) was discussed but CoP was chosen for potentially lower fracture risk.
Classification:
*
Osteoarthritis Severity:
Kellgren-Lawrence Grade IV bilaterally.
*
ASA Physical Status:
ASA II, suitable for elective major surgery.
Surgical Technique / Intervention
The procedure involved simultaneous bilateral total hip arthroplasty, performed by two attending surgeons concurrently, each operating on one hip. This approach optimizes operative time and minimizes overall anesthetic exposure while ensuring meticulous execution.
Pre-operative Preparation:
*
Anesthesia:
General endotracheal anesthesia combined with an epidural catheter for post-operative analgesia.
*
Patient Positioning:
The patient was positioned supine on a specialized fracture table (e.g., Hana table) to facilitate both direct anterior approaches. Both legs were prepped and draped freely to allow for intraoperative leg length assessment and manipulation. A sterile field encompassing both hips was created.
*
Antibiotic Prophylaxis:
Intravenous Cefazolin 2g was administered 30 minutes prior to incision, with repeat doses for prolonged surgery.
*
DVT Prophylaxis:
Mechanical compression devices (sequential compression devices, SCDs) were applied to the lower extremities pre-operatively and continued post-operatively.
Surgical Approach (Direct Anterior Approach - DAA):
The direct anterior approach was chosen due to its muscle-sparing nature, which can facilitate early mobilization and potentially reduce dislocation rates in experienced hands.
- Incision: A bikini incision (transverse) or longitudinal incision centered over the anterior superior iliac spine (ASIS) was made for both hips.
- Interval: The superficial fascia was incised. The interval between the sartorius (femoral nerve innervation) and tensor fascia lata (superior gluteal nerve innervation) was identified. The ascending branch of the lateral circumflex femoral artery and vein were ligated or cauterized.
- Capsulotomy: The direct head of the rectus femoris was retracted medially. The hip joint capsule was identified and an H-shaped or T-shaped capsulotomy was performed.
-
Femoral Head Osteotomy: With the hip dislocated anteriorly, a controlled osteotomy of the femoral neck was performed, typically 1 finger breadth proximal to the lesser trochanter, ensuring appropriate neck length preservation. The femoral head was then removed.

Figure 4: Intraoperative view during femoral head removal in direct anterior approach. -
Acetabular Preparation:
- Specialized retractors were used to expose the acetabulum.
- The acetabular labrum and osteophytes were meticulously débrided.
- Serial reaming of the acetabulum was performed using progressively larger hemispherical reamers until healthy subchondral bone was exposed, ensuring an anatomic and stable bed for the acetabular component. Reaming was performed to an undersized diameter (typically 1-2mm less than the final shell size) to ensure a secure press-fit.
- Acetabular component templating was confirmed.
-
Uncemented Monobloc Acetabular Shell Implantation:
A porous-coated, hemispherical acetabular shell was impacted into the prepared acetabulum at an ideal inclination (40-45°) and anteversion (15-20°). Initial press-fit stability was verified.

Figure 5: Intraoperative image showing preparation of the acetabulum and impaction of the uncemented monobloc shell. - Multiple fixation screws were inserted through designated holes in the shell (if present in the chosen monobloc design) to augment primary stability, particularly superiorly and postero-superiorly.
- The highly cross-linked polyethylene liner was then locked into the acetabular shell.
-
Femoral Preparation:
- The femur was prepared using an anterior femoral elevator and external rotation/extension to expose the femoral canal.
- The femoral canal was broached sequentially, starting with smaller broaches and progressing to the size determined by pre-operative templating, until cortical contact was achieved, ensuring appropriate version.
-
Uncemented Femoral Stem Implantation:
The final uncemented, tapered titanium alloy femoral stem was then impacted into the prepared femoral canal, achieving stable metaphyseal and diaphyseal fixation.

Figure 6: Intraoperative image demonstrating femoral canal preparation with broaches prior to stem implantation.

Figure 7: Uncemented femoral stem being impacted into the prepared femoral canal.
-
Trial Reduction & Stability Assessment:
- Trial femoral heads of varying neck lengths (e.g., -3.5mm, 0mm, +3.5mm) were used with the trial liner.
- Each hip was reduced. Leg length, offset, and stability in various planes (flexion, extension, internal/external rotation, abduction, adduction) were meticulously assessed. The goal was to equalize leg lengths to within 5mm and achieve a stable construct without impingement in the physiological range of motion.
- The contralateral hip status was continuously monitored during trial reductions to ensure no inadvertent dislocation or impingement.
-
Final Component Implantation:
- Once optimal leg length, offset, and stability were confirmed, the final ceramic femoral head (e.g., 32mm) was affixed to the femoral stem taper.
- Final reduction was performed.
- The stability of both hips was re-checked comprehensively.
-
Closure:
- The hip capsule was repaired (if feasible and desired) using non-absorbable sutures to enhance stability.
- Layered closure of the deep fascia, subcutaneous tissue, and skin was performed. No drains were used.
- Sterile dressings were applied.
Post-Operative Radiographs:
An AP pelvis and lateral hip radiographs were obtained in the recovery room.
*
AP Pelvis (Figure 8):
* Confirmed excellent positioning of both acetabular components (inclination 43° right, 42° left; anteversion visually appropriate).
* Femoral stem position was anatomical, centered in the canal, with appropriate version.
* Leg lengths appeared equal.
* Restoration of hip offset was satisfactory.
* No evidence of periprosthetic fracture or dislocation.

Figure 8: Post-operative AP Pelvis radiograph demonstrating well-positioned bilateral THA components.
Post-Operative Protocol & Rehabilitation
Immediate Post-Operative (Day 0-3):
*
Pain Management:
Epidural analgesia was continued for 24-48 hours, supplemented with multimodal oral analgesia (acetaminophen, gabapentin, NSAIDs where appropriate, opioid sparingly).
*
DVT Prophylaxis:
Continued SCDs. Initiated chemical prophylaxis with low molecular weight heparin (LMWH) at 12-24 hours post-op, continued for 4-6 weeks.
*
Blood Management:
Hematocrit and hemoglobin monitored. No blood transfusion was required for this patient, but a low threshold for transfusion is maintained for simultaneous THA.
*
Weight Bearing:
Immediate full weight-bearing as tolerated (FWBAT) was allowed on both lower extremities, consistent with uncemented components and DAA.
*
Physical Therapy (PT):
Initiated on post-operative day 0 or 1.
* Focus on gentle ROM exercises, ankle pumps, quad sets, gluteal sets.
* Instruction on transfer techniques (bed to chair) and safe ambulation with a walking aid (walker, then crutches).
* Emphasis on maintaining hip precautions (avoiding excessive flexion, adduction past midline, and internal rotation if a posterior approach was used – though less critical for DAA, still prudent in early stages).
Early Rehabilitation (Weeks 1-6):
*
Hospital Discharge:
Typically on post-operative day 2-4, once pain is controlled, patient is mobile with walking aid, and independent with basic ADLs.
*
Outpatient PT:
Regular sessions (2-3 times per week) with a focus on:
* Progressive strengthening of hip abductors, extensors, and core musculature.
* Gait training to normalize pattern and reduce reliance on walking aids.
* Improvement of hip ROM within safe limits.
* Endurance training.
*
Home Exercise Program (HEP):
Patient compliance with daily HEP is crucial.
*
Driving:
Permitted once pain is controlled and patient off opioid medications, typically 4-6 weeks post-op for right leg/automatic vehicle.
Intermediate to Long-Term Rehabilitation (Weeks 7-12 and beyond):
*
Progressive Loading:
Gradual increase in activity levels.
*
Advanced Strengthening:
Incorporate resistance bands, light weights.
*
Balance and Proprioception Training:
Essential for fall prevention.
*
Return to Activities:
Most patients return to light recreational activities (e.g., walking, swimming, cycling) by 3 months. Impact sports or activities requiring extreme hip motion are generally discouraged.
*
Follow-up:
Clinical and radiographic follow-up at 6 weeks, 3 months, 6 months, 1 year, then annually.
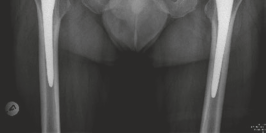
Figure 9: Patient ambulating independently with a cane during early rehabilitation.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls:
- Patient Selection for Bilateral Simultaneous THA: Ideal candidates are motivated, medically optimized (ASA I or II), younger (<70-75 years), with significant bilateral symptoms. Rigorous pre-operative medical clearance, including cardiac and hematological assessment, is paramount.
- Meticulous Pre-operative Templating: Essential for accurate component sizing, restoration of leg length, offset, and hip biomechanics. Use calibrated radiographs and potentially CT scans for complex cases. Templating guides surgical execution and minimizes intraoperative surprises.
-
Blood Management Strategy:
Simultaneous bilateral THA carries a higher risk of blood loss. Implement a multimodal strategy:
- Tranexamic Acid (TXA): Administer pre-incision and potentially intra-articularly to reduce perioperative blood loss.
- Intraoperative Cell Salvage: Consider for high-risk patients.
- Hypotensive Anesthesia: Judicious use to reduce bleeding.
- Optimize Hemoglobin: Address pre-operative anemia.
- DVT/PE Prophylaxis: Aggressive multimodal prophylaxis is crucial for simultaneous procedures due to increased risk. This includes mechanical (SCDs) and chemical (LMWH, factor Xa inhibitors) prophylaxis for an extended duration.
- Leg Length and Offset Restoration: Critical for patient satisfaction, biomechanics, and long-term implant survival. Utilize intraoperative tools (e.g., calipers, specific DAA leg length assessment tools, or direct visualization on a fracture table) to ensure accuracy.
- Surgical Team Coordination: If two surgeons are operating concurrently, seamless coordination and communication are vital to maintain sterility, ensure efficient workflow, and manage potential complications.
- Appropriate Component Selection: Uncemented monobloc components are excellent choices for younger, active patients with good bone stock, aiming for durable biological fixation and longevity. Consider ceramic-on-polyethylene or ceramic-on-ceramic bearings for low wear rates.
Pitfalls:
-
Increased Morbidity/Mortality (Compared to Unilateral THA):
- Higher Blood Loss and Transfusion Rates: Can lead to increased risk of infection, longer hospital stay, and transfusion reactions.
- Increased Risk of DVT/PE: Due to prolonged immobility and larger surgical trauma.
- Longer Operative Time and Anesthetic Exposure: Can contribute to perioperative complications, particularly in elderly or medically fragile patients.
- Higher Risk of Periprosthetic Joint Infection (PJI): Though absolute risk remains low, any increase is a significant concern.
-
Nerve Injuries:
- Lateral Femoral Cutaneous Nerve (LFCN) Palsy: Common with the DAA due to its superficial course. Usually transient but can cause bothersome dysesthesia.
- Femoral Nerve Palsy: Rare but devastating. Can occur from direct injury, prolonged retraction, or hematoma.
- Sciatic Nerve Palsy: Also rare, often related to leg lengthening or posterior retraction.
- Dislocation: While the DAA may have a lower early dislocation rate, it is still a significant complication. Careful attention to component position (inclination, anteversion), soft tissue tension, and avoidance of impingement is essential.
- Periprosthetic Fracture: Can occur intraoperatively (during reaming or stem impaction) or post-operatively. Meticulous bone preparation and appropriate force application are key.
- Heterotopic Ossification (HO): Particularly common with DAA. Consider prophylaxis (NSAIDs or low-dose radiation) for high-risk patients.
- Component Malposition: Leading to impingement, instability, accelerated wear, or limb length discrepancy. Emphasize meticulous technique and intraoperative checks.
- Technical Challenges of DAA: Steep learning curve, limited exposure for the femur, and risk of anterior cortical perforation during femoral preparation. Experience with the approach is critical.
Clinical & Radiographic Imaging

